
Abstract
Objective
To summarize the clinical features of secondary hyperparathyroidism (SHPT) in patients with chronic renal failure and to explore the predictive factors of postoperative hypocalcemia after total parathyroidectomy in these patients.
Methods
The clinical data of 87 patients admitted to Guangdong Electric Power Hospital from May 2013 to February 2020 were reviewed. All patients underwent total parathyroid resection and sternocleidomastoid microtransplantation. Age, sex, and the serum calcium, phosphorus, alkaline phosphatase (ALP), and intact parathyroid hormone (iPTH) concentrations were analyzed as predictive factors of postoperative hypocalcemia.
Results
Bone pain was the most common clinical manifestation in this study population, and all 87 patients experienced relief from their clinical symptoms after the surgical procedure. Age and the preoperative serum calcium, ALP, and iPTH concentrations were determined to be early predictive factors of postoperative hypocalcemia.
Conclusions
Age and the preoperative calcium, ALP, and iPTH concentrations are independent risk factors for postoperative hypocalcemia in patients with SHPT and renal disease who undergo total parathyroidectomy with sternocleidomastoid microtransplantation. These factors can help identify high-risk patients who can be managed by a multidisciplinary team to improve graft survival and quality of life.
Keywords
Introduction
Secondary hyperparathyroidism (SHPT) is characterized by abnormalities in calcium and phosphorus metabolism, parathyroid hyperplasia, and increased secretion of parathyroid hormone (PTH). 1 The pathogenesis of SHPT involves chronic renal insufficiency, intestinal malabsorption syndrome, Fanconi syndrome, and renal tubular acidosis. 2 In particular, chronic kidney disease (CKD) is common in patients with SHPT who develop vitamin D deficiency and in patients with SHPT who are pregnant and lactating. 3 The prevalence of abnormal blood calcium, phosphorus, and intact PTH (iPTH) concentrations in patients with CKD increases as the disease progresses. 4 Significant increases in the iPTH concentration are significantly associated with increases in mortality, hospitalization, and the incidence of spontaneous fracture. 5 Excessive iPTH concentrations cause serious harm to multiple organs, renal osteopathy, cardiovascular calcification, endocrine system disease, soft tissue calcification, and myelin fibrosis.6,7
Hyperparathyroidism in patients with CKD can generally be controlled with drugs.8,9 However, these drugs have a range of adverse effects, including vomiting and diarrhea, and are not widely used in many countries. 10 In an unadjusted intention-to-treat analysis, cinacalcet did not significantly reduce the risk of death or major cardiovascular events in patients with moderate to severe SHPT who were undergoing dialysis. 11 Because of these adverse effects and certain socioeconomic factors, non-adherence rates for cinacalcet are reportedly quite high.12,13 Furthermore, many patients’ conditions do not adequately respond to the drug.10,11
Surgical treatment is recommended in international and some national practice guidelines for patients with severe SHPT when drug therapy fails or is intolerable because of adverse reactions.14 –18 The three main surgical treatment options are subtotal parathyroidectomy (PTX), total PTX with autologous transplantation (PTX+AT), and total PTX without autologous transplantation. The optimal surgical treatment among these choices remains a matter of debate. 19 Considering the low recurrence rate and easier access to reimplanted glands, we perform total PTX with forearm autologous transplantation in patients at our center.19 –21 According to previous studies, surgery can drastically lower the iPTH concentration, improve control of the serum calcium and phosphorus concentrations, and ameliorate symptoms related to SHPT.22 –26 Unfortunately, postoperative hypocalcemia, also called “hungry bone syndrome” (HBS), is the most serious complication of parathyroid surgery and can lead to death if not immediately treated.16,27,28 Therefore, identification of the predictive factors of HBS are very important to ensure effective postoperative management of these patients.
Although studies have been performed to identify predictors of HBS, they mainly examined predictors one at a time, sometimes controlling for covariates. Integration of multiple risk factors may improve the detection of postoperative HBS.29 –31 In addition, literature focusing on SHPT of renal origin treated with PTX+AT is limited. The present study was performed to investigate the incidence of and risk factors for HBS after PTX+AT for SHPT of renal origin.
