
Abstract
Cerebral sinus venous thrombosis (CSVT) is a rare form of venous thromboembolism. Recurrent transient ischemic attacks were extremely rare clinical manifestation of CSVT. We reported a case of transient ischemic attack as an exceptionally rare form of CSVT. A 29-year-old woman presented with a headache and four episodes of a transient right limb weakness, numbness, and dysphasia lasting approximately 15 mins over the course of 2 weeks. Magnetic resonance venography revealed a superior sagittal sinus thrombosis with numerous prominent enlarged and dilated venous. Magnetic resonance imaging revealed venous infarction of the left frontal lobe. Transient ischemic attack-like episodes stopped with anticoagulation. We suggested that the patients with transient ischemic attack and symptoms of increased intracranial pressure should be carefully investigated in terms of CSVT.
Introduction
Cerebral sinus venous thrombosis (CSVT) is a rare form of venous thromboembolism. The most common presentations of CSVT include headache, reduced visual acuity, papilledema, focal neurological deficits, seizures, and diffuse encephalopathy. 1 The unusual causes of inflammatory vascular lesions and hypercoagulable states could lead to transient ischemic attacks (TIAs). 2 Recurrent TIAs are an extremely rare clinical manifestation of CSVT. TIA cases that are of venous origin and that fit the abovementioned definition have been rarely reported in the PubMed database. To the best of our knowledge, less than 10 cases have been previously reported in the literature.3–9 We presented a patient admitted to the Beijing Chao-Yang Hospital with a diagnose of CSVT presenting as TIA. This case report highlights the importance of identifying recurrent TIA from clinical manifestations of rare CSVT patients.
Case presentation
A 29-year-old woman admitted to our hospital with headache and weakness of the right numb. During the last 5 days, her headache was unresponsive to analgesics; it was persistent distension and pain, sometimes accompanied by dizziness and nausea. On the fourth day, she had right limb weakness with no triggers. The review of systems was negative; she had no history of migraine. The patient disclosed menstrual disturbance and received the treatment of oral contraceptives, ethinyl estradiol, and cyproterone acetate tablets, for 2 months. Family history was noncontributory. On admission, the neurological examination showed that distal muscle strength of the right upper limb was grade 1. Fundus examination indicated bilateral papilledema. Physical examination showed no abnormalities. The preadmission examinations of magnetic resonance imaging (MRI) and magnetic resonance venography (MRV) has confirmed the diagnosis of CSVT. She received treatment of subcutaneous low-molecular-weight heparin administration from the first day of admission. Her distal muscle strength in the right upper limb almost returned to normalcy on the third day. During hospitalization, the patient experienced a total of four episodes of slurring of speech, right-sided upper limb weakness, and numbness, lasting 15 min without any lapses of consciousness.
Cranial computerized tomography (CT) showed the direct sign of CSVT: dense triangle. The brain MRI revealed hyperintensities in the left frontal lobe cortex on fluid attenuated inversion recovery (FLAIR) and T2-weighted image, a dilation and thickening of subcortical veins caused by venous thrombosis on susceptibility weighted imaging. Magnetic resonance angiography of the cerebral arterial vessels were unremarkable, while MRV detected superior sagittal sinus thrombosis (Figure 1). CT perfusion showed perfusion deficits of the left frontal lobe cortex (Figure 2). Electroencephalography did not reveal any epileptic abnormalities.
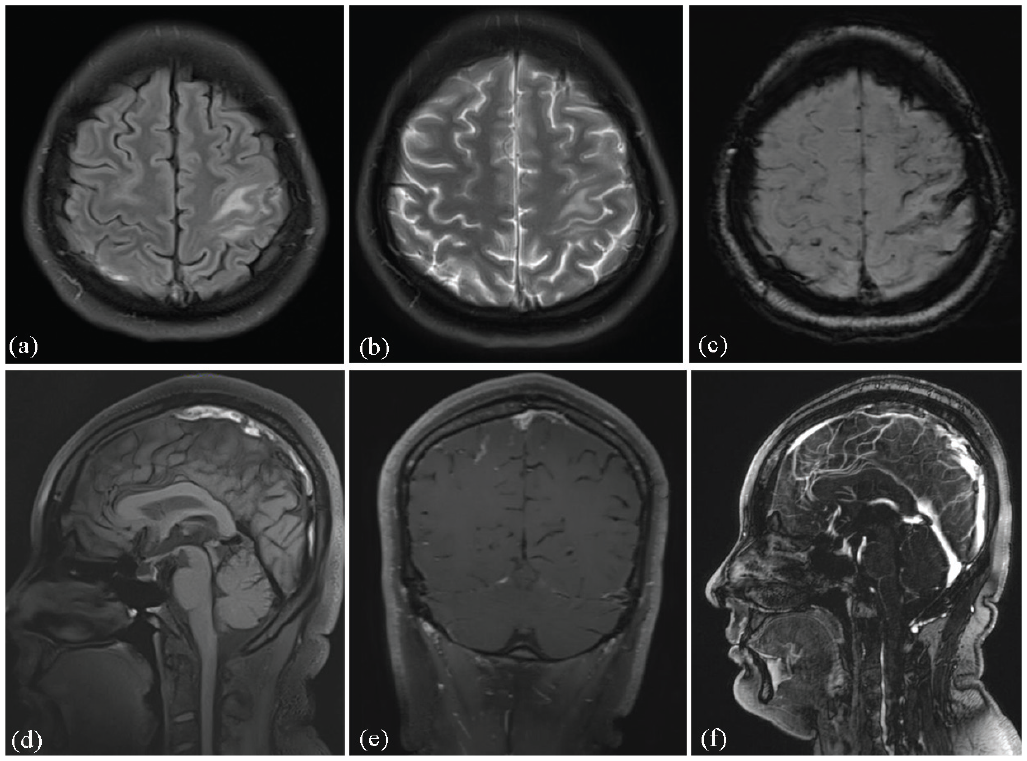
(a) Axial FLAIR images revealed a hyperintense lesion on the left frontal cortex. (b) Axial T2-weighted image showed a hyperintense lesion on the left frontal cortex. (c) Axial susceptibility weighted imaging revealed thickening and dilation of cortical veins. (d) Sagittal T1-weighted image showed thrombosis of the superior sagittal sinus. (e) Coronal T1 with gadolinium image. (f) Sagittal MRV revealed superior sagittal sinus thrombosis.

