
Abstract
Objective
To retrospectively investigate the epidemiological features, clinical manifestations and laboratory characteristics of bacteremic brucellosis.
Methods
Brucellosis patients admitted to our clinic from January 2015 to December 2017 were included in the study. Patient electronic medical records were reviewed for epidemiological features, clinical manifestations, and laboratory findings.
Results
A total of 132 brucellosis patients were analyzed (64 cases with bacteremic brucellosis and 68 cases with nonbacteremic brucellosis). The median duration from exposure to onset of symptoms was 6.9 weeks (range: 1 day to 32 weeks) and 21.9 weeks (range: 1–76 weeks) in patients with bacteremic and nonbacteremic brucellosis, respectively. More bacteremic than nonbacteremic patients presented with fever and chills. Arthritis was observed in 34 (25.8%) patients, and was more commonly observed in nonbacteremic patients. Using C-reactive protein (CRP) and procalcitonin (PCT) as serological markers, the areas under the receiving operating characteristic curves were 0.64 [95% confidence interval (CI): 0.54–0.73] and 0.61 (95% CI: 0.51–0.70), respectively, for distinguishing bacteremic from non-bacteremic brucellosis.
Conclusion
Fever and chills were frequently observed in bacteremic brucellosis patients, whereas arthritis was more common in nonbacteremic brucellosis patients. Serum CRP and PCT can be used as potential serological markers for diagnosing bacteremic brucellosis.
Introduction
Brucellosis is a prevalent zoonotic disease worldwide and continuous to be a major public health problem.1,2 Brucellosis is caused by facultative intracellular pathogens of the genus Brucella. Domestic and wild animals are considered natural reservoirs. 3 The disease is mainly transmitted to humans by direct contact with infected animals or by consumption of unpasteurized milk and meat products derived from infected animals. 4 Human brucellosis is a systemic infection that can affect various organ systems. Brucellosis typically causes abortion and sterility in animals and can have a variety of clinical presentations in humans including fever, sepsis, and multiple organ involvement.5,6 Brucella species have unique epidemiological, phylogenetic and pathogenetic characteristics. One unique characteristic is the significance of bacteremia in the course of the disease. 7
Although bacteremic brucellosis is not uncommon, reports of bacteremic brucellosis are scarce. The clinical features and complications of this disease are unclear. The present study aimed to retrospectively investigate the epidemiological features, clinical manifestations and laboratory characteristics of bacteremic brucellosis.
Materials and methods
Brucellosis patients admitted to the Department of Infectious Diseases and Clinical Microbiology of Tianjin Second People’s Hospital between January 2015 and December 2017 were included in the study. A retrospective analysis was undertaken. Patient electronic medical records were reviewed for epidemiological features, clinical manifestations, and laboratory findings. The study was approved by the Medical Ethics Committee of our hospital. Written consent was obtained from each participant.
Brucellosis was diagnosed on the basis of one of the following criteria: (1) isolation of Brucella species in blood; and (2) compatible clinical features, such as arthralgia, fever, sweating, chills, headache and malaise, supported by detection of specific antibodies at significant titers and/or demonstration of a fourfold or higher increase in antibody titer in serum specimens taken at 2- or 3-week intervals. Significant antibody titers were determined to be 1/160 or greater in agglutination tests. 8 Patients with positive culture results for Brucella species were classified as having bacteremic brucellosis and those with negative culture results for Brucella species were classified as having nonbacteremic brucellosis. Therefore, nonbacteremic patients were diagnosed based on clinical features suggesting brucellosis as well as antibody titers and agglutination tests.
Blood culture samples were incubated in the Bact/Alert 3D system (BioMeriéux, Marcy-l'Étoile, France) for up to 7 days. Typing of the bacteria was based on CO2 requirements, urease activity and growth on basic fuchsin and thionin dyes. Brucella species were determined using standard biochemical methods. Blood samples were prepared according to the guidelines of different tests. Routine blood counts and measurements of CRP, PCT and blood chemistry were conducted for all patients. Blood counts were determined using a Sysmex XT-4000i instrument (Sysmex, Kobe, Japan). Serum CRP levels were quantitated using an immunoturbidimetric assay with a Lifotronic instrument (Shenzhen Lifotronic Technology Co., Shenzhen, China). Serum PCT measurements were performed using an electrochemiluminescence immunoassay and a Cobas immunoassay analyzer (Roche, Basel Switzerland). Blood chemistry was assessed using a Hitachi 7180 automatic analyzer (Hitachi, Tokyo, Japan). Clinical and laboratory data were collected from comprehensive electronic medical records.