Methods
Study design and setting
This retrospective study involved 87 patients with SHPT who were admitted to Guangdong Electric Power Hospital from May 2013 to February 2020. Data collected included age, sex, chief complaint, and routine blood examination (serum) values for calcium, hemoglobin, phosphorus, alkaline phosphatase (ALP), and iPTH determined before the procedure and 2 days, 1 week, 2 weeks, 1 month, 2 months, 3 months, 6 months, and 12 months after the procedure. The patients were divided into an HBS and non-HBS group according to whether the lowest serum calcium concentration was <2.10 or ≥2.10 mmol/L, respectively, on the second day after surgery. Comprehensive data including the preoperative and postoperative serum calcium, phosphorus, ALP, and iPTH concentrations were prospectively collected and retrospectively analyzed. Univariate and multivariate logistic regression analyses were performed to determine independent risk factors for postoperative HBS.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 32 All patient details have been deidentified. All patients were thoroughly informed about the surgical risks, advantages, and procedures, and all provided written informed consent. The requirement for ethics approval was waived by the review board of Guangdong Electric Power Hospital because of the retrospective nature of this study.
Participants
This retrospective study involved 87 patients with hyperparathyroidism who were admitted to Guangdong Electric Power Hospital from 1 January 2013 to 31 February 2020. All of these patients developed renal failure and underwent PTX+AT during the study period. The patients included in this study met the following criteria: (1) persistent hyperparathyroidism as indicated by an iPTH concentration of >800 ng/L; (2) hypercalcemia (serum calcium concentration of >2.5 mmol/L) and/or hyperphosphatemia (serum phosphorus concentration of >1.94 mmol/L) that were not responsive to shock treatment with a standard dose of active vitamin D or other medical treatment; (3) severe SHPT resulting in bone and joint pain, muscle weakness, itching, vascular calcification, fracture, or other complications with a serious impact on quality of life; and (4) ultrasound findings showing that at least one parathyroid gland was enlarged to a diameter of 1 cm or to a volume of >300 mm3, or 99-Tc-MIBI showing a high-density shadow. The exclusion criteria were as follows: (1) severe systemic diseases such as heart, lung, and brain dysfunction; (2) severe coagulation dysfunction; (3) incomplete or missing data; (4) age of <16 years; and (5) a second surgery due to recurrent SHPT following initial PTX+AT.
Surgical procedure
All patients underwent total parathyroid resection and sternocleidomastoid micrograft transplantation under general anesthesia, which was induced by intravenous administration of propofol. This was followed by administration of the muscle relaxants rocuronium and cisatracurium and the analgesic sufentanil. With the patients under anesthesia, a transverse incision was made in the neck, and the upper and lower flaps were separated longitudinally at the midline. The upper and lower poles of the thyroids and the bilateral parathyroid glands were carefully explored, and a nerve detector was used to avoid nerve injury while performing the surgery. Next, the sternocleidomastoid muscle was separated, and two-thirds of the parathyroid tissue was resected and implanted in the sternoclavicular papilla. Smaller grafts with diffuse hyperplasia were selected for transplantation because smaller grafts have a more abundant blood supply and are more likely to survive. The transplantation site was marked with a nonabsorbable line that was easy to detect during follow-up. Moreover, we ensured that no hematoma was present at the transplantation site because this could affect graft survival. Intraoperative transplantation of the parathyroid glands was confirmed by pathological analysis.
Postoperative management
All 87 patients received symptomatic and supportive treatment, including diet control, hemodialysis or peritoneal dialysis, erythropoietin, and antihypertensive therapy. Furthermore, a postoperative drainage tube was routinely placed to ensure that neurological function was not disturbed. Additionally, the patients were monitored for hoarseness or suffocation because these signs could indicate compression of the nerves by a hematoma. All 87 patients were successfully treated with PTX+AT, and no surgical complications such as wound infection, hematoma, or recurrent laryngeal nerve palsy were observed during the follow-up period.
