
Abstract
Objective
Necrotizing soft tissue infection (NSTI) is a rare but life-threatening bacterial infection. This study was performed to analyze the clinical characteristics of patients with NSTI admitted to the intensive care unit of a trauma and burn center in Beijing and to summarize the treatment experience.
Methods
This retrospective study involved patients with NSTI admitted to the intensive care unit from January 2010 to January 2020. The clinical manifestations, pathogens, laboratory test results, and prognosis were compared between survivors and nonsurvivors.
Results
Thirty-two patients were enrolled (28 men, 4 women), including 25 (78.1%) survivors and 7 (21.9%) nonsurvivors. The patients’ median age was 41.5 years (range, 30.0–52.5 years). Mortality was significantly higher in patients with a blood urea nitrogen concentration of ≥11.5 mg/dL, creatinine concentration of <3.4 mg/dL, prothrombin time of ≥15.9 s, and international normalized ratio of ≥1.3. Streptococcus pyogenes and Clostridium perfringens infections were associated with higher mortality.
Conclusions
More attention should be given to elderly patients and those with hyponatremia, coagulation disorder, and higher blood urea nitrogen or creatinine concentrations. The finding of large gram-positive rods or large numbers of gram-positive cocci in wound secretion smears is a helpful early warning sign of highly lethal NSTI.
Keywords
Introduction
Necrotizing soft tissue infection (NSTI) is a rare but life-threatening bacterial infection characterized by rapid and extensive necrosis from the epidermis to the deep musculature. 1 It is often associated with sepsis and multiple organ failure, leading to a poor prognosis. NSTI is divided into types I and II based on the presence of polymicrobial or monomicrobial infection, respectively. The incidence of NSTI is 0.3 to 5.0 cases per 100,000 people worldwide. 1 , 2
The early clinical manifestations of NSTI are nonspecific. It can occur in any part of the body even without an obvious wound. However, distinguishing NSTI from common cellulitis is difficult in the early stage. The rates of misdiagnosis and missed diagnosis are as high as 85% to 100%. 1 Furthermore, NSTI develops rapidly and can lead to septic shock within 24 to 72 hours. Once this stage is reached, mortality is high even with aggressive treatment. 3
At present, very few reports about NSTI exist in China. Therefore, the present study was performed to analyze the clinical characteristics and mortality factors of patients with NSTI by reviewing the records of patients admitted to the intensive care unit (ICU) of Beijing Jishuitan Hospital in the past 10 years. The aim of this study was to provide a reference for NSTI management.
Materials and methods
The study protocol was approved by the Institutional Review Board of Beijing Jishuitan Hospital, Peking University on 1 April 2020 (No. 202003-04). Written consent was obtained from each patient prior to treatment. All patient details were de-identified to protect patient privacy. The requirement for informed consent for publication was waived because of the retrospective nature of the study. The reporting of this study conforms to the STROBE statement. 4
Patients
This retrospective study involved consecutive patients who were diagnosed with NSTI and admitted to the ICU of Beijing Jishuitan Hospital from January 2010 to January 2020. NSTI was diagnosed based on clinical findings, imaging tests, and microbiological examinations and was confirmed by surgical findings (gray necrotic tissue, lack of bleeding, thrombosed vessels, dishwater-gray exudate, noncontracting muscle, and positive finger test result). 1 , 5 Histologic examination was not routinely performed. Patients with severe infection of other organs, patients with lethal organ damage, children, and patients with incomplete medical records were excluded. The patient population was divided into a survivor and nonsurvivor group.
Data collection
The demographic data, cause of injury, location of the infection, local symptoms, clinical presentation, comorbidities, time from admission to the first operation, and initial laboratory test results were collected from the patients’ charts. Microbiological data (wound secretion smear results and blood, secretion, and tissue culture results) and clinical outcomes (number of operations, length of ICU stay, total hospitalization duration, and mortality rate) were documented. For all patients, the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score; 6 Site other than the lower limb, Immunosuppression, Age, Renal impairment, and Inflammatory markers (SIARI) score; 7 NSTI Assessment Score (NAS); 8 Acute Physiology and Chronic Health Evaluation II (APACHE II) score; and Sepsis-related Organ Failure Assessment (SOFA) score were calculated from the initial laboratory results.
