
Abstract
Recurrent respiratory papillomatosis is a human papillomavirus-mediated condition characterised by the development of benign squamous papillomata of the respiratory tract. Malignant transformation of recurrent respiratory papillomatosis, while rare, carries a poor prognosis and there are limited data surrounding treatment options, particularly in inoperable disease. We present the case of a 64-year-old male who developed malignant airway obstruction secondary to primary tracheal squamous cell carcinoma in the setting of a 5-year history of recurrent laryngotracheal papillomatosis, requiring placement of tracheostomy while on veno-venous extracorporeal membranous oxygenation. He was managed with cisplatin-based definitive chemoradiotherapy and had a complete metabolic response on post-treatment positron emission tomography/computed tomography, and remains free of recurrent squamous cell carcinoma at 16 months following treatment. This case supports the use of combined chemoradiotherapy as a potential therapeutic option for patients with primary tracheal squamous cell carcinoma, and emphasises the challenges associated with the long-term management of recurrent respiratory papillomatosis.
Keywords
Introduction
Recurrent respiratory papillomatosis (RRP) is a rare human papillomavirus (HPV)-mediated disease of adults and children, characterised by the development of benign squamous papillomata of the respiratory tract. Papillomata most commonly involve the larynx, but can affect the tracheobronchial tree and lung parenchyma. Malignant transformation of RRP is even rarer still, associated exclusively with squamous cell carcinoma (SCC) and occurring in 3%–7% of cases in adults and less than 1% in children.1,2
The aetiologic role of HPV in RRP is well-established, and most commonly associated with the so-called low-risk virotypes HPV-6 and HPV-11.1,3 Due to the refractory nature of the disease, its current management focuses on regular resection of disease, typically with CO2 laser. In a minority of cases, spontaneous remission can occur.3,4 Systemic bevacizumab, a recombinant monoclonal antibody and VEGF-A inhibitor, has shown some promise in small-scale case series as an adjuvant therapeutic for treatment-resistant disease. 5
The exact pathogenesis behind malignant transformation into SCC is poorly understood, but key risk factors include HPV-16 or HPV-18 infection, juvenile onset, smoking, previous radiotherapy or cytotoxic drug use and high disease severity score.2,4,6 Cases with pulmonary involvement appear to have particularly high rates of malignant transformation, at an estimated 16%. 7
Primary subglottic and tracheal malignancies are very uncommon, representing less than 1% of all malignant tumours, with the predominant histology being SCC (45%) followed by adenoid cystic carcinoma (ACC, 16.3%). 8 Current best practice consists of surgical resection where possible,8–11 but owing to their rarity, there are limited data available on optimal management in inoperable cases. We report on our experience with management of a 64-year-old man with unresectable tracheal SCC through the use of cisplatin-based chemoradiotherapy.
Case report
A 64-year-old male presented to a regional emergency department acutely stridulous and short of breath. His medical history was significant for recurrent laryngotracheal papillomatosis associated with HPV-11, diagnosed over 5 years prior and managed jointly by private ENT and thoracic surgeons. He had more than 50 prior laser debulking procedures but no history of irradiation or malignancy. He was an ex-smoker of 50 pack-years with comorbid hypertension and hyperlipidaemia. Computed tomography (CT) of the chest demonstrated a 23 mm× 15 mm endotracheal lesion causing severe tracheal stenosis.
He commenced on adrenaline and dexamethasone while awaiting transfer to a metropolitan tertiary hospital. After transfer, he proceeded to microlaryngoscopy and bronchoscopy while on veno-venous extracorporeal membranous oxygenation (ECMO), due to the inability to safely intubate. The airway was subsequently secured via tracheostomy, and tracheal biopsies were taken. Intraoperative findings included multiple non-obstructive papillomatoid lesions of the supraglottis, vocal cords and subglottis, as well as an atypical circumferential lesion extending from subglottis to 3 cm from the carina (Figure 1). There was no apparent involvement of the main bronchi. He was subsequently decannulated from ECMO and transferred to intensive care unit (ICU) on mechanical ventilation.

Pre-treatment microlaryngoscopy and microlaryngoscopy 1 year after completion of treatment (left and right, respectively).
Histopathology of the tracheal biopsies revealed well-differentiated SCC arising on a background of squamous papilloma. Staging positron-emission tomography (PET) demonstrated intense FDG avidity associated with the circumferential tracheal mass (Figure 2) but no evidence of nodal or distant metastases. After discussion in the hospital’s head and neck oncology multidisciplinary meeting, it was deemed that the disease was inoperable due to its size and concerns regarding feasibility of anastomosis after resection. He was consequently referred for combined chemoradiotherapy.

Axial PET/CT, pre-treatment and 10 weeks after completion of treatment (left and right, respectively).