Statistical analysis
Statistical analysis was performed using SPSS 19.0 software (SPSS Inc., Chicago, IL, USA). For normally distributed variables, data were presented as means and standard deviations. Differences between continuous variables were assessed using the Student’s t-test for parametric data. Differences between categorical variables were assessed using the chi-square test. Values of p < 0.05 were considered statistically significant.
Results
Patient demographics
A total of 132 patients with brucellosis were enrolled in the study including 64 cases with bacteremic brucellosis (47 men, 73.4% and 17 women, 26.6%) and 68 cases with nonbacteremic brucellosis (58 men, 85.3% and 10 women, 14.7%). The mean age of bacteremic cases was 47.1 ± 14.5 years (range: 2–69 years) and the mean age of nonbacteremic cases was 47.5 ± 14.4 years (range: 3–70 years). The median duration from exposure to the onset of symptoms was 6.9 weeks (range: 1 day to 32 weeks) and 21.9 weeks (range: 1–76 weeks) in bacteremic and nonbacteremic cases, respectively (p = 0.017). The mode of transmission was considered to be: (1) consumption of unpasteurized milk and meat products from infected animals (17 patients, 12.9%) and (2) direct contact with animals or animal products (109 patients, 82.6%). No source of infection was identified for six patients (4.5%). The demographic and epidemiological characteristics of patients are shown in Table 1.
Demographic and epidemiological characteristics of patients.

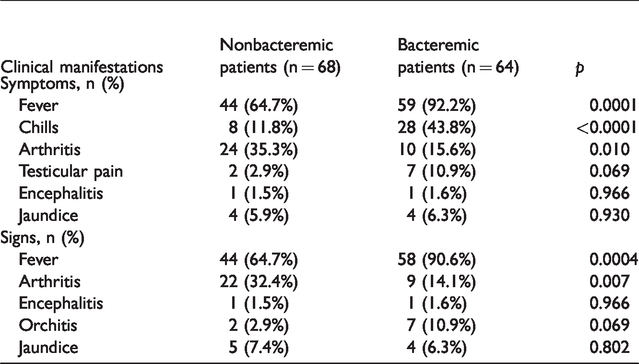
Clinical manifestations of brucellosis
The most frequent clinical manifestations were fever (78.0%) and chills (27.3%). More bacteremic than nonbacteremic patients presented with fever and chills as symptoms (fever, p = 0.001; chills, p = 0.001). Arthritis was observed in 25.8% of brucellosis patients and was significantly more common in nonbacteremic patients (35.3%) (p = 0.010). Orchitis was observed in 6.8% of patients and occurred in similar proportions of bacteremic and non-bacteremic cases (Table 2).
Comparison of clinical manifestations of brucellosis patients.
Laboratory characteristics of brucellosis patients
Significant elevations of serum CRP levels (p = 0.001) and thrombocytopenia (p = 0.023) were detected in bacteremic cases. Of the 132 patients, 11 (8.3%) had anemia, eight (6.1%) had thrombocytopenia and 92 (69.7%) had normal blood cell counts. Elevated liver enzyme levels were detected in about 20% of patients with brucellosis. The albumin levels of bacteremic patients were slightly but significantly lower than those of nonbacteremic patients (37.43 ± 3.68 g/L vs. 39.97 ± 3.99 g/L) (p = 0.001). The most frequent laboratory findings were high serum CRP levels (63.6%) in bacteremic patients. No elevation in serum PCT levels were observed in either bacteremic or nonbacteremic patients (Table 3).
Comparison of the laboratory characteristics of patients.
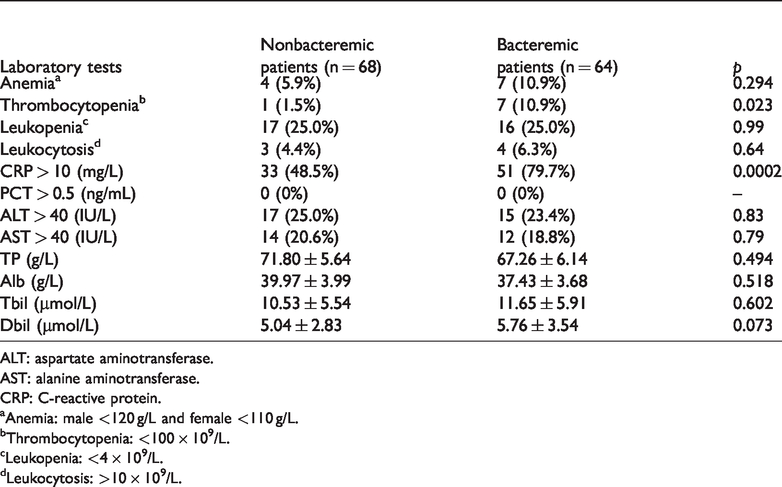
ALT: aspartate aminotransferase.
