
Abstract
Objective
In patients undergoing plastic surgery, to identify specific risk factors for anaemia and use of blood products, and assess their impact on patient outcome.
Method
For this retrospective study, data were analysed from patients who attended the Plastic Surgery Department at our hospital over a three-year period (2018 to 2020). Adult patients who presented with traumatic injuries, oncologic patients who underwent reconstructive procedures, and patients with soft tissue infections (STIs) who required plastic surgery for tissue coverage were included. Demographic and injury data, hospital admission characteristics, surgical procedures, laboratory test results, transfusion events, and in-hospital complications were extracted from patient records.
Results
Of the 350 patients included in the study, 228 (65%) presented with trauma, 76 (22%) underwent reconstructive surgery for cancers and 46 (13%) had STIs. In total, 175 (50%) patients developed anaemia, and 37 (11%) received blood transfusions; these were 20 (54%), 5 (14%), and 12 (32%) patients in the trauma, cancer and STI groups, respectively. Associated comorbidities and upper and lower limb surgery were the most significant risk factors for anaemia, while the number of surgeries and NSTIs were identified as risk factors for blood transfusions. Direct wound closure was consistently a protective factor for both anaemia and blood transfusions. Blood transfusions were independently associated with a high risk of sepsis, wound complications, and prolonged hospital stay.
Conclusion
While transfusions are necessary and even lifesaving in surgical patients, blood is a finite resource and its use may negatively impact patient outcome. Therefore, ongoing research must focus on providing safe and restrictive clinical practices while developing sustainable and accessible alternatives.
Keywords
Introduction
Patients who undergo plastic surgery vary in demographics, pathology, and surgical procedure requirements. Reconstructive surgery aims to restore function and aesthetics and may include, breast reconstruction after mastectomy, congenital craniofacial malformations repair, scar revision, skin grafting, and hand surgery for injuries or deformities. Burn reconstructive surgery repairs damaged skin, restores function, and improves appearance. Trauma reconstruction surgery can help restore features and function as well as provide soft tissue coverage and functional reconstruction, as is the case in limb trauma.
The cause of anaemia in plastic surgery patients is often multifactorial. Leading causes include, nutritional deficiencies (e.g., iron, vitamin B12, or folate), chronic diseases, and blood loss. 1 Treating the underlying cause may involve dietary changes, oral supplements, or medications. 2 However, severe anaemia may require blood transfusions. Blood products are used to replenish the patient's blood volume and improve oxygen delivery to tissues to promote healing. 3 The decision to transfuse will be based on various factors such as, clinician experience, current guidelines, institutional protocols, patient symptoms, haemoglobin level, and patient related comorbidities. Transfusion triggers are often individualised based on a comprehensive assessment of the patient’s status, hemodynamic stability, symptoms, and laboratory values.4–6 While blood transfusions are generally considered safe, there are potential complications that may occur during or after transfusion and vary in severity. For example, transfusion reactions can range from mild (e.g., fever, chills, or rash) to severe (e.g., anaphylaxis). In addition, transfusion-transmitted infections, fluid overload, transfusion-related acute lung injury (TRALI), iron overload and immunological complications although rare have also been recorded. 7 In an attempt to reduce unnecessary transfusions and associated risks, there has been a shift towards more restrictive transfusion practices. Indeed, this strategy is supported by clinical guidelines and evidence-based research that have found more liberal transfusion strategies do not inherently improve patient outcomes and may be associated with increased risks.8–10
We collected retrospective data from patients that had undergone one of three categories of plastic surgery (i.e., trauma surgery, cancer reconstruction surgery and surgery for severe soft tissue infections [STIs]). The purpose of our study was to identify risk factors for anaemia and blood transfusions and to ascertain their impact on patient outcome.
