
Abstract
Objective
To investigate the clinical significance of serum S100 calcium-binding protein A10 (S100A10) levels in lung cancer.
Methods
This prospective study enrolled patients with lung cancer, patients with benign lung nodules and healthy control subjects. Serum S100A10 levels and three biomarkers were measured and compared between the groups. Associations between serum S100A10 and clinical characteristics in patients with lung cancer were investigated. The diagnostic efficacy of serum S100A10 and carcinoembryonic antigen for lung cancer was calculated.
Results
The study enrolled 82 patients with lung cancer, 21 with benign lung nodules and 50 healthy controls. Serum S100A10 levels were significantly higher in patients with lung cancer compared with patients with benign lung nodules and healthy control subjects. Serum S100A10 levels of patients with advanced lung cancer were significantly higher than those with early stage disease. Patients with lymph node metastases had significantly higher serum S100A10 levels than patients without lymph node metastases. The cut-off serum S100A10 value for lung cancer detection was 1.34 ng/ml, which had a sensitivity of 48.2%, a specificity of 76.2% and an area under the curve of 0.63.
Conclusion
Serum S100A10 was significantly correlated with disease stage and lymph node metastasis. It has the potential to be a tumour biomarker for lung cancer.
Introduction
Lung cancer is a common cancer and approximately 80% of cases are non-small-cell lung cancer (NSCLC). 1 Despite multidisciplinary efforts to improve the clinical outcomes of lung cancer, it is still the leading cause of cancer-related mortality worldwide. 1 The low rate (<25%) of early diagnosis of lung cancer is the key reason for its high mortality rate. 2 Low-dose computed tomography (LDCT) has been used in screening for lung cancer, resulting in a reduction of the mortality rate by 20%. 3 However, high false positivity is the major drawback of LDCT. 3 Although serum tumour markers such as carcinoembryonic antigen (CEA), squamous cell carcinoma antigen (SCC) and cytokeratin 19 fragment (Cyfra21-1) are widely used for lung cancer diagnosis in clinical practice, they lack sufficient sensitivity and specificity. 4 Thus, new potential markers for the early diagnosis of lung cancer are urgently needed.
S100 calcium-binding protein A10 (S100A10), as a member of the S100 family, regulates a range of biological functions such as maintenance of cell motility, phosphorylation and transduction pathway signaling. 5 Previous reports have indicated that S100A10 acts as an oncoprotein in ovarian cancer, gastric cancer, breast cancer and renal cell cancer.6–9 In lung cancer, S100A10 is likely involved in the progression of invasion and metastasis through regulation of plasmin production and subsequent plasmin-dependent stimulation of matrix metalloproteinase (MMP)-2 and MMP-9. 10 A previous report demonstrated that S100A10 tissue levels were higher in cancer tissues. 11 However, the relationship between serum S100A10 and lung cancer has not yet been reported. This study aimed to investigate the clinical significance of serum S100A10 in lung cancer with a view to providing a new tumour biomarker for lung cancer.
Patients and methods
Patients and specimens
This prospective study enrolled consecutive patients with lung cancer and consecutive patients with benign lung nodules in the Department of Cardiothoracic Surgery, The First Affiliated Hospital of Chongqing Medical University, Chongqing, China between January 2021 and April 2021. Venous blood samples (2.0 ml) were collected from the patients and from 50 healthy control subjects that attended a clinic for a routine examination at the Health Management Centre, The First Affiliated Hospital of Chongqing Medical University, Chongqing, China. The healthy control subjects were age and sex matched to the patients. Each blood sample was separated by centrifugation at 2000 ×
The study was approved by the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University (no. 2021-493). The study participants provided written informed consent. The reporting of this study confirms with STROBE guidelines. 13
Serum S100A10 and tumour markers measurement
Serum S100A10 levels were quantified using an enzyme-linked immunosorbent assay (ELISA) kit (CSB-EL020623HU; Wuhan CUSABIO, Hubei, China). With regard the reference data for the S100A10 ELISA kit, the regression equation for the standard curve was as follows: y = 10.118x–0.8064, R2 = 0.9952. The performance parameters of the S100A10 ELISA kit are summarized as follows: intra-assay coefficient of variation <8%, inter-assay coefficient of variation <10%, detection range 0.312–20 ng/ml.
