
Abstract
Objective
To present the clinical characteristics, diagnostics, and treatments for Brucella prostatic abscess (BPA).
Methods
We retrospectively analyzed eight BPA patients according to their vocations, age, clinical manifestations, laboratory test results, magnetic resonance imaging (MRI) findings, and treatments.
Results
The median age was 59 years. The most common clinical symptom was fever, followed by dysuria, erectile dysfunction, frequent urination, and urodynia. C-reactive protein (CRP) concentrations were significantly elevated in all patients, and in all by one patient, the erythrocyte sedimentation rate (ESR) was high. Prostate enlargement occurred in 87.5% of the patients. Lesions were located in the prostate peripheral (87.5%) and central zones (100%), with homogenous signals on T1-weighted imaging (T1WI) and a hyperintense signal on short tau inversion recovery (STIR). Patients had a small nodule or multiple nodules, with slight hyperintense to hyperintense signals on T2-weighted imaging (T2WI) and diffusion-weighted imaging (DWI). Three patients had pelvic effusion, and seminal vesicle (37.5%), epididymis (12.5%), and bladder (12.5%) infections occurred. All patients received rifampicin and doxycycline with levofloxacin; all lesions had resolved at follow-up ultrasonography.
Conclusion
Even in epidemic areas, the incidence of BPA is relatively rare. Our findings may increase the understanding of BPA and reduce misdiagnosis and mistreatment.
Keywords
Introduction
Prostatic abscess has become less common in developed countries, especially among healthy men, owing to awareness of regular inspection and the effective use of antibiotics.1–3 However, the situation differs greatly in developing countries, particularly among groups with immunosuppressive diseases and an increased risk of infection. Historically, prostatic abscess was dangerous, considering its mortality rate, which ranged from 6% to 30%.4,5 The major pathogens in prostatic abscess are gram-negative bacilli (particularly Escherichia coli), which cause approximately 75% of cases of prostatic abscesses during the antibiotic era,6–8 and Brucella spp. are potential pathogens causing prostatic abscess.
Brucella prostatic abscess (BPA) is a unique infectious disease in men. BPA refers to the invasion of Brucella organisms into the prostate, which results in a small abscess and causes urinary system symptoms, such as dysuria, frequent urination, or urodynia. Brucellosis usually involves the bones and joints, particularly the spine;9,10 however, this infection is rare, and only a few BPA cases have been published.11,12 The following reasons explain this lack of published cases. First, the low incidence of brucellosis, even in the osteoarticular system,13,14 makes it easy to misdiagnose or mistreat. Second, the clinical manifestations of brucellosis are non-specific, and BPA is no exception.11,12,15 The great majority of patients with BPA have a low-grade fever, urodynia, and dysuria; there is no specific symptom to distinguish BPA from other urinary tract infections. Third, the pathogenesis is unclear, and some physicians are unaware of the disease. Finally, some patients develop BPA during the follow-up period instead of during the initial acute infection. Consequently, some cases might be misdiagnosed if routine imaging is not performed. In this retrospective study, we discuss the clinical manifestations, laboratory test results and magnetic resonance imaging (MRI) findings, treatments, and prognosis of eight cases of BPA.
Materials and methods
Study population
We retrospectively analyzed the data for all patients diagnosed with BPA in the Xinjiang Medical University Affiliated First Hospital from December 2013 to December 2019. The collected data were the patients’ clinical manifestations, laboratory test results, MRI findings, treatment, and follow-up results. The CONSORT flow diagram of this study is presented in Figure 1. The inclusion criteria were: (a) positive rose Bengal plate test or positive standard tube agglutination test results (≥1:160); 16 (b) positive bacterial culture results; and (c) available follow-up results after treatment. The exclusion criteria were: (a) previous prostatic surgery; (b), cancer or other prostatic diseases; (c) received treatment for BPA before the study; and (d) no MRI of the prostate. The reporting of the study conformed to the STROBE statement, 17 and the study was approved by the Medical Ethics Committee of the first affiliated Hospital of Xinjiang Medical University (approval number: 20160114-111). All patients provided verbal informed consent by phone.