Methods
This was a single centre, retrospective study involving patients admitted to the Plastic Surgery Department of the Emergency County Hospital in Cluj-Napoca over a 3-year period between 2018 and 2020. Patient characteristics were obtained using Atlasmed, the hospital’s electronic medical records system and transfusion data were obtained from the hospital’s blood bank registry. Patients were consecutively included if they were aged 18 years and over, and, presented with various surgical requirements that could be catalogued into the three main categories (i.e., trauma surgery, cancer reconstruction surgery and surgery for severe STIs). For the trauma group, patients were further classified by location, mechanism, and severity of injury. For those presenting with malignant conditions requiring reconstructive plastic surgery procedures, patients included those with breast cancer, skin cancers, head and neck cancers, bone cancers and other connective tissue cancers. For the group presenting STIs, patients had necrotizing soft tissue infections (NSTIs) or other less severe infections. Patients admitted for planned reconstructive procedures for other chronic conditions, such as brachial plexus palsy reconstructive procedures, or facial reanimation, were excluded. This was because blood loss in these surgical cases is usually well controlled and minimal and does not tend to be associated with anaemia or require blood transfusions.
For all patients, demographic data (e.g., age and sex) as well as admission characteristics (i.e., length of stay [LOS] in hospital, intensive care unit [ICU] admission and ICU LOS) were extracted from the database. Patient comorbidities were identified using ICD-10 codes and were included in the Charlson comorbidity index (CCI) scoring system.11,12 To account for the diversity in medical conditions, we used the CCI to evaluate the particular burden of comorbidity in these patients.
Details of wound closure procedures (i.e., direct closure, skin grafting, local and regional flaps and free flaps) were extracted and recorded. Other surgical procedures (e.g., debridement, fasciotomy, oncological resections, trauma surgery for upper and lower limb injuries including open reduction and internal fixation (ORIF) of fractures, tendon repair, muscle repair, nerve repair, artery repair and proximal and distal limb amputation and replantation) were also recorded. Haemoglobin (Hb) levels recorded on admission, discharge, average values throughout admission and minimal levels were noted. In transfused patients, minimal Hb levels can act as triggers for blood transfusions. Based on analysis of these Hb levels we identified patients who developed anaemia throughout their admission. Hb cutoff levels were defined in accordance with WHO recommendations (i.e., 12 g/dl for non-pregnant women and 13 g/dl for men). 13
Individual patient in-hospital complications were identified and catalogued. Sepsis was defined in patients presenting organ dysfunction in response to infection based on the Sequential Organ Failure Assessment (SOFA). 14 Acute respiratory insufficiency was recorded in patients who required ICU admission for intubation and mechanical ventilation. Pneumonia was recorded in patients with clinical symptoms and radiological confirmation of consolidation. Patients with renal dysfunction were identified based on the RIFLE (i.e., risk, injury, failure, loss) and KDIGO (kidney disease improving outcomes) criteria.15,16 Hepatic dysfunction was recorded in patients with bilirubin levels above 2 mg/dl.17,18 Wound infections were identified based on microorganisms isolated from surgical sites in correlation with clinical symptoms.19,20 Coagulopathy was recorded in patients with international normalized ratio (INR) > 1.5 and activated partial thromboplastin time (APTT) > 60 s throughout admission.21–23
The reporting of this study conforms to STROBE guidelines. 24 The study obtained formal approval from the Research Ethics Committee of the University of Medicine and Pharmacy “Iuliu Hatieganu”. (Approval no. 144/30.03.2020). Written informed consent was not required due to the retrospective design of the study and patient data were anonymized prior to analysis.
Statistical analysis
All analyses were conducted using the R statistical software (version 4.1.2). A P-value < 0.05 was considered to indicate statistical significance. Categorical variables were presented as absolute counts and as frequencies (%). Continuous variables were described as median (interquartile range), or mean ± standard deviation. For categorical data, comparisons between groups were analysed using Fisher’s exact test and for continuous variables Wilcoxon rank sum tests were used. To identify risk factors for transfusion, anaemia, and other categorical outcomes, logistic regression analyses were performed on items with a P-value < 0.05 and odd ratios (ORs) and 95% confidence intervals (CIs) were calculated.
