
Abstract
We report the case of a woman in her early 30 s who was diagnosed with Robert’s uterus. She had been experiencing progressive dysmenorrhea for a decade and sought treatment for infertility at our hospital. Preoperative ultrasound imaging resulted in a misdiagnosis of a complete uterine septum with an accompanying ovarian cyst. However, intraoperative ultrasound-guided laparoscopy and hysteroscopy confirmed the presence of an asymmetric mediastinal uterus with a blind cavity, consistent with Robert’s uterus, along with endometriosis. We performed a combined hysteroscopy and laparoscopy to excise the septum and endometrial cyst in the uterine cavity, and we inserted a uterine cavity stent to prevent postoperative intrauterine adhesions. Subsequent evaluations confirmed the success of the surgical and postoperative treatment strategies. The findings in this case suggest that despite the risk of a misdiagnosis before surgery, accurate assessment and effective surgical intervention for Robert’s uterus can be achieved by the combined application of hysteroscopy and laparoscopy, with guidance by ultrasound. Furthermore, our findings highlight the importance of addressing concurrent conditions in the management of Robert’s uterus.
Introduction
Robert’s uterus, also known as asymmetric septate uterus, represents a rare Müllerian abnormality characterized by the presence of an asymmetrical septum within the uterine cavity. This condition, which was initially documented by Robert in 1970,1,2 is associated with dysmenorrhea and various reproductive challenges, including recurrent miscarriages, infertility, and pregnancy complications. The management of this condition usually involves surgical intervention with the goal of removing the septum, which can improve the likelihood of a successful pregnancy. 3 We report the diagnosis and surgical treatment of a patient with Robert’s uterus who was in her early 30 s.
Case report