The flow diagram of patient selection.
MRI protocol
All patients underwent pelvic MRI after admission using a 1.5 T MRI unit (Magnetom or Avanto; Siemens, Erlangen, Germany). The MRI protocol was as follows: T1-weighted images (T1WI) were obtained in the axial plane with a repetition time (TR) of 500 ms and echo time (TE) of 11 ms. T2-weighted images (T2WI) were acquired in the axial, sagittal, and coronal planes with TR: 6700 ms and TE: 100 ms. Short tau inversion recovery (STIR) images were obtained in the axial and coronal planes with TR: 4500 ms and TE: 90 ms. Diffusion-weighted images (DWI) were also acquired in the axial plane with TR: 4105 ms; TE: 75 ms; two b values (b0, b1000); and slice thickness: 3 mm with no gap. The field of view (FOV) for all sequences was 240 mm × 240 mm; matrix: 400 × 400.
Statistical methods
Non-normally-distributed continuous data are presented as medians, and categorial data are presented as percentages.
Results
Demographic characteristics
The patients’ demographic characteristics are shown in Table 1; all patients were men. The median age of the patients was 59 years (range: 43–63 years). Half (50%) of all patients were herdsmen; two (25%) worked in commercial kitchens, one (12.5%) was a truck driver, and one (12.5%) was a governmental employee, and 25% had diabetes. All patients had a history of contact with cattle and sheep.
Demographic characteristics and clinical manifestations in brucella prostatic abscess patients
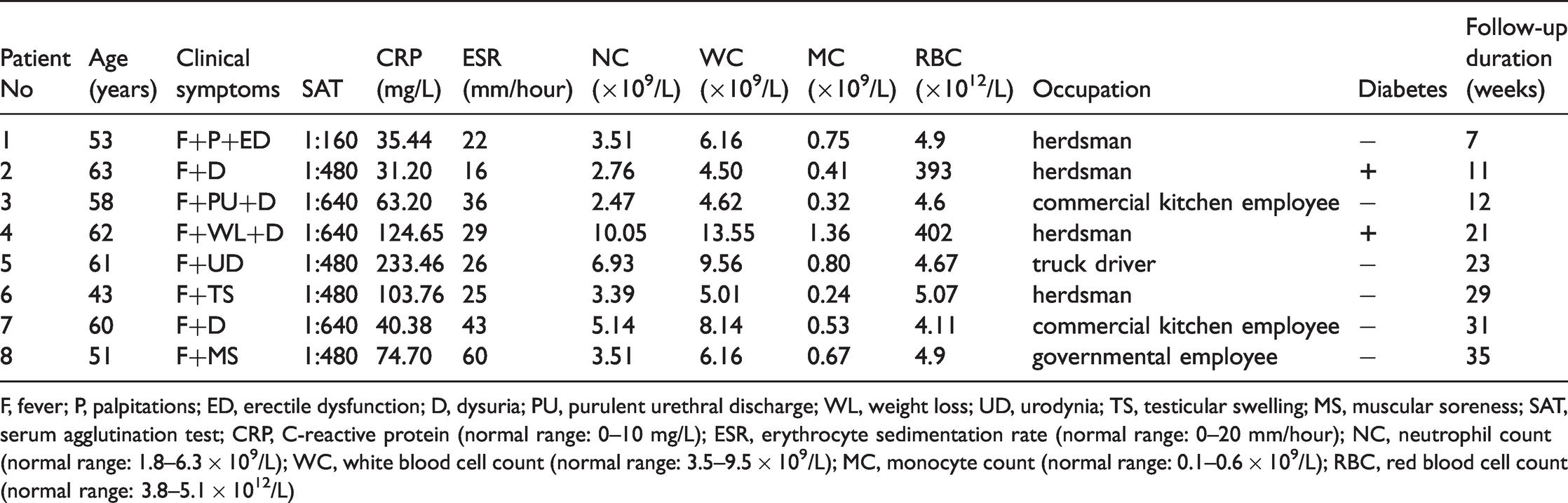
F, fever; P, palpitations; ED, erectile dysfunction; D, dysuria; PU, purulent urethral discharge; WL, weight loss; UD, urodynia; TS, testicular swelling; MS, muscular soreness; SAT, serum agglutination test; CRP, C-reactive protein (normal range: 0–10 mg/L); ESR, erythrocyte sedimentation rate (normal range: 0–20 mm/hour); NC, neutrophil count (normal range: 1.8–6.3 × 109/L); WC, white blood cell count (normal range: 3.5–9.5 × 109/L); MC, monocyte count (normal range: 0.1–0.6 × 109/L); RBC, red blood cell count (normal range: 3.8–5.1 × 1012/L)
Clinical characteristics
The patients’ clinical characteristics are shown in Table 1. All patients had a continuous or intermittent fever, and half had dysuria. The other clinical manifestations were erectile dysfunction, frequent urination, and urodynia.