Serum SCC, Cyfra21-1 and CEA levels were measured using electrogenerated chemiluminescence immunoassays (cobas® e 602 module; Roche Diagnostics, Mannheim, Germany). The minimum detectable concentrations were 0.078 ng/ml for S100A10, 0.1 ng/ml for SCC, 0.2 ng/ml for Cyfra21-1 and 0.2 ng/ml for CEA.
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 13.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Serum S100A10 levels are presented as median (interquartile range). Mann–Whitney U-test was used to compare the results between groups. Receiver operating characteristic (ROC) curves were used to determine the area under the curve (AUC) and sensitivity and specificity of serum S100A10 and serum CEA for lung cancer. According to the reference, the total AUC was an overall summary of the diagnostic accuracy as follows: AUC > 0.9 indicates excellent diagnostic accuracy; AUC between 0.71 and 0.9 indicates good diagnostic accuracy; AUC between 0.5 and 0.7 indicates poor diagnostic accuracy; AUC < 0.5 indicates the lack of diagnostic value of the biomarker. 14 A P-value <0.05 was considered statistically significant.
Results
This prospective study enrolled 82 patients with lung cancer and 21 patients with benign lung nodules. Of the 82 patients with lung cancer (mean ± SD age, 59.3 ± 9.6 years), 51 were male (62.2%) and 31 were female (37.8%). According to TNM clinical staging, 48 patients (58.5%) were in the early stage (I or II) and 34 patients (41.5%) were in the advanced stage (III or IV). Thirty-two of 82 patients (39.0%) had lymph node metastases. The demographic and clinical characteristics of the patients with lung cancer are summarized in Table 1. Of the 21 patients with benign lung nodules (mean ± SD age, 53.2 ± 8.6 years), 12 were male (57.1%) and nine were female (42.9%). Blood samples were also collected from 50 healthy control subjects (25 males, 25 females; mean ± SD age, 56.1 ± 7.8 years).
Demographic and clinical characteristics of patients with lung cancer (n = 82) that were included in this prospective study of the clinical significance of serum S100 calcium-binding protein A10 (S100A10) levels in lung cancer.

Data presented as n of patients (%).
aData from some patients were missing.
Serum S100A10 levels were significantly higher in patients with lung cancer than in the healthy control subjects and patients with benign lung nodules (median [interquartile range] 1.27 [0.9–1.72] ng/ml versus 1.13 [0.75–1.37] ng/ml, P = 0.018; 1.27 [0.9–1.72] ng/ml versus 1.04 [0.76–1.28] ng/ml, P = 0.039], respectively) (Figure 1). Significantly higher serum CEA levels were also found in patients with lung cancer than in the healthy control subjects and patients with benign lung nodules (median [interquartile range] 2.59 [1.59–4.69] ng/ml versus 2.15 [1.43–3.10] ng/ml, P = 0.03; 2.59 [1.59–4.69] ng/ml versus 1.8 [1.6–2.3] ng/ml, P = 0.023], respectively). No significant differences were found between the three groups in terms of serum Cyfra21-1 and SCC levels (median Cyfra21-1 [interquartile range] 3.20 [2.00–6.00] ng/ml versus 2.20 [1.84–3.55] ng/ml versus 2.20 [1.85–3.15] ng/ml, respectively; median SCC [interquartile range] 1.00 [0.80–1.40] ng/ml versus 1.02 [0.79–1.4] ng/ml versus 1.30 [0.80–1.60] ng/ml, respectively).

Levels of serum S100 calcium-binding protein A10 (S100A10) and three tumour markers in the three groups of study participants: patients with lung cancer (n = 82), patients with benign lung nodules (n = 21) and healthy control subjects (n = 50). (a) S100A10; (b) carcinoembryonic antigen (CEA); (c) cytokeratin 19 fragment (Cyfra21-1); (d) squamous cell carcinoma antigen (SCC). The colour version of this figure is available at: http://imr.sagepub.com.