The patient experienced menarche at the age of 12 years, and had a regular menstrual cycle of 30 days with a 5-day duration and a moderate menstrual flow of approximately 30 mL/month. She had a history of severe dysmenorrhea for 5 years and her symptoms had become progressively worse in the most recent 3 years. Initially, the discomfort could be alleviated with rest, but over time, it became increasingly necessary for her to rely on oral painkillers such as ibuprofen for relief. The patient did not undergo any surgical procedures or other pharmacological treatments, apart from the use of oral painkillers such as ibuprofen. Additionally, the patient did not experience amenorrhea and did not receive any emergency interventions for acute pelvic pain.
The patient, who had no history of pregnancy, sought treatment at the hospital in her early 30 s to achieve pregnancy. B-ultrasound showed the following: (1) a potential complete uterine septum; (2) the presence of adenomyosis; (3), and the possibility of bilateral ovarian endometriosis cysts (Figure 1(a) and (b)).
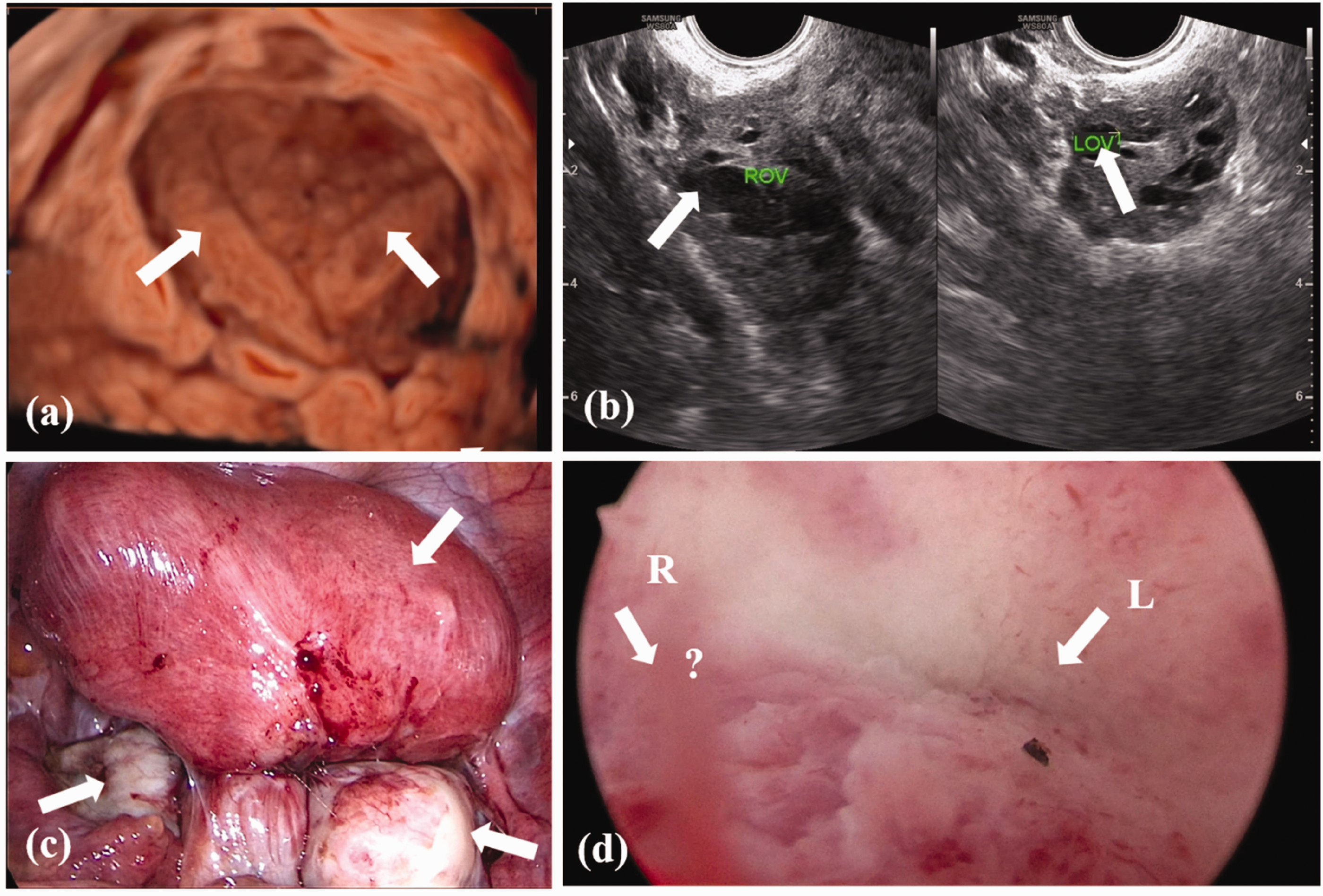
Pre- and intraoperative images. (a, b) Preoperative ultrasound images and (c, d) intraoperative images from laparoscopy and hysteroscopy are shown. (a) Regarding uterine cavity morphology, the uterine cavity is divided into two cavities by the septum. (b) Cysts can be seen in both ovaries. (c) The uterus, bilateral fallopian tubes, and ovaries under laparoscopy are shown. The arrows indicate the presence of uterine and bilateral ovarian cysts and (d) in the left uterine cavity under hysteroscopy, the opening of the left fallopian tube can be seen, while the opening of the right fallopian tube is not observed.
A speculum examination in the lithotomy position showed a long cervix with a partial longitudinal vaginal septum extending from 10 to 13 o’clock. The bottom of the upper and lower channel showed a smooth-surfaced cervix with a diameter of approximately 0.8 and 1.5 cm, respectively. An abdominal examination showed that the uterus was 10 × 9 × 8 cm with a slightly widened base. Regarding the adnexa, a palpable mass of 6 × 5 × 5 cm was detected in the right adnexal region, and the left adnexal region showed thickening. The uterus and bilateral appendages had poor mobility. We considered an ovarian cyst as an independent factor because of the patient’s age and the ultrasound findings that indicated complete uterine septum before the operation. We decided on the diagnosis of a complete uterine septum before surgery.