Statistical analysis
All data were analyzed using SPSS Statistics for Windows, Version 17.0 (SPSS Inc., Chicago, IL, USA). Quantitative data with a normal distribution are presented as mean with standard deviation, and those with a non-normal distribution are presented as median with interquartile range. Qualitative data are presented as frequency and percentage. Differences between the two groups were compared using an independent-groups t-test when the quantitative data were normally distributed with homogeneity of variance; otherwise, the Mann–Whitney U test was used. Qualitative data were compared using the χ2 test, and Fisher’s exact test was used when data were limited. All laboratory findings (quantitative data) were reanalyzed with conversion to qualitative data by calculating the cutoff value through the receiver operating characteristic curve. A p value of <0.05 was considered statistically significant.
Results
The database contained information regarding 34 patients diagnosed with NSTI. However, one patient with an abdominal infection (intestinal rupture) and one child (9 years old) were excluded. Consequently, 32 patients with NSTI were enrolled in this study. The male:female ratio was 7:1 (28 men, 4 women), and their median age was 41.5 years (range, 30.0–52.5 years). The patients comprised 25 survivors and 7 nonsurvivors (Table 1). The overall mortality rate was 21.9%.
Comparison of demographics and clinical characteristics between the survivor and nonsurvivor groups.

Data are presented as median (interquartile range) or number of patients. p < 0.05 was considered statistically significant.
BMI, body mass index; NSTI, necrotizing soft tissue infection.
NSTI was most commonly seen during spring and summer (87.5%). The etiologies of injury were car accidents (n = 27), machine-related injuries (n = 2), an animal bite (n = 1), minor muscle contusion (n = 1), and absence of antecedent trauma (n = 1). Furthermore, 6 (18.8%) of the 32 patients had comorbidities, including diabetes (n = 4), hypertension (n = 1), and hyperlipidemia (n = 1). Lower extremity infection was the most common presentation (78.1%). Other infection sites included the upper extremity in three (9.4%) patients, perineum and genital area in three (9.4%), and shoulder in one (3.1%). The most common manifestations were swelling (93.8%), severe pain (90.6%), and fever (87.5%) (Figure 1).

Frequency of presenting symptoms.
The median APACHE II and SOFA scores were 14 (range, 11–17) and 8 (range, 5.3–10), respectively. The false-negative rates of the LRINEC score, SIARI score, and NAS were 6.3%, 34.4%, and 31.2%, respectively.
All patients underwent wound secretion and blood cultures during the early stage of admission with a positive rate of 93.8%. No microbes were identified in two patients. Escherichia coli was the most common pathogenic bacteria (9/30, 30.0%). Clostridium perfringens (2/3, 66.7%) and Streptococcus pyogenes (3/5, 60.0%) were associated with a high mortality rate (Figure 2).

Composition of pathogenic bacteria.
In terms of laboratory tests, the blood urea nitrogen (BUN) concentration, prothrombin time, and international normalized ratio were significantly higher in the nonsurvivor than survivor group (p = 0.001, p = 0.020, and p = 0.006, respectively) (Table 2); however, the sodium concentration was significantly lower in the nonsurvivor group (p < 0.001). Mortality was significantly higher in patients with a BUN concentration of ≥11.5 mg/dL (p < 0.001), creatinine concentration of ≥3.4 mg/dL (p < 0.001), prothrombin time of ≥15.9 s (p = 0.015), and international normalized ratio of ≥1.3 (p = 0.009).
Initial laboratory and clinical findings on admission.
