
Abstract
Oropharyngeal squamous cell carcinoma is a distinct subtype of head and neck cancer that has become increasingly linked to human papillomavirus over the last four decades. Described is the case of two brothers diagnosed with human papillomavirus-positive oropharyngeal squamous cell carcinoma 6 years apart. The first brother, R.M., presented with an 8-month history of tonsillar swelling, found to be stage III human papillomavirus-positive oropharyngeal squamous cell carcinoma. Despite delayed treatment with chemoradiation, he developed metastatic disease and succumbed to his illness. The second brother, K.M., presented only 3 weeks after the development of neck swelling given his family history, which was also diagnosed as stage III human papillomavirus-positive oropharyngeal squamous cell carcinoma. Following prompt chemoradiation and neck dissection, K.M. has remained in remission for 9 years. Literature has yet to characterize this degree of familial clustering among human papillomavirus-positive oropharyngeal squamous cell carcinomas. Hence, this introduces the possibility of a genetic predisposition to human papillomavirus’s oncogenesis in the oropharynx. This case emphasizes the importance for clinicians to stay vigilant of the family history of human papillomavirus, as well as poses significant implications for future research investigating the interaction of genetic aberrations on human papillomavirus’s oncogenic process.
Introduction
The incidence of the human papillomavirus (HPV) as an etiological contributor to head and neck cancers has been sharply rising each year over the last couple decades. 1 As the majority of middle-aged adults are unvaccinated against HPV, this virus holds considerable oncogenic potential in this age group and has resulted in a 25.1% increase in HPV prevalence found within oropharyngeal squamous cell carcinomas (OPSCC) from 1990 to 2014. 2 To further investigate this linkage between HPV and head and neck cancers, researchers have begun looking into the growing field of genomics. One large meta-analysis revealed a significant association between a function single nucleotide polymorphism (SNP) in an exon of the p53 gene and HPV-positive oral cancer. This SNP, p.Arg72Pro, in p53, displayed increased affinity for HPV’s E6 oncoprotein, thus increasing their binding and subsequent proteasomal degradation of p53. 3 While this study only focuses on genetic aberrations interrelated to HPV in oral cancers, little is known on any genetic susceptibility to HPV in OPSCCs.
To explore a possible genetic predisposition to HPV’s mediated oncogenesis of OPSCC, this article describes the first case reported of HPV-positive OPSCC arising in two siblings. Despite the majority of oropharyngeal cancers occurring in the tonsil, literature has yet to document any instance of siblings both developing OPSCC, of which are both HPV positive. 4 This unique familial clustering serves not only as a strong reminder of the importance of family history in a patient presentation but also offers a path toward finding a new therapeutic against HPV-positive OPSCCs. Interestingly, while HPV-positive OPSCC carries a 58% reduction in risk of death compared to HPV-negative OPSCC tumors, treatment modalities have yet to deescalate alongside this prognosis difference, and the standard of care remains at surgery, radiotherapy, and cisplatin regardless of HPV status. 5 Further research following this case report may result in a discovery of a genetic aberration in OPSCC tumors, and possibly reshaping treatment to be more tailored to HPV status.
Case report
Case no. 1
R.M., a 52-year-old immunocompetent male, presented with an 8-month history of right tonsillar swelling. The patient denied any history of tobacco or alcohol abuse. The patient was initially unaware of any significant family history; however, later learned of his cousin previously having HPV-positive head and neck cancer with otherwise unknown details. Primary care was treated with antibiotics with no improvement. The patient complained of worsening neck soreness and swelling for 3 weeks. He had associated headaches, occasional dysphagia, and right-sided sensitive teeth. Oral examination revealed decreased mobility of the tongue. Computed tomography (CT) of the neck indicated a 4 cm mass in the right tonsillar fossa, extending into the parapharyngeal space, as well as an enlarged right mid jugulodigastric lymph node measuring 2.3 cm (Figure 1(a)). Subsequently, an in-office biopsy of the right tonsillar mass and a fine needle aspiration (FNA) of the right neck mass were performed. Both hematoxylin and eosin (H&E) staining of the tonsil specimen and FNA of the neck mass were consistent with invasive, poorly differentiated squamous cell carcinoma. Immunohistochemical (IHC) studies found that the cells were immunoreactive toward p16, confirming HPV positivity. Following the 8th edition of the AJCC Cancer Staging Manual, these findings together satisfied the staging criteria for prognostic clinical stage III HPV-positive OPSCC given the 4 cm mass invading structures in the parapharyngeal space (T4), the one ipsilateral lymph node under 6 cm (N1), and no metastasis (M0). For reference, prognostic clinical stage group III can be satisfied by these categories: T0N3M0, T1N3M0, T2N3M0, T3N3M0, T4N0M0, T4N1M0, T4N2M0, or T4N3M0. 6 Although images of the H&E and IHC pathology slides were unavailable due to being discarded for age, genotyping did determine HPV16 as the causative agent.