On the third day after admission, the patient underwent surgical treatment. Laparoscopic surgery was initially performed. During the procedure, we observed dense adhesions between both ovaries and the walls of the uterus, as well as extensive and dense adhesions between the posterior wall of the uterus and the colonic wall. Bilateral ovarian cystectomy and adhesiolysis of the intestinal tract were performed under laparoscopy (Figure 1(c)). We then proceeded with hysteroscopic surgery. The vagina was expanded using a speculum, and the cervical canal at the base of the upper vagina was probed. The probe was able to reach a depth of only 2 cm. The upper part of the cervical canal was not visible, which indicated the presence of cervical dysplasia. We then inserted the probe into the cervical canal of the lower vagina to investigate the depth of the uterine cavity, which measured 9 cm. Hysteroscopy showed an abnormal shape of the uterine cavity, with a thin endometrium, and several polyps measured 0.5 to 0.8 cm in diameter. The lower left side of the uterus showed the opening of the left uterine horn and fallopian tube (Figure 1(d)). However, upon careful examination of the entire uterine cavity and cervical canal, we did not find the opening of the right uterine horn and fallopian tube or any connection with the contralateral uterine cavity (Figure 1(d)). On the basis of these findings, we diagnosed the patient with Robert’s uterus, where the right uterine cavity is a blind end. The right wall of the uterine cavity was incrementally incised under ultrasound guidance. Several endometriosis lesions were identified between the uterine muscular wall, and the incision resulted in the release of brown viscous fluid. The muscular layer was then further dissected towards the lower right side, which was approximately 3 cm thick. Subsequently, the lamellar endometrial tissue became visible upon cutting through the muscular wall. The dissection continued along this plane until the right uterine cavity was exposed. The right uterine horn and fallopian tube opening were visualized in the lower right portion of the uterine cavity, as well as multiple endometrial polyps on the right and posterior walls (Figure 2). The mediastinal surface at the base of the uterus measured approximately 6 cm in width and 7 cm in length. The dissection of the mediastinal surface proceeded until it reached the same level as the oviduct openings on both sides. A uterine cavity stent was inserted to prevent intrauterine adhesion.

Exposed right uterine cavity after dissecting the septum under hysteroscopy.
After discharge, the patient received the first intramuscular injection of 3.75 mg of a gonadotropin-releasing hormone-agonist 4 on the second day of her menstrual cycle, followed by two subsequent injections of 3.75 mg of a gonadotropin-releasing hormone-agonist every 28 days. The initial dose induced a flare effect, which stimulated endometrial growth and further prevented intrauterine adhesions. The subsequent two doses aimed to diminish the likelihood of recurrence of ovarian endometriotic cysts, uterine adenomyosis, and endometrial polyps.
Three months after the surgery, a follow-up hysteroscopy confirmed the proper placement of the uterine cavity stent, wide uterine cavity, and clear visibility of the uterine horns and fallopian tube openings on both sides, with no endometrial polyps (Figure 3). However, minor adhesions were noted at the base of the uterine cavity (Figure 3). The uterine support was removed and the adhesions were carefully separated, resulting in the restoration of the uterine cavity’s morphology. These final follow-up results indicated the success of the surgical and postoperative treatment plan, enabling the patient to prepare for pregnancy.

Morphology of uterine cavity under hysteroscopy after treatment. Hysteroscopy verified the accurate positioning of the uterine cavity stent and the wide uterine cavity, and there was clear visualization of the uterine horns and bilateral fallopian tube openings. Minor adhesions were observed at the base of the uterine cavity and were carefully dissected.
The reporting of this study conforms to the CARE guidelines. 5 We obtained written informed consent from the patient for her treatment and the publication of this case report. Ethics approval was obtained from the Ethics Committee of The Third People’s Hospital of Yunnan Province (approval number: 2021KY022).
Discussion
Robert’s uterus is a rare and unique Müllerian anomaly.6,7 Robert’s uterus is often accompanied by progressive abdominal pain and dysmenorrhea caused by hematometra.2,8 These symptoms are attributed to the presence of partial functional endometrium lining the blind-ended uterine cavity, which connects to the ipsilateral fallopian tube.2,9,10 This configuration leads to the accumulation of menstrual blood in the cavity, causing menstrual pain. Additionally, some of the blood exits into the pelvic cavity via the ipsilateral fallopian tube, contributing to the development of secondary endometriosis, endometriotic cysts, and pelvic adhesion. 11 These factors explain the symptoms, such as dysmenorrhea, bilateral ovarian endometriotic cysts, intestinal adhesions, and adenomyosis, experienced by our patient.
Robert’s uterus is classified under the American Society of Reproductive Medicine Müllerian Anomaly Classification 2021 as a uterine septum. 12 This classification recognizes the presence of a longitudinal septum that divides the uterine cavity, potentially resulting in various reproductive complications. Additionally, according to the recent classification established by the European Society for Gynecological Endoscopy and the European Society of Human Reproduction and Embryology, 13 this type of malformation can be defined as U6, indicating an unclassified uterine malformation. However, some practitioners may define this malformation as a complete septated uterus (U2b), which is characterized by unilateral cervical hypoplasia (C3) and a normal vagina (V0).