Results
Of the 350 adult patients included in the study, 228 (65%) presented with acute traumatic injuries, 76 (22%) underwent reconstructive surgery for cancers and 46 (13%) had STIs (Table 1). In total, 175 (50%) patients had anaemia and 37 (11%) received blood transfusions. Of the 37 transfusions, 20 (54%), 5 (14%), and 12 (32%) were for the trauma, cancer and STI groups, respectively. Of the 350 patients, 165 (47%) had a comorbidity, half of whom (81 patients) had a cardiac condition.
Summary of patient characteristics.

Data are expressed as, mean ± standard deviation, n, or n (%) or medians [25th, 75th percentiles].
some patients may have had upper and lower limb amputation
CCI, Charlson comorbidity index; ICU = intensive care unit; LOS, lenth of sty; AKI = acute kidney injury; NSTIs = necrotizing soft tissue infections; HB, haemoglobin; ns, not significant
Most injuries for the trauma patients were domestic incidents (208, 91%), for 11 (5%) patients, injuries occurred in vehicle-related incidents, and for 9 (4%) patients they were work-related. Of the 46% (106/228) trauma patients who developed anaemia, 19% (20/106) received blood transfusions (Table 1). In total, 12% (28/228) patients had upper or lower limb amputations, all developed anaemia and 39% (11/28) were transfused.
Of the 76 (22%) oncologic patients, 32% (24/76) had breast cancer of whom 92% (22/24) had anaemia and one (0.04%) received a blood transfusion (Table 1). Of the 45% (34/76) patients with skin cancers, 21% (7/34) developed anaemia and one was transfused. In total, 8% (6/76) patients had head and neck cancers, of whom, three were osseous and three were non-osseous. Five (83%) of these patients developed anaemia and three (50%) received a blood transfusion. Ten (10/76, 13%) patients had surgery for bone cancers and six (60%) developed anaemia and one was transfused.
Of the 46 (13%) patients that underwent surgery for STIs, 43% (20/46) had NSTIs and 57% (26/46) had other less severe infections. All 20 patients with NSTIs developed anaemia and 10 (50%) were transfused. Nine (9/26, 35%) of the patients with less severe infections had anaemia and two (8%) required a blood transfusion (Table 1).
A comparison of surgical procedures in patients with and without blood transfusions is shown as a graphical presentation in Figure 1. Free flap surgery was performed in 38 (11%) patients. Twenty-four deep inferior epigastric artery perforator (DIEP) flaps were recorded, four of which were bilateral and, in one case, a mastectomy was performed at the same time as the reconstruction. In total, nine anterolateral thigh (ALT) flaps were used for limb reconstruction, two lateral arm flaps (LAF) for hypopharynx reconstruction post-laryngectomy and in one case of functional reconstruction of the upper limb post-sarcoma resection surgery, a gracilis muscle flap was used. In two patients with head and neck defects post-oncological resection, a fasciocutaneous infragluteal (FCI) and deep circumflex iliac artery (DCIA) flaps were performed.