Significantly higher serum S100A10 levels were found in patients with lung cancer at the more advanced stages than those in the early stages (median [interquartile range] 1.65 [1.20–1.76] versus 1.12 [0.75–1.45] ng/ml, respectively, P < 0.01) (Figure 2). Patients with lymph node metastases showed significantly higher S100A10 levels than patients without lymph node metastases (median [interquartile range] 1.47 [1.21–1.75] versus 1.07 [0.76–1.40] ng/ml, respectively, P < 0.01). No significant differences in serum S100A10 levels between squamous cell carcinoma and adenocarcinoma were found (median [interquartile range] 1.52 [1.10–1.73] ng/ml versus 1.27 [0.85–1.69] ng/ml, respectively). Serum S100A10 levels in patients with tumour size >1 cm and tumour size ≤1 cm were not significantly different (median [interquartile range] 1.35 [1.00–2.42] ng/ml versus 1.15 [0.90–2.00] ng/ml, respectively).
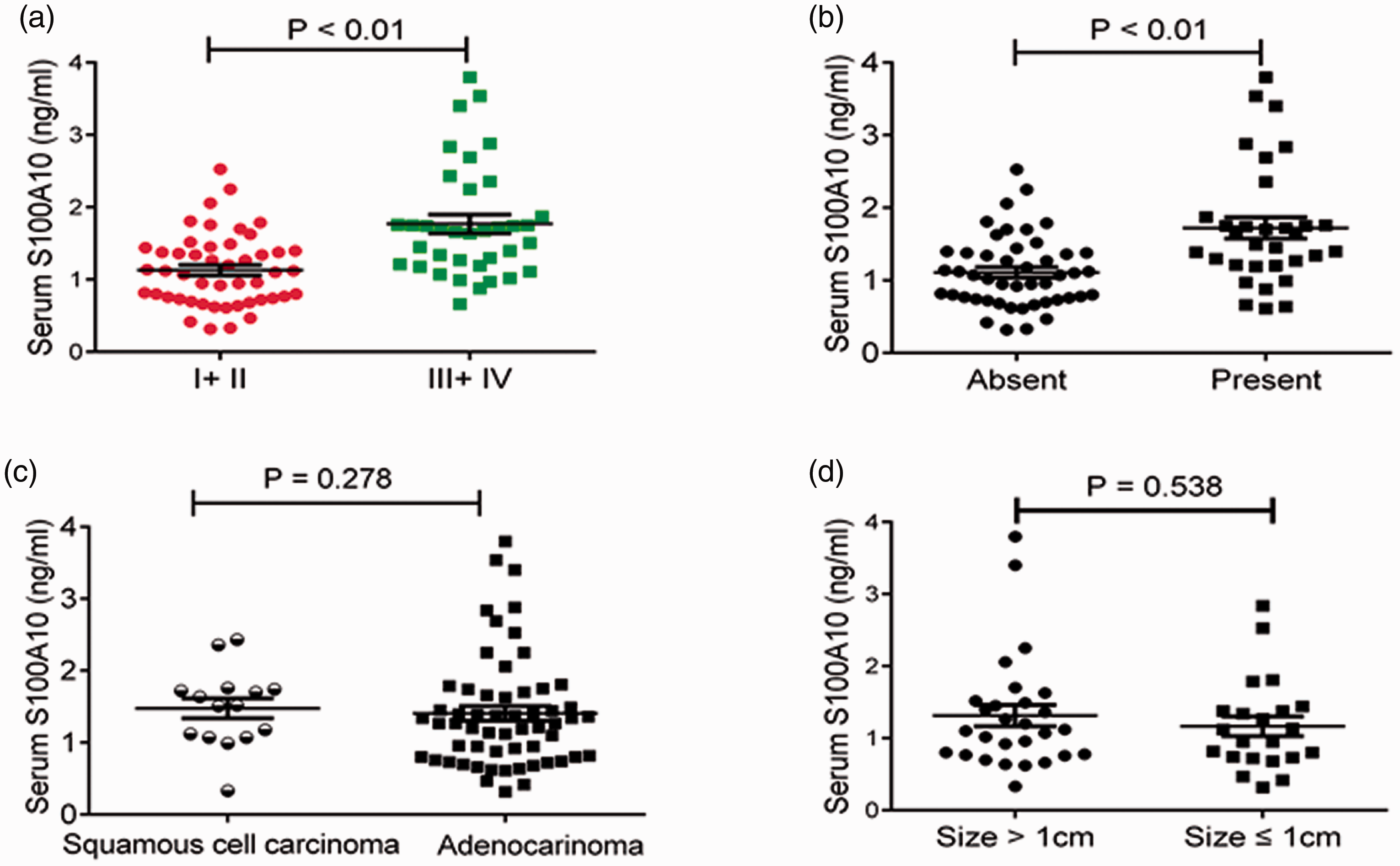
Relationship between the levels of serum S100 calcium-binding protein A10 (S100A10) and clinical characteristics in patients with lung cancer (n = 82): (a) Tumor–Node–Metastasis (TNM) stage; (b) lymph node metastasis; (c) histological type; (d) tumour size. The colour version of this figure is available at: http://imr.sagepub.com.