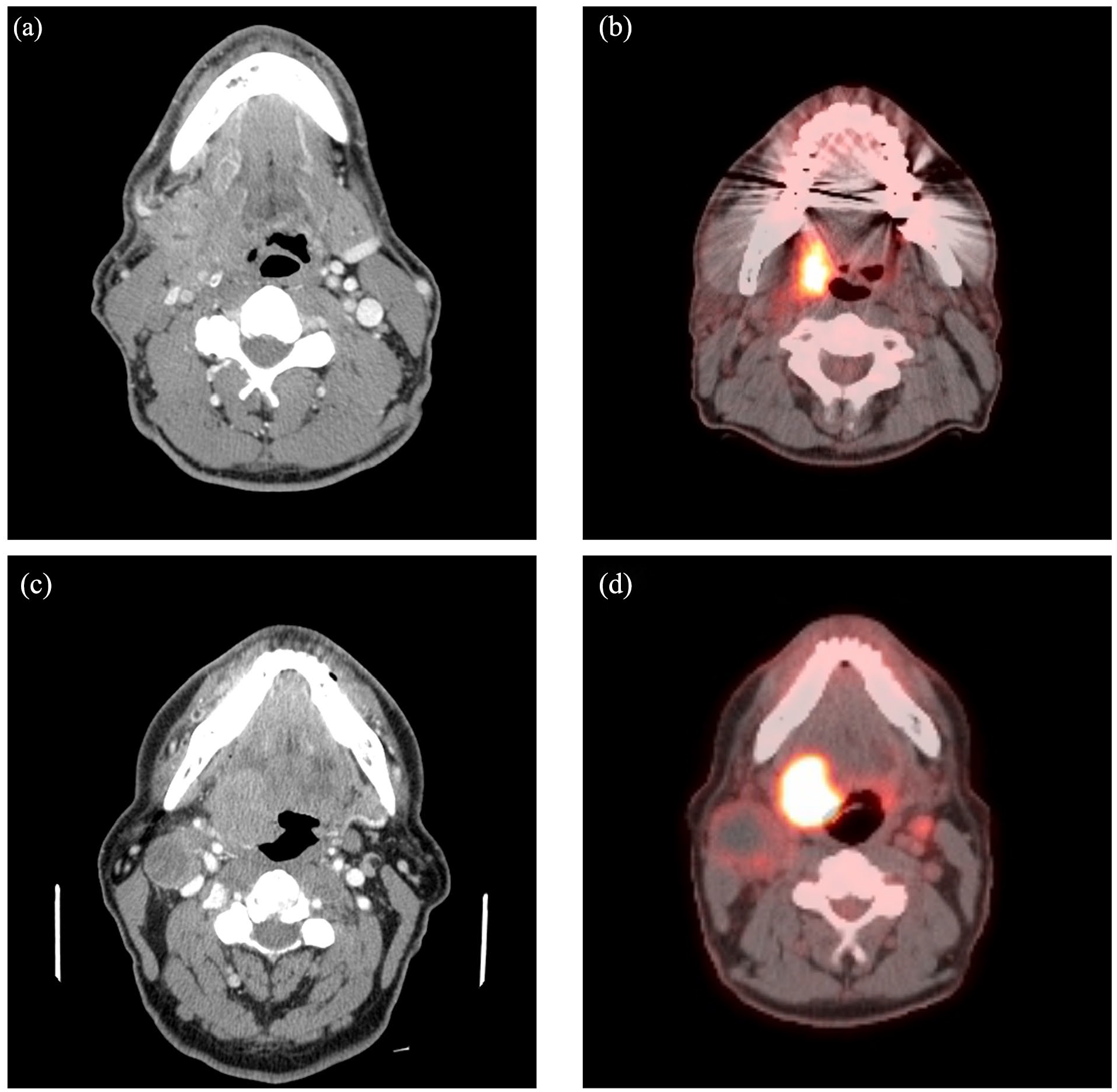
Axial sections of R.M.’s neck computed tomography (CT) (a) and positron emission tomography (PET) scans (b) reveal a 3 cm mass with fludeoxyglucose (FDG) uptake in the right tonsillar fossa extending into the parapharyngeal space. Axial sections of K.M.’s neck CT (c) and PET scans (d) demonstrate a 3.4 × 3.2 cm enhancing mass in the right oropharynx with strong FDG uptake that extends up to the inferior nasopharynx and soft palate.