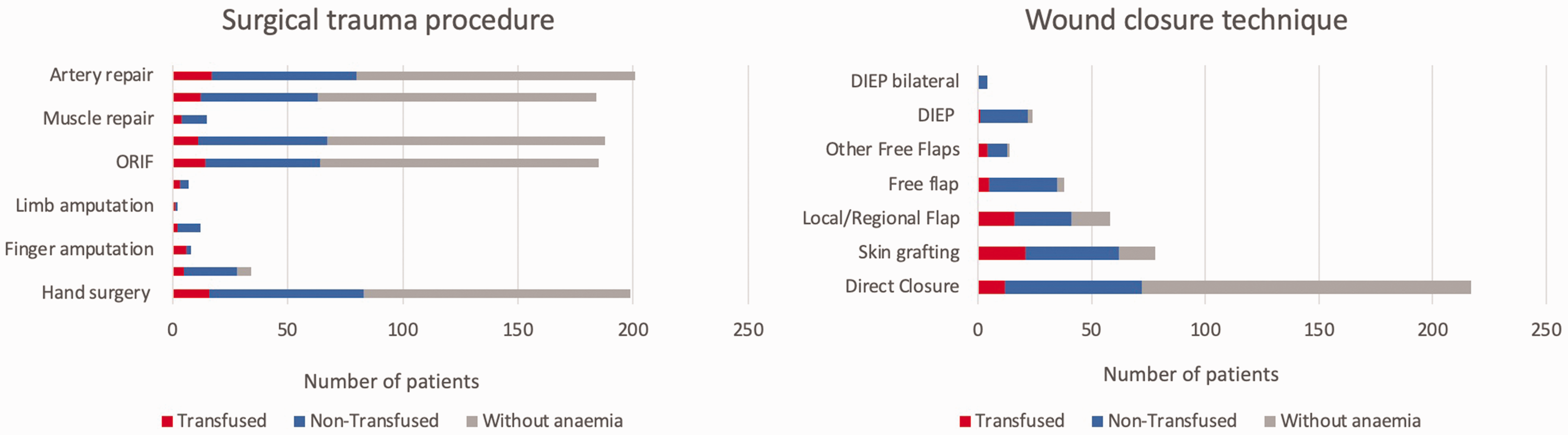
Comparison of surgical procedures in transfused, non-transfused patients and patients without anaemia. ORIF= open reduction with internal fixation, DIEP= deep inferior epigastric artery perforator flap.
Of the 70 patients who had complications, wound complications were the most common (76%, 53/70) and of these 74% (39/53) had anaemia and 32% (17/53) had a transfusion. The median (range) trigger Hb level for transfusion was 7.7 (7.1–8.1) g/dl (Table 1).
In total, 37 patients were transfused with 78 red blood cell (RBC) units (i.e., an average of two units transfused per patient) with a maximum of six units transfused in the case of a trauma patient. A comparison of transfused RBC units per patient by diagnosis, age, sex, and number of surgical procedures is shown in Figure 2.

Comparison of transfused red blood cell (RBC) units by patient diagnosis, sex, age, and number of surgical procedures. Data are shown as mean ± standard deviation.
Logistic regression analysis identified that upper and lower limb surgery and comorbidities were significant risk factors for anaemia (Table 2). An analysis of risk factors for transfusion showed that NSTIs were the most common reason for blood transfusions (OR = 4.98, P = 0.01) (Table 3). With each extra surgical intervention, the odds of requiring a blood transfusion increased more than two-fold (OR = 2.67, P = 0.002). We also identified that direct wound closure represented an independent protection factor for both patients developing anaemia (OR = 0.06, P < 0.001) and the need for blood transfusions (OR = 0.35, P = 0.01).
Risk factors for anaemia.
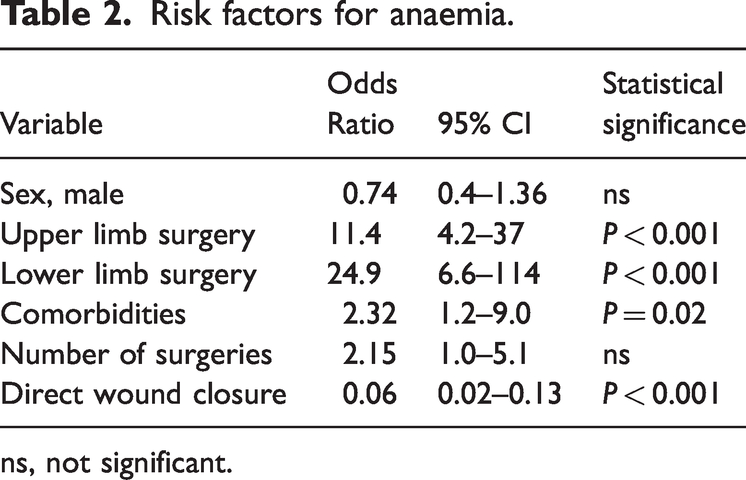
ns, not significant.
Risk factors for blood transfusion.

NSTIs = necrotizing soft tissue infections; ns, not significant.