Magnetic resonance imaging is the preferred imaging modality for diagnosing Robert’s uterus because it effectively visualizes the uterine diaphragm and hematocele within the uterine cavity. 14 Three-dimensional ultrasound can provide similar imaging results to those of magnetic resonance imaging. However, the gold standard for diagnosis is hysteroscopy combined with laparoscopy guided by B-ultrasound. 15 Hysteroscopic metroplasty, with the assistance of B-ultrasound, can restore the physiological and anatomical integrity of the uterine cavity, thereby enhancing fertility. Laparoscopy can address pelvic adhesions and ovarian cysts associated with Robert’s uterus.
The diagnosis of Robert’s uterus poses challenges, often leading to confusion with other obstructive uterine anomalies, such as a uterine septum and type II residual horn uterus, among others. Robert’s uterus may be misdiagnosed as a complete uterine septum, as was the case in our patient before surgery. Both conditions involve two uterine cavities, but one cavity in Robert’s uterus is blind, 12 complicating differentiation through imaging techniques. Our case shows that, despite potential misdiagnosis before surgery, accurate assessment and effective surgical planning can be achieved through the combined use of hysteroscopy and laparoscopy, with guidance by B-ultrasound during the procedure.16,17 During the operation, hysteroscopy showed a blind uterine cavity, while laparoscopy confirmed the presence of only one uterus in the pelvic cavity. The integration of findings from hysteroscopy and laparoscopy allowed for a definitive diagnosis of Robert’s uterus.
Robert’s uterus presents with symptoms similar to those of a type II residual horn uterus because both conditions possess a blind cavity. 12 Increased pressure within this blind cavity can lead to the reflux of menstrual blood from the fallopian tube into the abdominal cavity, resulting in a series of pathological changes and the onset of dysmenorrhea. 2 The key distinction between these two conditions lies in the structural characteristics:12,13 Robert’s uterus comprises a single, normally appearing uterine structure (as observed in this case, Figure 1(c)), whereas a type II residual horn uterus shows two asymmetrical uterine cavities. Laparoscopy allows visualization of these anatomical differences, facilitating accurate differentiation between the two conditions.
From an imaging perspective, differentiating Robert’s uterus from an accessory cavitated uterine mass presents challenges because of their similarities. 17 Both conditions involve a uterus with a blind cavity that produces menstrual blood. The critical distinction is that menstrual blood from the blind cavity of Robert’s uterus can reflux into the abdominal cavity through the fallopian tube, while this does not occur in cases of an accessory cavitated uterine mass. Consequently, the opening of the fallopian tube is visible in the blind cavity of Robert’s uterus, but not in an accessory cavitated uterine mass. During hysteroscopy guided by B-ultrasound, visualization of the right fallopian tube opening is possible after the uterine septum is removed (Figure 2). Additionally, dysmenorrhea tends to be more severe in patients with an accessory cavitated uterine mass.
In conclusion, the findings in the present case show that, despite the risk of misdiagnosis before surgery, accurate assessment and effective surgical intervention for Robert’s uterus can be achieved through the combined application of hysteroscopy and laparoscopy, with guidance by ultrasound. This case also highlights the necessity of integrating the treatment of Robert’s uterus with concurrent conditions. Furthermore, thoroughly evaluating the risk of postoperative intrauterine adhesions is essential.
Footnotes
Acknowledgements
We thank the patient for her permission to publish this case.
Author contributions
Diagnosis and treatment: Jiying Li, Hongping Yue, Hongwen Hu, and Huanhuan Sheng; data collection: Jiying Li and Hongping Yue; drafting of the manuscript: Jiying Li; critical revision of the manuscript: Huanhuan Sheng and Chengxing Wu; obtaining funding: Yin Li; and approval of the final manuscript: Hongwen Hu.
Data availability statement
Data are available from the corresponding author upon request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Research Foundation of The Third People’s Hospital of Yunnan Province (grant numbers: 2022SSYKT002 and 2022SSYKT015).