R.M. then completed three cycles of cisplatin (100 mg/m2) and 70 Gy of intensity-modulated radiation therapy (IMRT) to the oropharynx. While a post-treatment positron emission tomography (PET) scan showed minimal uptake in the right tonsillar region, a follow-up PET scan 6 weeks later demonstrated moderate fludeoxyglucose-18 (FDG) uptake in the right base of the tongue as well as the right tonsillar region (Figure 1(b)). Four months after completing chemoradiation, the patient underwent a repeat biopsy of the right posterolateral tongue, right posterior tongue, right soft palate, and right tonsillar fossa. Pathology was negative for malignancy for all biopsy sites with clear margins. Six months later, the patient had a follow-up head CT only showing mild maxillary and ethmoid chronic sinusitis with no evidence of neoplastic disease or recurrence.
After a year of symptomatic relief, the patient developed dyspnea, chest discomfort, and lower midline neck swelling. In the emergency department, R.M. required thoracentesis for his pleural effusion, from which cytology revealed malignant cells consistent with HPV-positive OPSCC. A repeat PET scan demonstrated a large hypermetabolic cervical lymph node in the anterior aspect of the lower neck, a rind of pleural metastasis along the lower right lateral pleural surface with small metabolic mediastinal lymph nodes, and right metabolic pleural effusion. Given his stage II diagnosis, R.M. began cediranib therapy along with several cycles of taxol and carboplatin. After another year of treatment, neck, abdominal, and pelvis CT showed large pericardial effusion causing restrictive cardiomyopathy and hepatic congestion, a right pleural mass exerting mass effect on the right mainstem bronchus and right pulmonary artery, and left-sided pleural effusion. Unfortunately, R.M. succumbed to his disease shortly after.
Case no. 2
K.M. is the older brother of the previous patient and presented to the clinic 6 years after the death of R.M. This 64-year-old immunocompetent male presented with right neck swelling and associated tenderness for 3 weeks. The patient also denied any history of tobacco or alcohol abuse. During examination, an exophytic right tonsillar mass was appreciated as well as firm swelling of the right lateral neck. CT of the neck uncovered a 3.4 × 3.2 cm mass of the right tonsil and base of the tongue that extended into the inferior nasopharynx and soft palate, alongside a contralateral level 2 lymph node and an ipsilateral level 3 lymphadenopathy measuring 2.5 × 5 cm (Figure 1(c)). Given his family history, he promptly underwent bilateral tonsillectomy and FNA of the right neck mass. The contralateral tonsil was removed to minimize the chance of missing malignant cells given the small risk of synchronous bilateral OPSCCs. Due to the anatomical extension of the tumor, the whole bloc tumor was surgically unresectable, and only friable tissue was removed for histologic examination. As the tumor was received in fragments and not in totality, resection margin status was precluded. Pathology of the tonsil was consistent with squamous cell carcinoma (Figure 2(a)), with IHC staining being positive for p16 (Figure 2(b)), and the HPV16 genotype. Right neck node FNA and a following PET scan (Figure 1(d)) confirmed metastatic involvement of the OPSCC, placing him at clinical stage III (T4 N2 M0) HPV-positive OPSCC.

(a) H&E stain of K.M.’s right tonsil. The section reveals non-keratinizing squamous proliferation, large hyperchromatic nuclei, abundant mitoses, and basal cell morphology. This is consistent with well to moderately differentiated squamous cell carcinomas (200×). (b) Immunohistochemical stain with 3,3′-diaminobenzidine chromogen of K.M.’s tumor exhibiting block-like staining in the basal cell layer, positive for p16INK4a (200×). (R.M.’s pathology slides were unavailable for use.).
K.M. then began concurrent chemoradiation, consisting of 6 weeks of cisplatin (40 mg/m2) and 7 weeks of IMRT. After completion of treatment, the patient’s right neck mass decreased by approximately 50% in size on examination. A PET scan 3 months after chemoradiation showed resolution of prior metabolic activity and a 4.0 × 2.3 × 1.8 cm necrotic lymph node in the right neck with no abnormal activity. Six months after chemoradiation, the patient had a repeat PET scan, still demonstrating an unchanged necrotic lymph node. K.M. then underwent a right neck dissection, which yielded a dense fibrous capsule with lymphoid tissue and no malignant cells identified. The patient has since remained in remission for the past 7 years with no throat symptoms. He has been following up every 6–12 months with visual and endoscopic examination of the oropharynx to monitor for disease recurrence or complications from treatment. As K.M. has been clinically asymptomatic for 7 years and is seen regularly in the practice, imaging is no longer indicated and will continue with routine follow-ups.