The serum calcium concentration was monitored the day before surgery and the second day after surgery to adjust the calcium supplementation. All patients were empirically treated with intravenous infusion of 40 mL of 10% calcium gluconate on the day of surgery and on the first postoperative day. After the patients had remained stable for 3 to 5 days after the procedure, they were transferred back to the medical ward for treatment and follow-up and managed by a multidisciplinary team. When the corrected serum calcium concentration was maintained at ≥2.10 mmol/L, the calcium supplementation was gradually reduced and replaced with oral calcium carbonate and vitamin analogs. When the corrected serum calcium concentration was stable within the reference range and no hypocalcemia or other surgery-related symptoms were present, the patient was discharged.
Data collection and definition of HBS
Data were obtained from the patients’ medical records. All data were provided in tabular format. The variables for which data were obtained in this study were age, sex, chief complaint, and routine blood examination (serum) values for calcium, hemoglobin, phosphorus, ALP, and iPTH determined before the procedure and 2 days, 1 week, 2 weeks, 1 month, 2 months, 3 months, 6 months, and 12 months after the procedure.
In our center, HBS is defined as a corrected serum calcium concentration of ≤2.1 mmol/L lasting more than 4 days and occurring at any time following PTX+AT despite standard supportive treatment. 19
Statistical analysis
SPSS for Windows, Version 16.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analyses. Quantitative data are expressed as mean ± standard deviation; those with a skewed distribution are expressed as median (range). Categorical data are expressed as number and percentage of cases. Repeated-measures analysis of variance was used for comparison between groups. Multivariate logistic regression with the forward stepwise method and likelihood ratio was then used to determine independent predictors of the occurrence of HBS. A P value of <0.05 was considered statistically significant.
Results
Demographic and clinical data
Table 1 shows the characteristics of the patients with concurrent SHPT and renal disease who were included in this study. The patient cohort comprised 43 men and 44 women with a mean age of 55.72 ± 7.82 years. Of the 87 patients, 78 (89.6%) experienced various symptoms before surgery: bone pain in 56 (64.4%), muscle weakness in 37 (31.0%), and gastrointestinal symptoms in 15 (17.2%) (nausea and vomiting in 10 and constipation in 5).
Perioperative symptoms (N = 87)

Data are presented as number of patients.
All 87 patients were successfully treated with PTX+AT, and no surgical complications such as wound infection, hematoma, or recurrent laryngeal nerve palsy were observed during the follow-up period.
Preoperative and postoperative comparisons at different time points
The changes in the serum iPTH, ALP, calcium, phosphorus, and hemoglobin concentrations before and after PTX are shown in Table 2. Repeated-measures analysis of variance was used for comparison between groups, and the results were corrected using the Greenhouse–Geisser procedure. The iPTH, phosphorus, and calcium concentrations were significantly lower after surgery, whereas the hemoglobin concentration was significantly higher after surgery (P < 0.05). One patient in the graft survival group developed recurrence (recurrence rate of 1.47% within 1 year). The iPTH concentration in this patient returned to the reference range after the second operation, and the recurrence was found to have been caused by graft hyperplasia without residual or ectopic parathyroid glands. Eighteen patients had hypocalcemia on the second day after surgery (20.7% incidence of hypocalcemia).