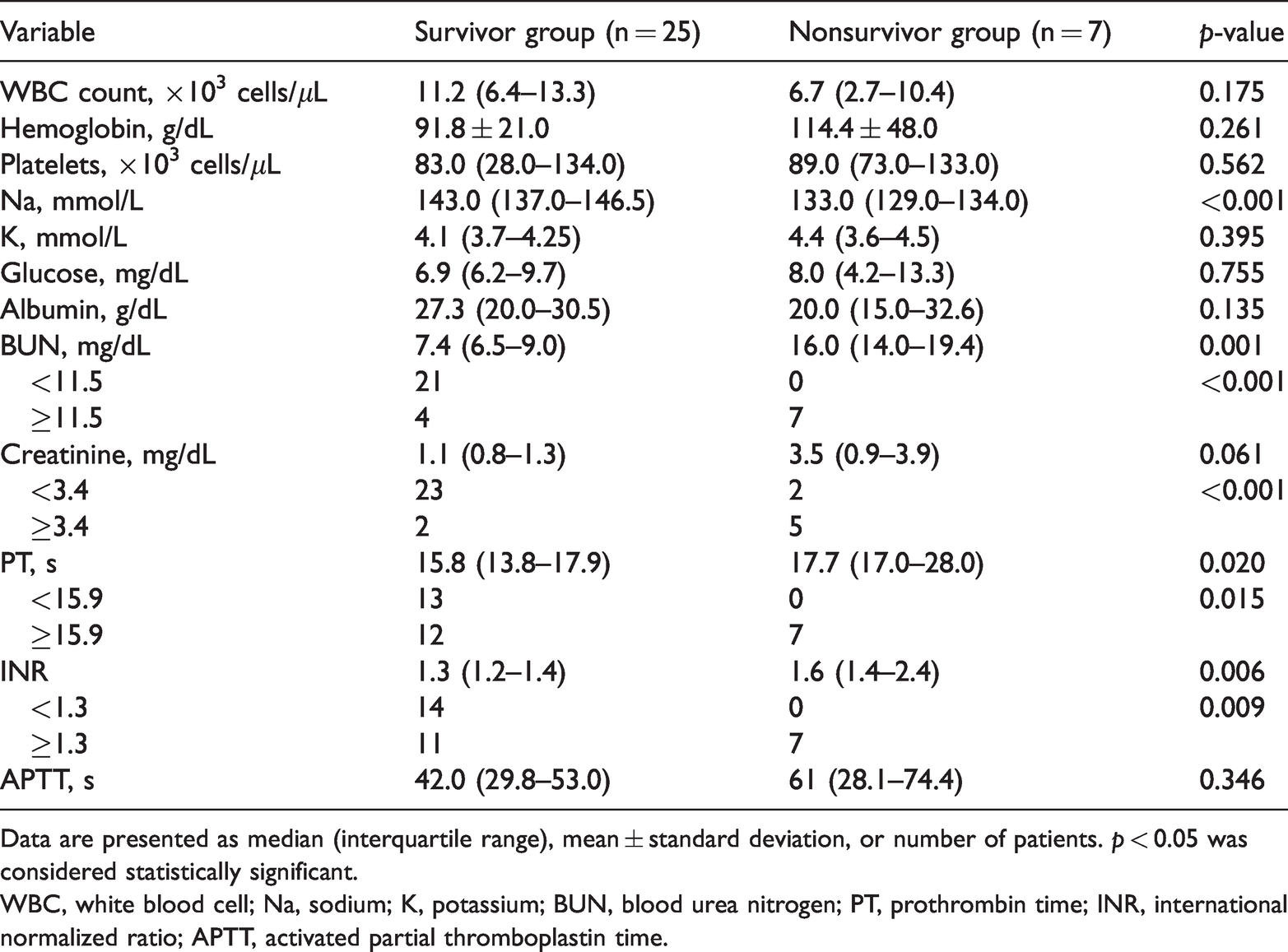
Data are presented as median (interquartile range), mean ± standard deviation, or number of patients. p < 0.05 was considered statistically significant.
WBC, white blood cell; Na, sodium; K, potassium; BUN, blood urea nitrogen; PT, prothrombin time; INR, international normalized ratio; APTT, activated partial thromboplastin time.
All patients underwent at least one surgery. The median time from admission to the first operation was 9.5 hours (range, 8.0–12.8 hours). However, the median time from admission to the first operation was significantly shorter in the survivor than nonsurvivor group (p = 0.002). The total duration of hospitalization was 36.0 days (range, 27.0–44.0 days) with an ICU stay of 14.5 days (range, 7.0–20.0 days). No statistically significant difference was found in the total duration of hospitalization or ICU stay between the survivor and nonsurvivor groups.
The details of a special case of NSTI in a patient without obvious trauma are shown in Figure 3.