The ROC curve analysis for serum S100A10 for diagnosing lung cancer had an AUC of 0.63 (95% confidence interval [CI] 0.54, 0.72) (Figure 3). Youden’s index was calculated to set an optimum cut-off value of 1.34 ng/ml with a sensitivity of 48.2% and a specificity of 76.2%. The AUC of serum CEA for lung cancer was 0.62 (95% CI 0.53, 0.71) with a sensitivity of 42.2% and a specificity of 86.2%. Using a combination of serum S100A10 and serum CEA for lung cancer diagnosis produced an AUC of 0.67 (95% CI 0.59, 0.76) with a sensitivity of 36.1% and a specificity of 96.9%.
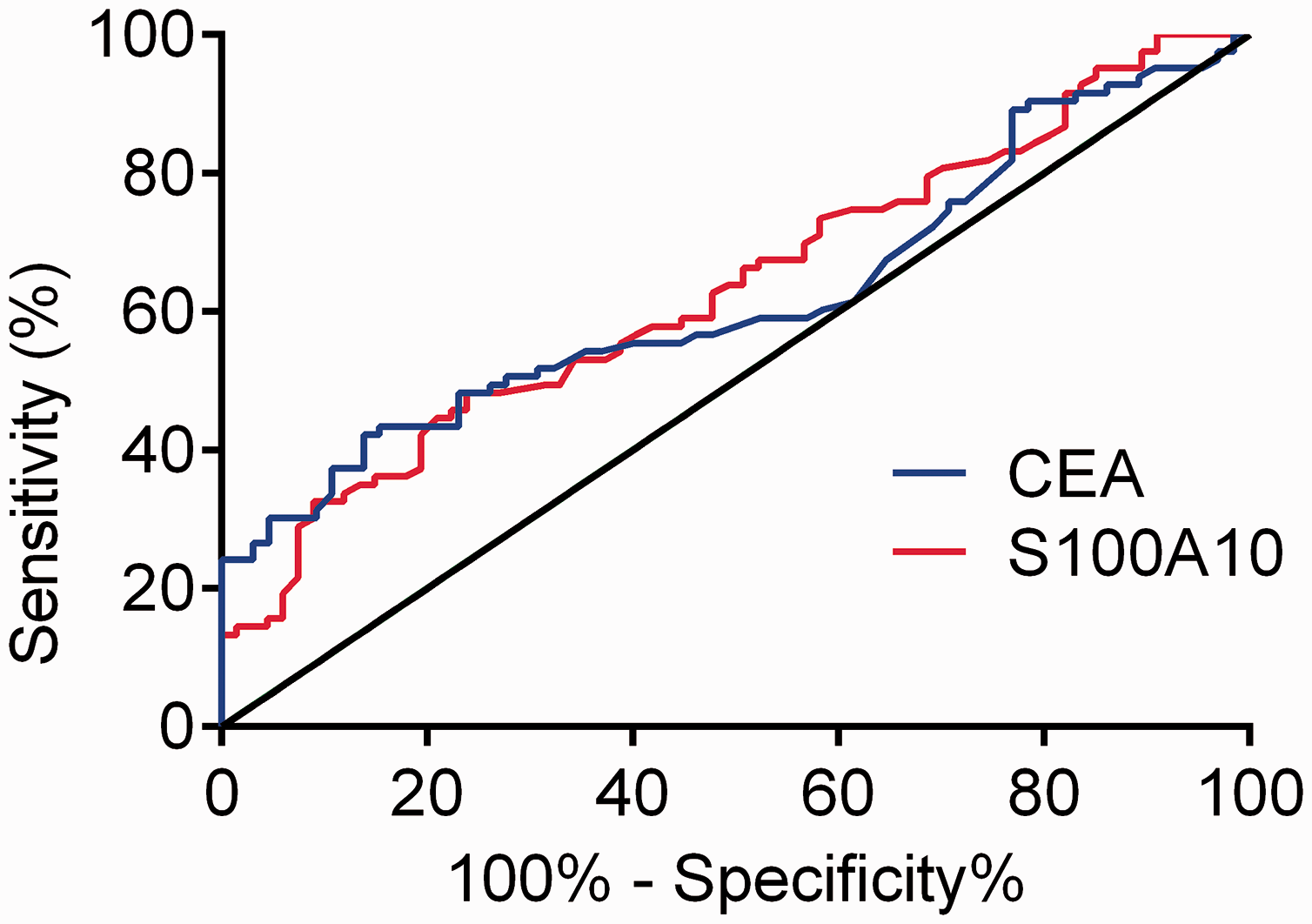
Diagnostic efficacy of serum S100 calcium-binding protein A10 (S100A10) and carcinoembryonic antigen (CEA) for lung cancer. The colour version of this figure is available at: http://imr.sagepub.com.
Discussion
The findings of this current study demonstrated that serum S100A10 levels were significantly higher in patients with lung cancer than in those with benign lung nodules and healthy control subjects. Previous reports have indicated that S100A10 expression was increased in leukaemia, colorectal cancer and melanoma.15–17 In pancreatic ductal adenocarcinoma, S100A10 has been found to be overexpressed in tumours when compared with normal ducts and nonductal stroma; 18 and S100A10 expression was upregulated in lung cancer tissue. 11 These findings are in accordance with those of the current study and suggest that serum S100A10 might be marker for lung cancer.
An ideal tumour marker is associated with clinical characteristics. 19 These current results demonstrated that serum S100A10 levels were associated with tumour TNM stage and lymph node metastasis. In lung cancer, S100A10 participates in metastasis through regulation of plasmin production and subsequent plasmin-dependent stimulation of MMP-2 and MMP-9. 10 MMPs are capable of the degradation of the extracellular matrix and basement membrane, a critical step in tumour progression. 