Preoperative and postoperative comparisons of laboratory parameters at different time points (N = 87)
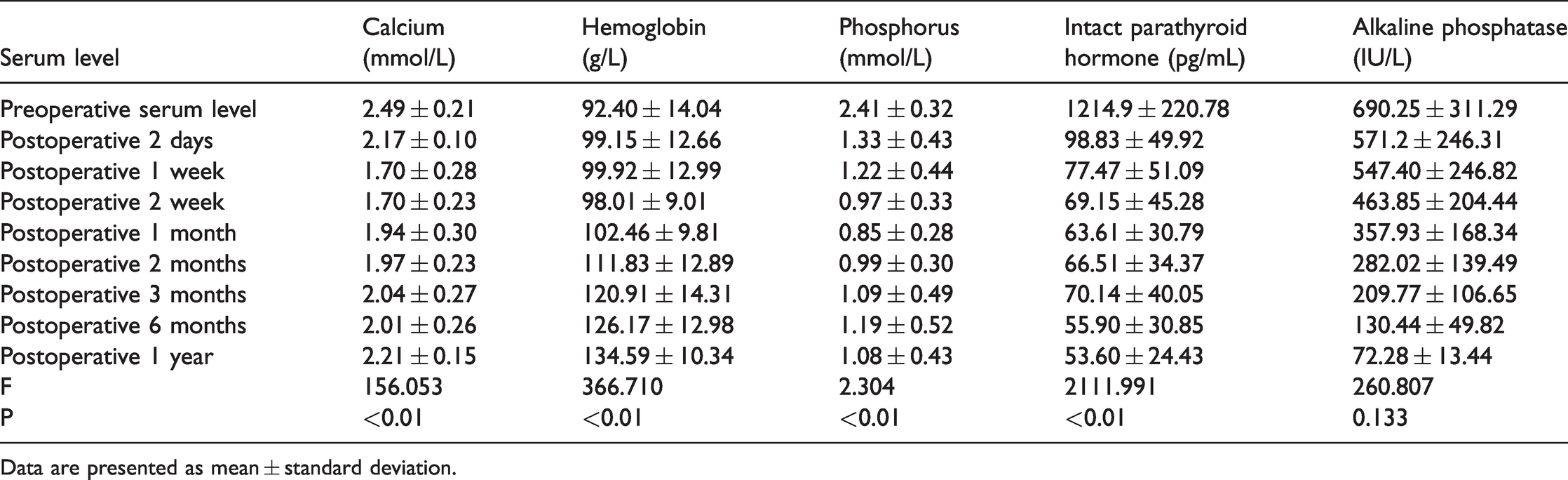
Data are presented as mean ± standard deviation.
Multivariate logistic regression analysis for development of postoperative hungry bone syndrome

SE, standard error; CI, confidence interval.
Predictors of early postoperative hypocalcemia after total PTX for SHPT
Age, sex, and the preoperative serum calcium, phosphorus, ALP, iPTH, and hemoglobin concentrations were used as independent variables for the multiple regression analysis, and the alpha level was set at 0.05. All of the abovementioned significant parameters were then entered into the multivariate logistic analysis (Table 2). The result showed that the following parameters remained significantly associated with the occurrence of postoperative HBS: preoperative ALP concentration [odds ratio (OR), 0.724; 95% confidence interval (CI), 0.548–0.957; P < 0.05], preoperative iPTH concentration (OR, 1.437; 95% CI, 1.024–2.119; P < 0.05), and age (OR, 1.112; 95% CI, 1.016–1.217; P < 0.05).
Discussion
SHPT is a common complication in patients with end-stage renal disease. Severe SHPT causes bone pain, muscle weakness, itching, skeletal malformations, atrophy, restless leg syndrome, sicca syndrome, ectopic calcification, constipation, peptic ulcer disease, spontaneous long fractures, and sleep disorders, thus contributing to poor health-related quality of life in patients undergoing dialysis.24 –26,33 As shown in Table 1, bone pain was the most common clinical manifestation in our study, followed by muscle weakness and nausea and vomiting.
PTX+AT reportedly has good clinical outcomes, such as significant improvement in quality of life, in patients with the appropriate indications.5,34 –38 Furthermore, it can reduce mortality and cardiovascular events.39 –44 The serum calcium, phosphorus, and iPTH concentrations decreased sharply after surgery in our study, consistent with these previous findings.22 –26 The reduction in the iPTH concentration and simultaneous suppression of extraosseous calcification stress via decreased serum calcium and phosphorus concentrations, which favor mineral metabolism, are the most direct mechanism by which PTX+AT may improve survival and cardiovascular outcomes. 45
Regretfully, PTX+AT can also lead to unfavorable conditions such as HBS. HBS is defined as a corrected serum calcium concentration of ≤2.1 mmol/L lasting more than 4 days and that may occur at any time following PTX+AT despite standard supportive treatment.19,29,30 Symptoms of severe hypocalcemia include perioral paresthesia, tingling in the extremities, carpospasm, severe muscle spasm, and/or a positive Chvostek or Trousseau sign. 46 Moreover, HBS can lead to pathologic fracture, coma, and even death if not corrected in a timely manner. 47
The incidence of hypocalcemia in patients with SHPT who undergo PTX reportedly ranges from 20% to 85%.27,30,48 In the present study, 18 patients had developed hypocalcemia by the second day after surgery; the incidence of hypocalcemia was 20.7%. For all patients with SHPT treated by PTX+AT, the K/DOQI Clinical Practice Guidelines for Bone Metabolism and Disease in CKD recommend that intravenous calcium supplementation be initiated immediately after surgery to maintain a normal calcium concentration. When oral medication is available, K/DOQI recommends 1 or 2 g of calcium carbonate (totaling 1.2–2.4 g/day of elemental calcium) three times daily, adjusted to maintain normal calcium ions. 14 In our study, 40 mL of 10% calcium gluconate was given intravenously on the day of surgery and the first day after surgery to prevent a low postoperative calcium concentration.