The patient commenced radiotherapy of 60 Gy over 27 fractions over 5.2 weeks (Figure 3) with high-dose cisplatin (100 mg/m2) in weeks 1 and 4. He tolerated treatment very well, with just the expected painful radiation mucositis and tracheitis necessitating narcotic analgesia. He required a two-night unplanned hospital admission for management of cisplatin-associated anaemia and non-neutropaenic aspiration pneumonia.
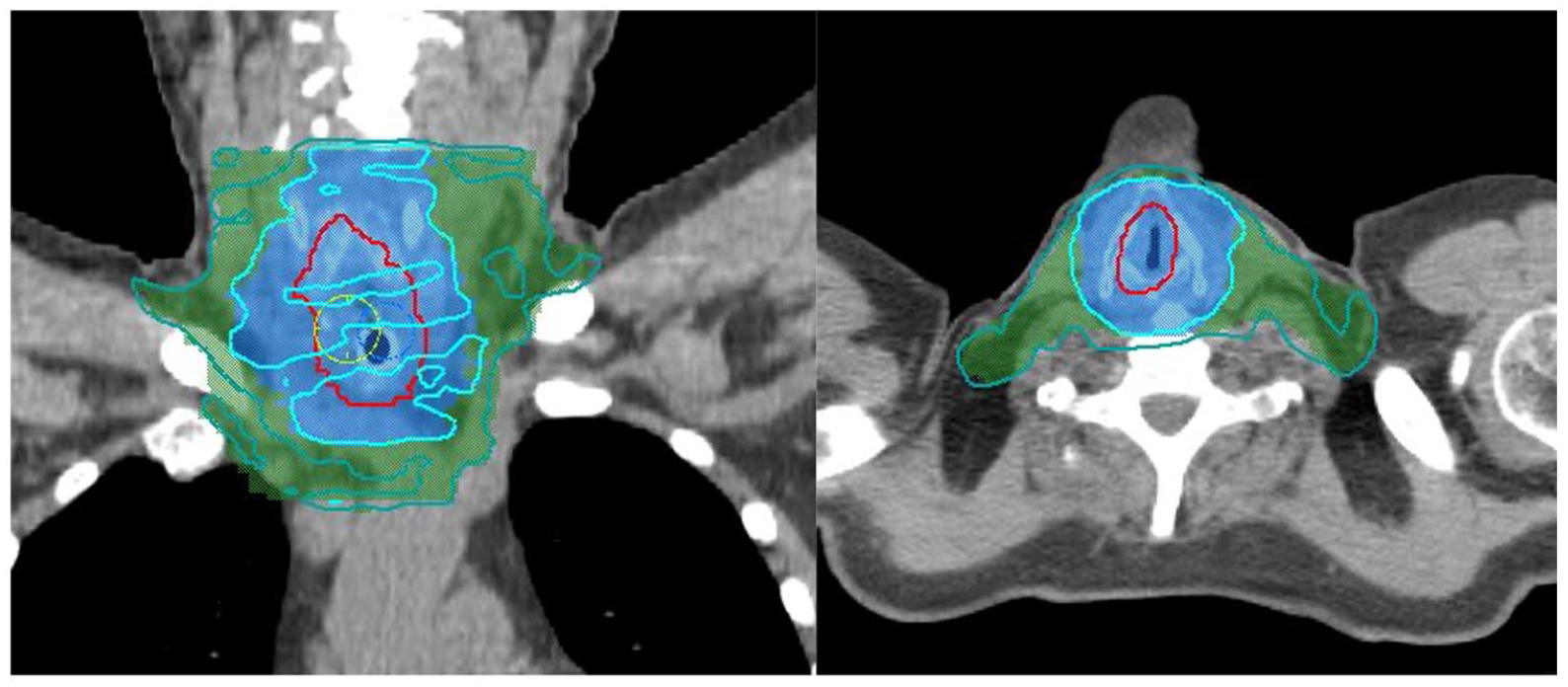
Radiation dosimetry.
Restaging PET 10 weeks following completion of chemoradiotherapy demonstrated marked reduction of metabolic activity in the primary site and no new nodal disease or distant metastatic disease (Figure 1). It was unclear whether the residual FDG avidity was related to inflammation around the tracheotomy site or residual disease. Repeat microlaryngoscopy revealed non-obstructive granulation tissue adjacent to tracheostomy insertion site; biopsy of this site showed no evidence of residual SCC. Two weeks later, the patient was electively readmitted for tracheostomy decannulation on the basis of patient wishes; he was successfully decannulated and discharged home after one night of inpatient observation.