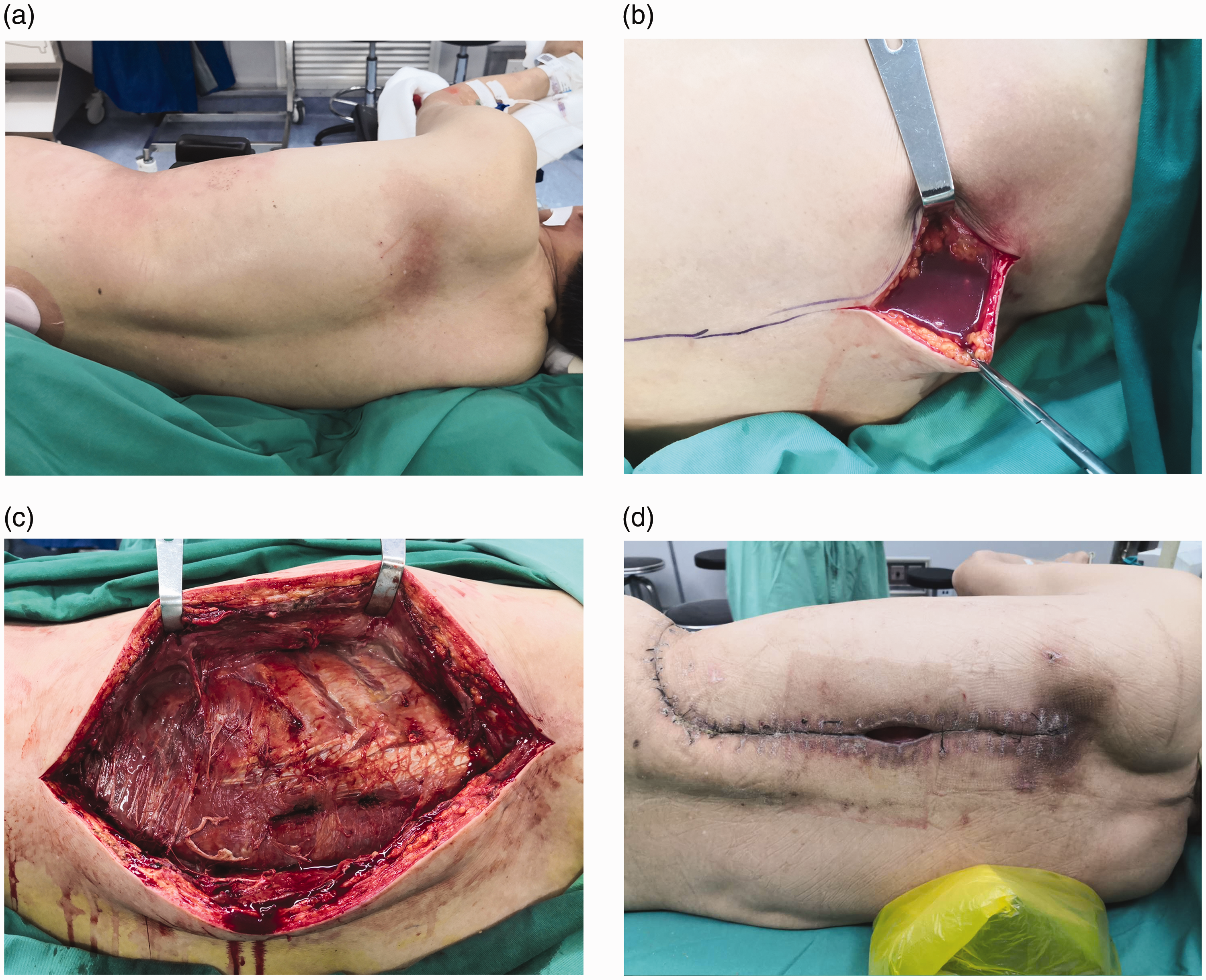
Necrotizing soft tissue infection in a patient without obvious trauma. A 63-year-old man developed subcutaneous pain in the left chest after a fall 1 month previously but had no open wounds. No abnormalities were noted on repeated chest and abdomen computed tomography examinations. The pain gradually expanded to the entire left chest and back. He was admitted to the hospital with a high fever and shock. After admission, his white blood cell count and C-reactive protein concentration were 24.7 × 109/L and >160 mg/L, respectively. Imipenem–cilastatin sodium and linezolid were given for anti-infection treatment. (a) Postoperative posture. (b) First operation; a large amount of dishwater-gray exudate was encountered after cutting the latissimus dorsi. (c) A long incision extending along the longitudinal axis of the body revealed necrotic fascia and muscles. (d) The wound healed after five operations.