Laboratory results
The patients’ laboratory data are shown in Table 1. All standard tube agglutination test results were positive (>1:160), and all patients’ C-reactive protein (CRP) concentrations were significantly elevated. In all but one patient, the erythrocyte sedimentation rate (ESR) was increased. Other laboratory data were also elevated, namely the monocyte count (50.0%), neutrophil count (25.0%), red blood cell count (25.0%), and white blood cell count (25.0%). In addition, all patients underwent microbiological or biochemical examinations, such as bacterial culture or immunological tests to rule out tuberculosis; all results were negative.
Imaging findings
The patients’ MRI findings are shown in Table 2. Prostate enlargement occurred in 87.5% of the patients. BPA lesions were present mainly in the prostatic peripheral zone (87.5%) and central zone (100%). All patients showed homogenous signals on T1WI and hyperintense signals on STIR (Figure 2 and Figure 3). All lesions were a small nodule or multiple nodules; 75% of the patients had slightly hyperintense signals on T2WI, and 25% had hyperintense signals on T2WI (Figure 4). Four patients who underwent DWI had slight hyperintense signals (Figure 5). Contrast-enhanced MRI was performed in two patients, which showed mild ring enhancement. Three patients had pelvic effusion, and seminal vesicle (37.5%), epididymis (12.5%), and bladder (12.5%) infections also occurred.
MRI findings in brucella prostatic abscess patients.
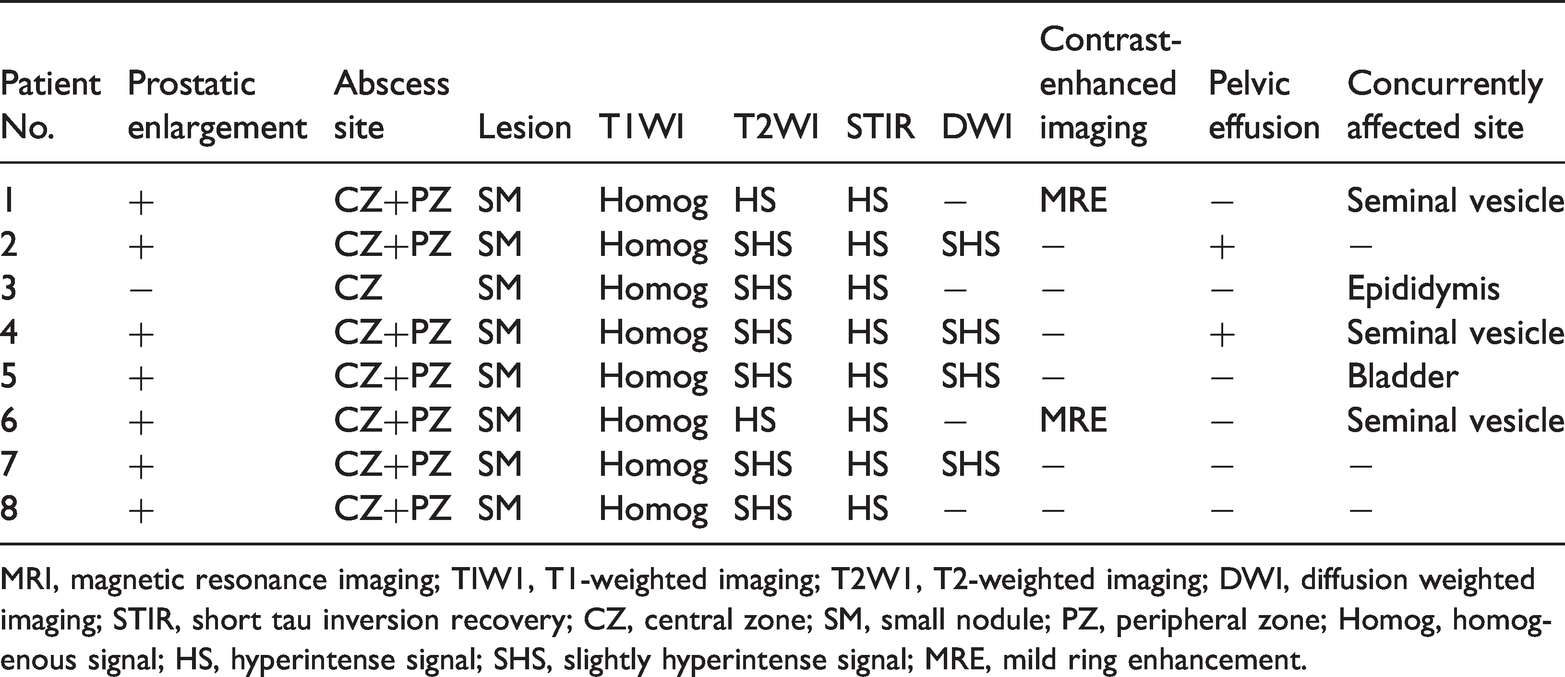
MRI, magnetic resonance imaging; TIW1, T1-weighted imaging; T2W1, T2-weighted imaging; DWI, diffusion weighted imaging; STIR, short tau inversion recovery; CZ, central zone; SM, small nodule; PZ, peripheral zone; Homog, homogenous signal; HS, hyperintense signal; SHS, slightly hyperintense signal; MRE, mild ring enhancement.

Axial MR T1WI demonstrating homogenous signal lesions in the prostate.

Axial MR STIR showing multiple prostatic nodules with hyperintense signals.