Discussion
These cases introduce the phenomenon of HPV-positive OPSCC among brothers, a familial clustering that has yet to be documented in current literature. While these brothers experienced vastly different outcomes following their right-sided tonsillar malignancies, they both received the gold standard of care for OPSCC, a blend of surgery, radiation, and chemotherapy. The key distinction between their stories was how R.M.’s cancer was detected 8 months after the onset of symptoms, while K.M.’s cancer was detected 3 weeks after the onset of symptoms. Due to K.M.’s relevant family history, his primary care physician immediately alerted otorhinolaryngology for consultation, minimizing delay in treatment. Despite both brothers presenting at stage III on initial scans, having an earlier detection likely improved K.M.’s prognostic outcome. This highlights the importance of clinicians maintaining a high index of suspicion for malignancy when presented with an oropharyngeal mass in a patient with no history of smoking or alcohol use, yet a family history of HPV-positive OPSCC.
R.M. and K.M.’s sibling connection also opens a new door, postulating the presence of an underlying hereditary susceptibility to HPV’s oncological process. One large genome-wide association study (GWAS) in Sweden assessed the role host-genetic variations in sisters play in HPV-positive cervical cancer, discovering that inherited genetic variations accounted for 27% of cervical cancer susceptibility with only 2% of the liability of disease being due to shared environment. 7 Furthermore, a large analysis of the Swedish Cancer Registry found a lack of any associations between head and neck cancers and various lifestyle factors. 8
This idea of a possible genetic predisposition to HPV-mediated carcinogenesis holds significant potential, calling for a new therapeutic avenue to be explored. Unfortunately, cisplatin still possesses a grade 3 toxic profile and the leading OPSCC immunotherapy candidate, pembrolizumab, also demonstrated grade 3 or worse adverse toxic events in 55% of patients in their latest phase III trial.9–11 Plus, studies have documented pembrolizumab only having an objective response rate of 15% against head and neck squamous cell carcinomas, with more than 50% of patients still experiencing adverse toxic events.12,13 This leaves a notable gap for HPV-specific immunotherapy to intervene, which is where the story of these two brothers may pose considerable medical promise.
Looking at preclinical data related to OPSCC, one critical gene of interest is TGFβ. Multiple studies have determined that variant T869C of TGFβ is positively associated with HPV-positive OPSCC and found to be overexpressed in these tumors. Notably, a TGFβ polymorphism, rs1982073, demonstrated increased radiosensitivity, thus improving overall survival.14,15 Not investigating these cases’ pathological samples for TGFβ represents one limitation of this case report. As molecular analysis of TGFβ was not considered at the time of patient diagnosis nor was this assay readily available at the tertiary care center at the time, it is the hope of this study for clinicians to consider this genetic test for future patients. Molecular and epidemiological studies are needed to fully analyze polymorphisms in TGFβ and other genes while being conducted through the lens of OPSCC to correlate HPV-positive and HPV-negative statuses. By connecting the underlying biological mechanisms with population data through large GWAS, an understanding of this genetic predisposition to HPV’s oncogenesis could be uncovered. These future studies should possess influential implications for novel immunotherapies against these pathways, all in the hope of de-escalating the standard of care without cost to the patient. Optimizing treatment for HPV-positive OPSCC will be a perpetually evolving endeavor, but begins with implementing safer and more specific treatment alternatives.
Conclusion
This study reports the first documented case of two siblings both developing HPV-positive OPSCC. It stands to reinforce the significance of a positive family history of malignancy in a patient’s presentation. The prompt patient referral and early diagnosis of K.M., influenced by his brother, R.M.’s diagnosis, underscores the impact of familial awareness on clinical outcomes. The story of these two brothers suggests a possible genetic predisposition to HPV-mediated oropharyngeal carcinogenesis and warrants further research into potential genetic factors.
Footnotes
Acknowledgements
The authors would like to thank Dr. Michael Hitchcock for his support. We are also grateful for the family’s willingness to share their story.
Author contributions
All authors contributed to the study’s conception and design. Material preparation and data collection were performed by R.M., C.P., and I.B. Data analysis was performed by M.D., C.J., and D.C. The first draft of the manuscript was written by M.D. and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from a legally authorized representative of the DECEASED subject (Case 1) and from the subject himself (Case 2) for their anonymized information to be published in this article.