Discussion
NSTI has been described as various entities (e.g., necrotizing fasciitis, necrotizing myositis, gas gangrene, and streptococcal gangrene). 1 However, given the extensive involvement of the epidermis, dermis, subcutaneous tissue, fascia, and muscle, as well as their similar clinical features and treatment strategies (antibiotics, early extensive surgery, and organ supportive care), recent literature suggests that these severe soft tissue infections should be classified as NSTI. 1 , 2 NSTI can be classified into types I (polymicrobial) and II (monomicrobial), and the incidence of these two types is typically very similar. 9 , 10 The most common pathogens involved in type I infection are Escherichia coli and Enterococcus species, whereas Streptococcus pyogenes and methicillin-resistant Staphylococcus aureus are the most common pathogens involved in type II infection. 1 In the present case series, the incidence ratio of types I and II infection was 1.0:1.3 (13 vs. 17 patients, respectively). Moreover, the mortality of type II NSTI was significantly higher than that of type I (35.2% vs. 7.7%, p < 0.05).
Despite advances in the understanding of NSTI, the mortality rate of NSTI is still high at 18% to 34%. 11 , 12 The overall mortality in the present study was 21.9%. In previous studies, factors associated with high mortality included older age, delayed surgery, low body mass index, and abnormal laboratory test parameters (white blood cells, hemoglobin, creatinine, sodium, BUN, and platelets). 9 , 13 , 14 In the present study, nonsurvival was associated with older age, a higher BUN or creatinine concentration, coagulation disorder, lower sodium concentration, and longer duration from admission to the first operation compared with patients in the survivor group.
The mortality rate among patients infected with Streptococcus pyogenes or C. perfringens was significantly higher than that among patients infected by other pathogens. In previous studies, the average mortality rate associated with infection by Streptococcus pyogenes infection was 29% and reached 45% when combined with septic shock. 3 , 15 Without adequate surgical debridement, mortality due to C. perfringens infection may reach 100%. 16 In the present study, mortality due to Streptococcus pyogenes and C. perfringens infection was 60.0% and 66.7%, respectively (Figure 2). Moreover, Streptococcus pyogenes infection was exclusively seen in type II NSTI, whereas C. perfringens was observed in both types. The high mortality of these two pathogens is mainly due to their potent bacterial exotoxins and the host response. 1
Early detection of Streptococcus pyogenes and C. perfringens is of great importance for clinical decision-making and thus lowering mortality. Wound smears can provide valuable information early in the disease course. Furthermore, C. perfringens is the main pathogen causing gas gangrene (80%). Other pathogens include C. novyi, C. septicum, and C. sporogenes. 1 , 17 In this study, all cases of gas gangrene were caused by C. perfringens. Clostridium perfringens presents as large gram-positive rods without spores on examination of wound smears. 18 The early wound secretion smears from the three patients with gas gangrene infection in the present study showed large gram-positive rods, indicating that the secretion smear has good sensitivity for C. perfringens screening. However, isolation of C. perfringens from the wound is not sufficient to diagnose gas gangrene because this microorganism may colonize the wound without causing disease. 18 In addition, wound smears for the screening of C. perfringens are accompanied by a certain false-positive rate. Microbes such as Bacillus subtilis also show similar large gram-positive bacilli (Figure 4), but they do not progress to gas gangrene. Thus, Streptococcus pyogenes infection is histologically characterized by a paucity of infiltrating phagocytes and large numbers of gram-positive cocci at the infected site. 1 Therefore, the possibility of the presence of highly lethal NSTI is indicated when large gram-positive rods or large numbers of gram-positive cocci are observed in the wound smear.

Wound secretion smear of Clostridium perfringens and Bacillus subtilis (gram staining). (a) Large-form gram-positive bacilli. The culture results revealed C. perfringens. (b) Gram-positive bacilli similar to C. perfringens. The culture results revealed B. subtilis.