Axial MR T2WI showing multiple prostatic nodules with slightly hyperintense signals.
Axial MR DWI showing multiple prostatic nodules of varying size with hyperintense signals.
Treatment and follow-up
The patients’ follow-up results are shown in Table 1. All patients received rifampicin and doxycycline with levofloxacin; 200 mg of doxycycline, 600 mg of rifampicin, and 500 mg of levofloxacin were combined daily for 7 to 65 weeks (average: 12.6 weeks). The clinical symptoms of all patients resolved, and all lesions in the eight patients had disappeared by the end of treatment on follow-up ultrasonography.
Discussion
Brucellosis is a zoonotic allergic disease associated with Brucella spp., a tiny intracellular bacterium, which is present worldwide and may infect any organ.1,11,18 The most vulnerable part of the body regarding brucellosis is the osteoarticular system, followed by the genitourinary system. The incidence of reproductive complications with brucellosis is approximately 1.4%–25%. 12 BPA is a severe urogenital complication that can lead to an enlarged prostate and difficulty urinating, but the condition is quite rare. 19
This study involved the largest number of cases of BPA in China. The median age of the patients was 59 years (range: 43–63 years), and 50% were herdsmen, 25% worked in commercial kitchens, 12.5% were truck drivers, and 12.5% were governmental employees. All patients had a history of exposure to cattle and sheep. Our findings were consistent with the conclusions of Mangalgi et al., 20 who argued that easier exposure to animals resulted in greater susceptibility to brucellosis. People with occupations with increased exposure to animals or animal products may have a high risk of developing BPA. Therefore, while it may seem trivial, career history can help determine a correct diagnosis. Additionally, 25% of our patients had diabetes; however, Alenazi et al. 19 reported a completely different result. This divergence might be caused by insufficient numbers of patients with BPA.