Logistic regression analysis (data reported in text and not in a table) was performed to ascertain transfusion impact on patient outcome. Adjusting for patient demographics, diagnostic and surgical management, we found that blood transfusions independently increased the risk of overall patient complications (OR = 4.42, P < 0.001) as well as specific complications (i.e., sepsis [OR = 5.22, P = 0.05] and wound complications [OR = 4.50, P < 0.001]).
Linear regression analysis (data reported in text and not in a table) showed that the use of blood products was independently associated with a long hospital stay (OR = 12, P < 0.001). Prolonged hospitalisation was also associated with an increased comorbidity burden (OR = 3.1, P = 0.008), a high number of surgical procedures (OR = 6.1, P < 0.001), traumatic injuries (OR = 6.4, P < 0.001) and infections (OR = 4.7, P = 0.003).
Discussion
Blood transfusions may be necessary during plastic surgery for a variety of reasons, including compensation of blood loss during extensive surgical procedures, maintenance of adequate oxygenation and tissue perfusion during lengthy operations, or correction of anaemia before or after surgery to prevent complications and promote healing. In our retrospective study of data from patients who had undergone plastic surgery, we found that patients who had a high comorbidity burden and underwent more surgical procedures, particularly limb surgery, were more likely to develop anaemia and patients with severe infections and multiple surgical procedures were more likely to be transfused. In addition, we found that blood transfusions increased the rate of complications and prolonged hospital stay.
In trauma, haemorrhagic shock is the primary cause of death. 25 Enhanced resuscitation techniques have been one of the most significant recent advances and continue to be a critical area of investigation. A balanced ratio of RBCs to plasma and platelets is currently the standard of care for resuscitation because it is associated with improved survival. 26 A dose-dependent relationship between transfused blood units and infections has been observed. Advanced Trauma Life Support (ATLS) guidelines recommend the used of aggressive fluid resuscitation combined with massive transfusion protocols, blood recovery techniques and surgical control of blood loss in treating hypovolemic shock. 7 In the setting of severe vascular injury, aggressive crystalloid resuscitation may worsen the trauma associated coagulopathy and as such, massive transfusion protocols have been developed to improve survival rates. 27 The definition of a massive transfusion is controversial. Initially, it was described as the administration of 10 or more RBC units transfused to a patient within 24 hours. However, gradually it has been amended to transfusion of more than four units within an hour with anticipation of more to be required or the replacement of 50% total volume within three hours. 28 In addition to logistical challenges and strain on blood bank services, massive transfusions are associated with the development of coagulopathy, hypothermia and acidaemia. 28 Indeed, shock, tissue injury and haemodilution are the primary causes for trauma related coagulopathy. 28 Several pharmacological agents may be used to mitigate coagulopathy. These include: recombined activated factor VII; prothrombin complex concentrate; antifibrinolytics (i.e., aprotinin, aminocaproic acid and tranexamic acid; fibrin sealants; artificial blood).7,29 In cases of penetrating limb trauma, the use of prehospital and in-surgery tourniquet placement has proven to be effective in decreasing blood transfusion requirements and mortality from haemorrhagic shock in both civilian and military populations. 30 Tourniquets have proved effective without an increase in complications such as nerve palsy or ischemic injury. We found that traumatic limb amputations were correlated with the development of anaemia and the necessity for blood transfusions whether replantation was performed or not. We believe that this may be due to the severity of the haemorrhagic shock. The need for multiple surgeries also independently increased the risk of blood transfusions while direct wound closure represented a strong protective factor for both anaemia and transfusions following multivariate analysis.