Surgical exploration is an indispensable method for the diagnosis of NSTI. It is also essential for determining the extent of infection and controlling the source of infection. 19 , 20 Typical findings include gray necrotic tissue, lack of bleeding, thrombosed vessels, dishwater-gray exudate, noncontracting muscle, and a positive finger test result. 1 , 4 Minimizing the time from admission to the first operation is critical for reducing mortality. 21 In one study, the survival rate of patients who underwent surgery within 24 hours after admission was significantly higher than that of patients who underwent surgery after 24 hours. 9 In the present study, the median time from admission to the first operation was 9.5 hours (range, 8.0–12.8 hours), which was significantly shorter than that in previous studies (19–35 hours). 9 , 22 This discrepancy has two likely explanations. First, because they work exclusively in a local trauma and burn rescue center, the surgeons in our trauma and burn department are more experienced in identifying NSTI, which helps avoid delayed diagnosis and thus misdiagnosis. Second, because our institution is a tertiary referral center, the diagnosis of NSTI may be made elsewhere before admission to Beijing Jishuitan Hospital.
According to the guidelines published by the Infectious Diseases Society of America, 20 vancomycin or linezolid combined with carbapenem or piperacillin–tazobactam is recommended for treatment of NSTI. Furthermore, piperacillin–tazobactam is preferred as the initial antibiotic treatment if the pathogen is suspected to be Streptococcus pyogenes. In addition to surgical debridement and antibiotic treatment, the roles of organ support, standardized antishock therapy, and multidisciplinary collaboration have also been recognized. Approximately 50% of patients with NSTI develop septic shock during their disease course. 9 Thus, implementation of the sepsis bundle within 1 hour is recommended to improve the prognosis of patients with septic shock. 23 Moreover, multidisciplinary collaborative management is an effective modality to reduce the mortality rate of NSTI. 2 , 9 In Beijing Jishuitan Hospital, the intensivists participate in the treatment of patients with NSTI as soon as a septic shock is suspected. After the operation, all patients are transferred to the ICU to further manage shock and provide organ and nutritional support. The clinical pharmacists assist in the assessment of antibiotic treatment. The surgeons oversee daily wound care. Finally, patients are transferred to the Department of Burns and Plastic Surgery for wound repair if their clinical condition is stable.
Wong et al. 6 proposed the LRINEC score, which is the most widely used predictive system for NSTI diagnosis. The LRINEC scoring system uses the total white blood cell count and the hemoglobin, sodium, glucose, creatinine, and C-reactive protein concentrations to differentiate NSTI from other mild infections. However, the positive predictive value of the LRINEC score ranges from 57% to 92%. 6 , 9 , 19 In addition, some new predictive scoring systems have been proposed (e.g., SIARI score and NAS). 7 , 8 The validated false-negative value of the LRINEC score (6.3%) in the present study was significantly lower than the SIARI score (34.4%) and NAS (31.2%).
At present, very few reports about NSTI exist in China. In this study, we analyzed the characteristics and prognosis of 32 patients with NSTI. We highlighted the lethality of Streptococcus pyogenes and C. perfringens infection and discussed the role of wound smear in early detection of these highly lethal pathogens, which may be of practical significance for clinical practice. Furthermore, we introduced our experience in treating NSTI. We emphasized the importance of multidisciplinary collaborative management as an effective modality to reduce NSTI-related mortality.
This study has some limitations. First, this was a retrospective single-center study. The small sample size was too underpowered to show statistical significance. Second, the evaluation of predictive tools was limited to the false-negative rate because patients with conditions mimicking NSTI (such as mild soft tissue infection) were excluded from this study. Thus, further studies are necessary. Finally, information on the time from injury to admission was missing for some patients, so the time from admission to the first operation was used instead. The results are still comparable because most previous studies also adopted this parameter.1,8,21
Conclusions
Clinicians should fully understand the clinical characteristics and mortality-related factors of NSTI. Elderly patients and patients with hyponatremia, coagulation disorder, or higher BUN or creatinine concentrations may be at higher risk of death; thus, more attention should be given to these patients. The finding of large gram-positive rods or large numbers of gram-positive cocci on wound secretion smears may be helpful as an early warning of highly lethal NSTI. The avoidance of delayed debridement, rational use of antibiotics, and multidisciplinary cooperation are essential for improvement of the clinical outcome of NSTI.