
Abstract
Choriocarcinoma is a highly malignant gynaecological tumour. This disease becomes life-threatening once brain haemorrhage or brain herniation occurs. Timely and accurate brain surgery can gain treatment time for patients that have a large number of cerebral haemorrhages and/or brain herniation. This current report describes a case of choriocarcinoma secondary to a hydatidiform mole in a 55-year-old woman that presented with neurological symptoms. Following admission to hospital, computed tomography examination found that lung and brain metastases were accompanied by cerebral haemorrhage. Cerebral hernia occurred during induction chemotherapy treatment and emergency surgery was performed. The patient recovered after individual chemotherapy and rehabilitation treatment. Patients with a very high risk of choriocarcinoma with brain metastasis should be referred to a comprehensive medical centre. Necessary surgical treatment and individualized chemotherapy can reduce the mortality of patients with choriocarcinoma brain metastasis.
Introduction
Choriocarcinoma is a malignant form of gestational trophoblastic neoplasia (GTN). The most common metastatic site for this form of neoplasia is the lung. 1 Primary choriocarcinoma outside the reproductive tract is rare. 1 It can occur in other organs such as the lung, mediastinum, stomach, intestines and retroperitoneum. 2 Primary choriocarcinoma of the gastrointestinal tract has been reported in the literature,3,4 but these publications are case reports suggesting that such cases are quite rare.
Choriocarcinoma develops from villous trophoblast cells and the pathological features of these malignant epithelial tumours include abnormal trophoblastic hyperplasia and atypical hyperplasia. 1 Although brain metastasis rarely occurs, approximately 60% of patients with brain metastasis can have secondary intraparenchymal haemorrhage and the death rate will increase significantly. 5 This current report describes a case of metastatic brain choriocarcinoma with a severe cerebral hernia during treatment that improved after surgery and chemotherapy.
Case report
A 55-year-old Chinese woman was admitted to the neurology ward at The First Affiliated Hospital of University of Science & Technology of China, Anhui Provincial Hospital, Hefei, Anhui Province, China in May 2018. The patient presented with sudden numbness and weakness of her left limbs due to right parietal haemorrhage verified by computed tomography (CT) imaging of the brain. The serum level of β-human chorionic gonadotrophin (β-hCG) at admission was 395 974 IU/l. The patient indicated that this symptom arose after washing her hair 2 days previously. This patient (gravida 5, para 2) had a history of hydatidiform mole pregnancy in September 2016 and she underwent bilateral salpingo-oophorectomy and hysterectomy at the local hospital with a serum β-hCG level greater than 