In cancer patients undergoing neck dissection, one study found that sex, body mass index (BMI), tumour stage, and type of free flap used for reconstruction, were the strongest independent predictors of blood transfusions in head and neck oncologic surgery.3,31 Another study reviewed data from 585 cases of oral, pharynx, parotid and sinonasal tumours and found that osseous and non-osseous free flaps predicted blood transfusions differently. 32 Similar to our study, while patients undergoing free flap reconstructive surgery were more likely to develop anaemia, the use of free flaps was not a predictor for blood transfusions. 32 A meta-analysis of data from patients who underwent head and neck reconstructive surgery found that the rate of complications was comparable in free flap and pedicled flap reconstructions and that blood transfusions increased the risk of surgical-site infection (SSI), hospital readmission, and hospital LOS but did not affect medical or surgical complications. 33 In data from 136 patients who underwent head-and-neck pedicled flap reconstruction, investigators found no correlation between blood transfusions, flap failure, LOS, or medical problems. 34 These findings are similar to those observed following free flap reconstructive procedures.35,36
Breast reconstructive surgical procedures mainly involve implant-based reconstructions, autologous reconstructions or a combination of both. While it is generally accepted that preoperative anaemia does not lead to increased flap complications in breast reconstructive surgery, postoperative anaemia may be associated with a high rate of medical complications. 37 Reported transfusion rates in patients with breast reconstruction vary. For example, in a large study involving 55,840 patients with autologous breast reconstruction, researchers found transfusion rates of 7%. Most significant risk factors for transfusion were patient-related cardiac comorbidities, diabetes, chronic kidney diseas (CKD), obesity, and chronic lung disease. The researchers also found that patients with blood transfusions had significantly higher complication rates, hospital LOS and overall costs compared with patients who did not receive trnasfusions. 38 By comparison, in a retrospective review of 512 patients undergoing microvascular breast reconstruction, the peri-operative transfusion rate was 0.98% and there was no increase in complications between patients with higher or lower Hb levels. 39 In our study, all 24 patients underwent autologous breast reconstruction with DIEP flaps and while they were associated with anaemia (92%) the transfusion rate was low; only one patient required a blood transfusion (0.04%).
NSTIs are a group of infections characterised by subcutaneous tissue, fascia, or muscle necrosis, associated with high morbidity and mortality. Their aetiology is commonly a mixture of aerobic and anaerobic bacteria but they may also be monomicrobial. Organisms identified in NSTIs include: B-haemolytic streptococcus; methicillin-resistant Staphylococcus aureus (MRSA); Enterococcus species; Clostridium species; Gram-negative bacilli; fungi. 40 NSTIs have been linked to diabetes, age, and comorbidities. 41 One study involving 253 patients with NSTIs found anaemia and blood transfusions predicted poor outcomes. 41 In our study, logistic regression showed that patients with NSTIs were the most likely of several groups of patients to receive blood transfusions, and, in these patients, the risk of transfusions was five times higher when compared to the other groups. Secondary analysis of data from a multicentre, randomized, prospective study of 399 trauma patients, found that blood product transfusions doubled the incidence of nosocomial infections within the first 30 days of hospitalization and were dose-dependent. 42 Another study, involving 697 patients with head and neck cancer undergoing major oncological surgery, found that anaemia, blood transfusions, smoking, drinking, diabetes, previous radio- and chemotherapy, type and duration of surgery, tracheostomy, and clean-contaminated wound surgeries increased the risk of SSIs. 43 Importantly, one report found that women in surgical units were more likely to die from hospital-acquired pneumonia, even after controlling for other comorbidities. 44 We found that blood transfusions were independently associated with high rates of sepsis and wound complications as well as increased length of hospital stay.
Our study was limited by the small number of cancer and SSI patients who received blood transfusions, preventing us from performing separate subgroup analysis. Therefore, a prospective, multicentre study with a large sample size and a long follow-up period is required to validate our results.
Anaemia is a common feature in surgical patients and blood transfusions are often necessary and even lifesaving. However, the use of blood products may lead to complications impacting patient outcome and as such it is important to tailor transfusion rates to specific patient requirements and continuously guide research to promote safe and restrictive clinical practices.
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of Lorand Parajdi in providing support for statistical analysis and data interpretation.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
The work was funded by a PCD grant awarded by the University of Medicine and Pharmacy “Iuliu Hatieganu” Cluj Napoca No. 246/80/17.01.2020 and No. 1033/72/13.01.2021.