Surveillance microlaryngoscopy and bronchoscopy at 9 months post-completion of treatment demonstrated marked subglottic and proximal tracheal stenosis secondary to irradiation, as well as non-obstructive recurrent laryngeal papillomata. There was no clinical or histological evidence of recurrent SCC (Figure 1). Subsequent to this, he required 3–6-weekly balloon dilation for worsening stridor associated with his airway stenosis. At 13 months following completion of chemoradiotherapy, he required re-tracheostomy for upper airway control of critical subglottic stenosis; repeat biopsy at this time again showed no evidence of malignancy. Definitive management of his proximal tracheal stenosis is necessary before future decannulation can be considered. He remains free of malignant recurrence at 16 months following treatment.
Discussion
Malignant transformation of RRP has historically proven challenging to treat, and its management has only been described in individual case reports. In a similar case of RRP-associated tracheal SCC, Kanazawa et al. 6 reported treatment with primary radiotherapy by accelerated hyperfractionation with good local control, but the patient ultimately died from metastasis to the lung. Another report 12 described use of primary interferon-α2b and cisplatin in a patient with RRP-associated bronchogenic SCC without significant response. Further cases13,14 of RRP-associated pulmonary SCC describe primary surgical approaches to management. To our knowledge, our case represents the first successful use of primary chemoradiotherapy in the management of SCC arising from malignant transformation of RRP. He will require close surveillance for disease recurrence as well as ongoing management of recurrent papillomatous disease and his severe subglottic and proximal tracheal stenosis.
Primary tracheal malignancies are rare, with only 2.6 new cases per 1,000,000 people each year. 8 The associated prognosis is grave. The largest population-based study of primary tracheal carcinoma to date utilised the US-based National Cancer Institute’s Surveillance, Epidemiology and End Results (SEER) database from 1973 to 2004, identifying 578 separate cases; overall 5-year survival was 27.1%, with SCC carrying the worst prognosis with a 5-year survival of only 12.6%. 8 The authors noted a statistically significant improvement in survival with cases that underwent surgery; however, this finding must be interpreted with caution due to the inherent biases in treatment allocation, and thus outcomes in retrospective series. Unfortunately, the database did not capture data about the use of chemotherapy.
Indeed, owing to the rarity of primary tracheal SCC, there are very limited data available surrounding the potential benefit of adjuvant radiotherapy following multiple surgical excisions, or definitive chemoradiotherapy in unresectable disease. There are no prospective studies, with the existing literature consisting entirely of individual case reports and small-scale retrospective reviews.10,11,15–17 Videtic et al. 15 found success in the use of cisplatin-based chemoradiotherapy in a 64-year-old man with primary tracheal SCC. He was administered two cycles for induction, followed by concurrent administration of two further cycles alongside external beam radiotherapy (60 Gy over 30 fractions). He had complete response on post-treatment CT at 6 weeks, and remained disease-free after 2 years. Joshi et al. 17 reported their use of concurrent chemoradiotherapy in a 50-year-old man with basaloid SCC of the trachea, administering a dose of 60 Gy over 37 fractions with seven doses of weekly paclitaxel and carboplatin. Surveillance PET/CT at 2 years following treatment had no evidence of local or distant disease, although he went on to develop bone and lung metastases by the third year of follow-up.
More recently, Jiang et al. 10 observed a 5-year survival of 13.8% in 49 patients with malignant primary tracheal tumours in Changsha, China, identified retrospectively over the period of 2009–2019. The longest survival time was observed in patients treated with complete surgical resection where viable (seven patients, 22.6%). 10 Of the non-surgical group, two received symptomatic treatment only (6.5%), four patients (12.9%) underwent radiotherapy only, eight patients (25.8%) underwent concurrent chemoradiotherapy, and a further eight patients (25.8%) underwent concurrent chemoradiotherapy with additional bronchoscopic intervention. The addition of bronchoscopic intervention had a statistically significant benefit on survival outcomes when compared to chemoradiotherapy alone. Unfortunately, this study also did not capture data about the specifics of chemoradiotherapy regimens, but nevertheless suggests that bronchoscopic intervention may be a useful adjunct in management of patients with inoperable primary tracheal malignancies.
Our choice of chemoradiotherapy regimen, in particular the use of a platinum-based chemotherapy agent, was on the basis of extrapolation from its proven efficacy in other head and neck SCCs. The addition of concurrent cisplatin to radiotherapy has been well-demonstrated to improve locoregional control and overall survival in stage 3 and 4 mucosal head and neck SCCs. 18 Our early success in this case lends further credence to this modality of treatment, and highlights it as an area that warrants further research.
Conclusion
RRP remains a challenging entity to manage with significant associated morbidity. Malignant transformation, while rare, is an important consideration in the long-term management of affected patients. Our preliminary success with the use of combined chemoradiotherapy for the treatment of inoperable tracheal SCC suggests that this is a viable treatment option in this rare disease.
Footnotes
Acknowledgements
The subject of this case report provided written informed consent for its publication, including the use of clinical photography and medical imaging. The authors thank the subject and his family for their support in putting together this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.