Interestingly, BPA has a slow progression rather than an acute onset. Additionally, BPA may be found with concurrent brucellosis in multiple organ systems, resulting in complex and diverse clinical manifestations. Our study found that the most common clinical manifestations in BPA were fever and dysuria, consistent with other studies.20–22 The fever might be caused by inflammatory mediators in the blood, and the enlarged prostate might cause dysuria. Among our BPA cases, 37.5% had concurrent seminal vesicle infections, and one patient had epididymitis. Other studies reported a 10% incidence of epididymitis in brucellosis.15,21 We attached great importance to these studies’ findings because the studies revealed that BPA significantly reduced the quality of life among middle-aged men.
CRP concentration in all of our cases and ESR in all but one of the patients were increased to varying degrees, and these results were highly consistent with findings reported by She et al. and Cift and Yucel.3,23 ESR and CRP are two common indicators that reflect infection in the body. The results of the standard tube agglutination test in our study were positive in all patients (>1:160). Other laboratory results were also increased, namely monocyte count (50.0%), neutrophil count (25.0%), red blood cell count (25.0%), and white count (25.0%), similar to results reported by Trotta et al. 24
MRI provides the highest tissue contrast resolution among imaging tests, and we found that it clearly revealed single or multiple prostatic abscesses. In the current study, prostatic enlargement occurred in 87.5% of the patients, and the BPA lesions occurred mainly in the peripheral zone (87.5%) and central zone (100%). All patients showed homogenous signals on T1WI and hyperintense signals on STIR. The reason for this difference may be that the prostate is a glandular tissue with a relatively high water content; therefore, TIWI results in a homogenous signal. All lesions appeared as a small nodule or multiple nodules. The results of a study of hepatosplenic brucella abscess were similar. 13 In addition, all of our patients presented with hyperintense signals on STIR. DWI is a very good technique for examining abscesses, and helps differentiate abscesses from tumors. In this study, all patients had slight hyperintense to hyperintense signals on T2WI and DWI, and all patients showed mild ring enhancement on contrast-enhanced MRI. Three patients had pelvic effusion. Patients were also complicated with other organ infections, which is consistent with the characteristics of brucellosis, which tends to invade multiple organs.3,10
All of our patients received daily rifampicin, doxycycline, and levofloxacin, with an average of 12.6 weeks of combined treatment. The clinical symptoms of all patients resolved, and all lesions had disappeared by the end of treatment on follow-up ultrasonography.
There are several limitations to our study. First, this study involved a small number of patients; second, not all patients underwent biopsy; and finally, all patients were selected from the same hospital, which may have caused selection bias. Consequently, further studies with more patients from different hospitals are needed to confirm our findings.
Conclusion
Even in epidemic areas, the incidence of BPA is relatively rare. Our findings can increase the understanding of BPA and reduce misdiagnosis and mistreatment. Importantly, when encountering a prostatic abscess, the possibility of BPA must be considered, especially for herdsmen in endemic areas.
Footnotes
Acknowledgments
The authors gratefully acknowledge the financial support provided by the Xinjiang Uygur Autonomous Region Natural Science Foundation of China.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Xinjiang Uygur Autonomous Region Natural Science Foundation of China (Grant no. 2017D01C300).
The funding agency was not involved in the research design, data collection, data analysis, or the study conclusions. All of the authors had access to all data.
Author contributions
HG and WL conceived the study and wrote the main manuscript. HG prepared Figures 1 to ![]() . YH and SL collected the data. SL and ZG performed the literature search. All authors reviewed the manuscript, and all authors approved the final version for submission.
. YH and SL collected the data. SL and ZG performed the literature search. All authors reviewed the manuscript, and all authors approved the final version for submission.