AST: alanine aminotransferase.
CRP: C-reactive protein.
aAnemia: male <120 g/L and female <110 g/L.
bThrombocytopenia: <100 × 109/L.
cLeukopenia: <4 × 109/L.
dLeukocytosis: >10 × 109/L.
Diagnostic performance of serum CRP and PCT
Using serum CRP and PCT levels as serological markers, the areas under the receiver operating characteristic curves were 0.64 [95% confidence interval (CI): 0.54–0.73] and 0.61 (95% CI: 0.51–0.70), respectively (Figure 1).

Receiver operating characteristic curves of serum CRP and PCT levels as serological biomarker for diagnosis of bacteremic brucellosis (a: CRP; b: PCT).
Discussion
Brucellosis is a re-emerging bacterial zoonosis that remains endemic in China. Infections can cause serious complications, and early diagnosis is important for optimal prognosis. 9 The gold standard for the diagnosis for brucellosis is identification of Brucella species from blood or bone marrow cultures.10,11 The rate of positive blood cultures in brucellosis ranges from 15% to 90%.3,12 Clinically, brucellosis may occur as an acute (less than 2 months), subacute (2 months to 12 months) or chronic (more than 12 months) infection. Blood culture results vary depending on disease progression. Consistent with previous studies, we found that acute brucellosis was usually associated with a high rate of Brucella bacteremia.11,12
Brucellosis is a systemic infection and can lead to various clinical symptoms. Therefore, signs and symptoms are usually not specific. Fever was reported as the most common presenting sign in bacteremic patients.5,11,13 In our study, fever and chills were observed significantly more often in bacteremic patients than in nonbacteremic patients. Fewer bacteremic than nonbacteremic patients presented with arthritis. A Turkish study of mostly adult patients demonstrated similar results. 14
Early assessment of the risk of brucellosis relies on information derived from clinical examinations and laboratory findings. 15 Of the 132 patients studied here, 8.3% had anemia, 6.1% had thrombocytopenia and 70.0% had normal blood cell counts. A slight elevation of liver enzyme levels could be detected in approximately 20% of all patients with brucellosis. Elevated liver enzyme levels are usually subclinical and jaundice is rare. 16 Elevated alanine aminotransferase levels returned to normal in all patients when treatment was finished. We observed lower albumin and platelet count in bacteremic patients compared with nonbacteremic patients, which might occur because liver and bone marrow dysfunction is more severe in bacteremic patients.
Inflammatory markers measured in the clinical assessment of brucellosis patients often provide useful information. Serum CRP and PCT are classic serological markers of inflammation and are used to monitor the progress of infection. CRP is a sensitive but nonspecific biomarker of systemic inflammation, and is synthesized in the acute phase of inflammatory responses.17,18 Elevated CRP levels are associated with brucellosis and might be useful to diagnose acute brucellosis. 19 Compared with nonbacteremic cases, elevated CRP levels were detected significantly more often in bacteremic cases. As a nonspecific inflammatory marker, CRP alone is a suboptimal predictive factor for Brucella infection, although more than 60% of patients with brucellosis show CRP elevation.
PCT, a precursor of the hormone calcitonin, is synthesized by thyroid C cells and generally has low levels in healthy individuals. PCT production in various tissues occurs in inflammatory processes such as sepsis, severe systemic bacterial infections, malaria and some fungal infections.20–22 PCT levels >0.5 ng/mL are usually considered as diagnostically relevant for most bacterial infections. 23 Our findings revealed that all brucellosis patients had normal levels of PCT irrespective of their blood culture results. This suggested that PCT levels in brucellosis may be specific but not sensitive for Brucella bacteremia. A previous receiver operating characteristic curve analysis of PCT levels in Brucella bacteremia suggested that PCT was not sufficiently sensitive in diagnosing Brucella bacteremia, but could be useful for excluding Brucella bacteremia. 24
In conclusion, patients with Brucella bacteremia presented early in their course of illness. Their clinical features and laboratory characteristics, however, did not differ from nonbacteremic brucellosis patients. Fever and chills were frequently observed in bacteremic brucellosis patients, whereas arthritis was more often observed in nonbacteremic brucellosis patients. Liver and bone marrow dysfunction was more severe in bacteremic patients than nonbacteremic patients.