10 S100A10 has been found to be correlated to histological subtype, histological grade and International Federation of Gynecology and Obstetrics stage in epithelial ovarian cancer. 20 In addition, univariate Cox regression analysis indicated that S100A10 was correlated with short overall survival. 20 In a study of breast cancer, S100A10 expression was significantly elevated in high-grade, triple-negative tumours and tumours with a high proliferative index. 8 In a study of lung squamous cell carcinoma tissue, S100A10 levels were significantly associated with higher TNM stage, tumour size, lymphatic invasion and lymph node metastasis. 11 The results of these studies were consistent with literature reporting that serum S100A10 is related to cancer characteristics. 17
Serum CEA, Cyfra21-1 and SCC are widely used for lung cancer diagnosis in clinical practice, but their diagnostic efficacy is limited. 21 ROC curve analysis is the most useful tool for evaluating diagnostic efficacy. The AUC ranges from 0.5–1.0, with values close to 1 indicating a high diagnostic efficacy. In the present study, the AUC (0.63) for S100A10 and the AUC (0.62) for CEA in lung cancer diagnosis indicated that the diagnostic accuracy was unsatisfactory. When serum S100A10 and serum CEA were combined for lung cancer detection, the AUC was increased to 0.67 with a sensitivity of 36.1% and a specificity of 96.9%. The diagnostic values were similar for serum CEA and serum S100A10 levels. Although serum CEA is a tumour biomarker for lung cancer in the clinic, its specificity is not strong and its sensitivity is not high. 4 Thus, serum S100A10 might be useful as a complementary marker for CEA in lung cancer.
In conclusion, elevated serum S100A10 levels in lung cancer correlated positively with TNM stage and lymph node metastasis, suggesting that serum S100A10 level has the potential to be a tumour biomarker for lung cancer.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the National Nature Science Foundation of China (no. 81972011) and the Chongqing Health Commission (no. 2021MSXM095, no. 2020MSXM009).