The above analysis indicates that it is important to predict postoperative hypocalcemia. Although HBS has been reported in prior studies,29 –31 literature focusing on this topic is still limited. Moreover, the risk factors for postoperative hypocalcemia are still controversial19,30; therefore, further research is needed. Risk factors proposed to date include a lower preoperative corrected serum calcium concentration, radiologic evidence of osteitis fibrosa cystica, a higher bone-specific ALP concentration, and a greater weight of the resected parathyroid glands.16,19,48 –50 Our multiple logistic regression analysis showed that the preoperative ALP concentration was an independent predictor of hypocalcemia: a higher preoperative ALP concentration was associated with a higher incidence of postoperative hypocalcemia. In agreement with our findings, patients with a high preoperative ALP concentration are reportedly more likely to develop postoperative hypocalcemia and even HBS.29,33 Therefore, it is strongly recommended that patients with a high preoperative ALP concentration be monitored more closely early in the postoperative period (preferably in a high-dependency ward) and that the serum calcium be frequently monitored to avoid complications associated with early postoperative hypocalcemia. For high-risk groups, postoperative intravenous calcium supplementation should be provided immediately and at a higher dose. Additionally, oral vitamin D and calcium supplementation should be started if possible. 16 Studies have also shown that preoperative treatment with calcitriol can reduce the dose of intravenous calcium required after total PTX by 56% and the length of hospital stay by 50%. 51
The pathogenesis of postoperative hypocalcemia is multifactorial, and one of the main mechanisms might be the sudden removal of iPTH after PTX. This is plausible because patients with SHPT have iPTH concentrations that are associated with high osteoblast activity, high ALP concentrations, and severe bone disease.52,53 However, some studies have shown no association between the preoperative iPTH concentration and early postoperative hypocalcemia.27,33,54 In contrast, our study revealed a positive correlation between the serum iPTH concentration before and after surgery and the development of postoperative hypocalcemia, and this finding is also supported by other studies.27,55 Studies have shown that patients with a 4-hour PTH concentration of ≥10 pg/mL can safely be discharged from the hospital without routine supplementation. Furthermore, calcitriol should be strongly considered in patients with a 4-hour PTH concentration of 5 to 10 pg/mL. 56
Studies have shown that higher patient age is associated with a higher occurrence of postoperative hypocalcemia, 16 and this is consistent with the findings of the present study. Some studies have shown that elderly patients often develop vitamin D deficiency and low oral intake, which might explain why aging is associated with an increased risk of postoperative hypocalcemia. 16 In contrast, some studies have shown that younger patients are more likely to develop postoperative hypocalcemia after total PTX. 56 The reason for this is unclear and must be explored in future studies.
Although several risk factors were detected in this study, the study is limited by it having been performed at a single center and including only 87 patients. This sample size is too small to be representative, and the results of this study might not apply to patients in other medical centers. In addition, this study was retrospective in nature; long-term follow-up data were not evaluated. Thus, further research from multiple centers is needed to support our results.
In conclusion, age and the preoperative serum ALP and iPTH concentrations were found to be independent predictors of postoperative hypocalcemia in patients with SHPT who underwent total PTX. These variables may help clinicians identify patients undergoing hemodialysis who are at higher risk of HBS following parathyroid surgery and thus monitor them more closely during the postoperative period. Such high-risk patients may benefit from postoperative calcium and vitamin D supplementation, and they should be managed by a multidisciplinary team in the medical ward once their condition has stabilized after surgery.
Footnotes
Acknowledgements
The first author also thanks all friends who have put considerable time and effort into providing comments on the draft and to the author’s parents for their continuous support and encouragement.
Author Contributions
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.