CT perfusion revealed perfusion deficits of the left frontal cortex. (a) Normal cerebral blood volume (CBV), (b) decreased cerebral blood flow (CBF), (c) delayed mean transit time, and (d) delayed time to peak.
Laboratory data discovered that D-dimer quantification was 3.84 mg/L (normal range (nr), ⩽0.55 mg/L), C-reactive protein level was 20.24 mg/L (nr: 0–10), and erythrocyte sedimentation rate was 25 mm/h (nr: 2–15). Autoimmune related antibody spectrum results were normal. Detailed laboratory investigations, including hypercoagulability tests as protein C, protein S, and antiphospholipid antibodies were normal. We performed a thorough serological and lumbar puncture to exclude infectious causes of venous thrombosis. The pressure of cerebrospinal fluid (CSF) was 220 mm H2O higher than normal level. Infection-related results were negative. According to the results of auxiliary inspection, other conditions such as vasculitis, cerebral vasospasm, hypercoagulable state, migraine, partial seizures, subarachnoid hemorrhage, and infectious diseases were excluded.
Treatment
Oral contraceptive was the final etiological diagnosis of the patient. Medical treatment included dehydration reducing intracranial pressure, subcutaneous low-molecular-weight heparin administration, and microcirculation improvement. She was discharged on anticoagulant therapy (warfarin) for 3 months. No further attacks presented during hospitalization and at the 1-month follow-up. She received neuroimaging follow-up after 6 months to assess the recanalization of the occluded superior sagittal sinus thrombosis.
Discussion
This CSVT patient presented with four episodes of paroxysmal limb weakness, numbness, and dysphasia, lasting approximately 15 min. The brain CT and MRI scans showed surrounding FLAIR hyperintensity from gyral edema resulting from venous congestion. Electroencephalogram examinations were negative twice. CT perfusion revealed perfusion deficits of left frontal lobe in this patient. Therefore, this patient was diagnosed with venous cerebral infarction and TIA.
The most common form of focal neurological deficits of CSVT is motor weakness, such as mono-paresis, hemiparesis, or bilateral involvement in patients with deep venous system thrombosis. The tendency for the superior sagittal sinus to drain on one side more than the other occurs at the earliest stages in the embryo and proceeds into adulthood. 10 Thrombosis of cerebral venous sinuses could lead to an increase of intracranial pressure and decrease of CSF absorption. This further results in a decrease of cerebral perfusion pressure and metabolic failure, followed by intracellular edema and cytotoxic edema. 8 The pathogenesis of TIA caused by CSVT still remains debatable. In our study, this patient had normal computerized tomography angiography examination results to exclude large artery atherosclerosis but abnormal perfusion deficits of computerized tomography perfusion. Yosuke Takeuchi 9 reported a case with headache and sudden-onset right hemiparesis, which diagnosed with CSVT and confirmed decreased blood flow in frontal lobe. This case reported was similar with our patient. Previous studies reported that cortical spreading depression theory and reduced regional cerebral perfusion could explain the occurrence of TIA in patients with cortical venous thrombosis.3,7 Patients with TIA-like episodes and headache secondary to venous hypertension should be carefully investigated in terms of CSVT. TIA-like episodes usually present motor weakness, and rarely has visual or sensory deficits. 11
Conclusion
Early diagnosis is essential to minimize morbidity and improve survival of patients with CVST. CSVT is a multifactorial disease with different risk factors, such as hereditary conditions, infectious diseases, and drugs. In our case present, oral contraceptives were the initiating cause of CSVT. Anticoagulant treatment, initially with heparin and subsequently with oral anticoagulant is administered for 3 months. TIA-mimic syndrome deserves to be surveyed more carefully and intensively, especially when accompanied by symptoms of increased intracranial pressure, we should consider CSVT.
Footnotes
Acknowledgements
Not applicable.
Author contributions
All authors participated equally in the article preparation and literature review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for her anonymized information to be published in this article.