200 000 IU/l. The postoperative pathology suggested a hydatidiform mole. After surgery, she was treated with 50 mg/m2 methotrexate intramuscular (i.m.) injection given once every 3 weeks and repeated seven times, but was lost to follow-up shortly after biochemical remission was obtained without any further cycles of chemotherapy. After treatment, the patient did not go to the hospital for regular review from 2016 until the occurrence of the symptoms reported here.
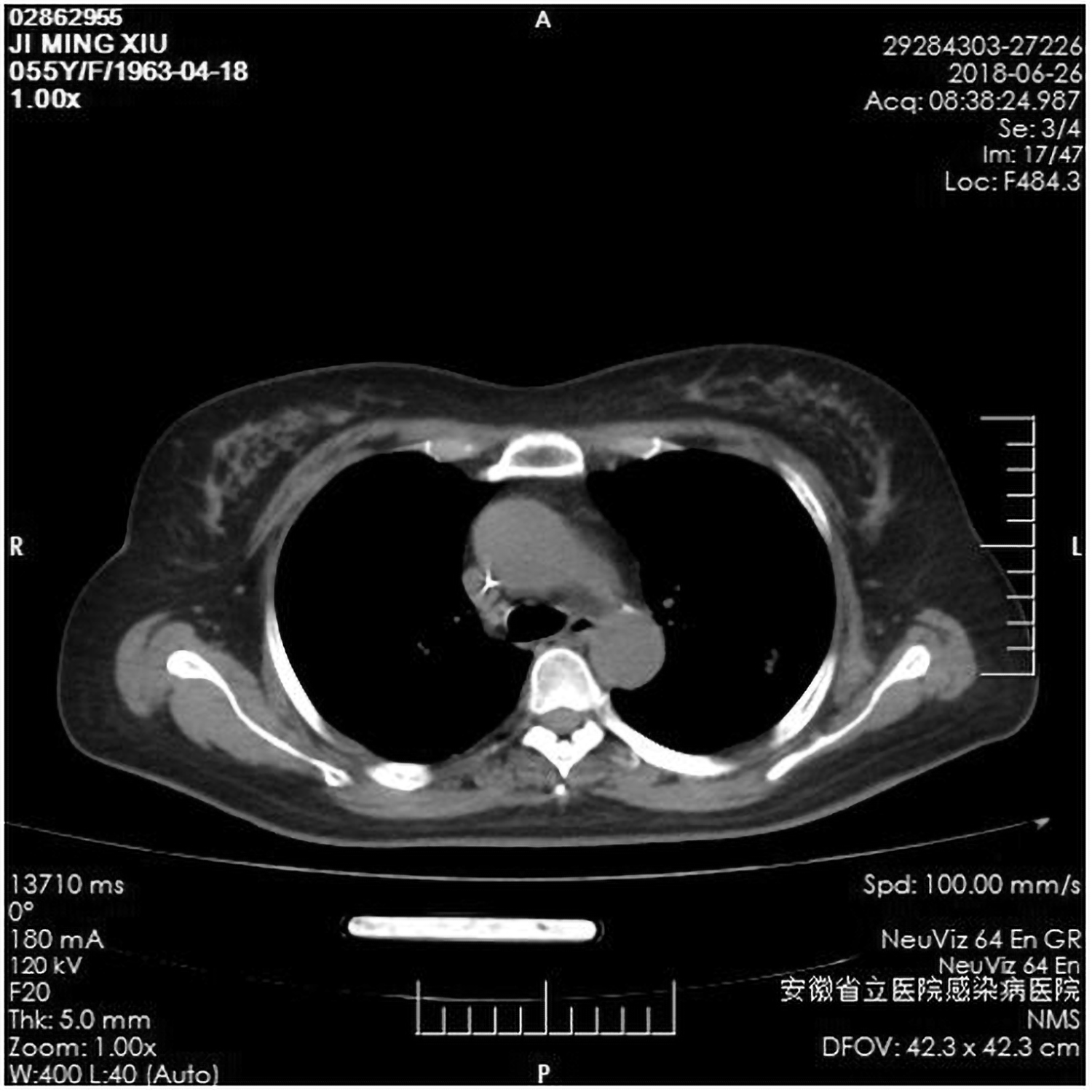
The patient was transferred to the Department of Obstetrics and Gynaecology, The First Affiliated Hospital of University of Science & Technology of China, Anhui Provincial Hospital, Hefei, Anhui Province, China with a diagnosis of choriocarcinoma with brain metastasis (IV: 15) in May 2018. CT imaging demonstrated that multiple circular soft-tissue changes were scattered in the left lung and there was a right parietal cerebral haemorrhage in the brain (Figures 1 and 2). According to National Comprehensive Cancer Network® guidelines, if there is extensive metastatic disease with a prognostic score ≥ 12, it is recommended to perform a modified treatment with the etoposide and cisplatin (EP) induction regimen using 100 mg/m2 etoposide intravenous (i.v.) and 20 mg/m2 cisplatin i.v. once daily on days 1 and 2 repeated weekly for 1–3 weeks prior to the start of the etoposide, methotrexate, actinomycin D, cyclophosphamide and vincristine (EMA-CO) regimen. The chosen treatment regimen was initially 100 mg/m2 etoposide i.v. and 20 mg/m2 cisplatin i.v. once daily on days 1 and 2. On the second day of chemotherapy with the EP regimen, the patient suddenly developed severe vomiting, sweating, paleness, and subsequently the patient lost consciousness. The patient had a dilated pupil on the right and her reflection of light disappeared. She immediately received an emergency CT scan. She was still vomiting during the scan and continued to be in a coma. The CT imaging indicated that the bleeding in the right parietal tumour was significantly increased compared with the previous scan taken upon her first admission, which suggested a brain hernia (Figure 3). Emergency decompression using a craniotomy bone flap and resection of the metastatic tumour was performed. During the operation, the cerebral pressure was extremely high. After cutting the dura mater, a haematoma was seen to rupture from the cortex. The surgeon removed approximately 60 ml of haematoma and noted that the tumour tissue was soft. The tumour was completely resected along with the surrounding oedema zone (Figure 4). Due to the patient’s critical condition following surgery, the patient was transferred to the intensive care unit (ICU). The serum β-hCG level rose to 450 673 IU/l on the day of the surgery. The day after the surgery, the patient received continual induction chemotherapy with the EP regimen (100 mg/m2 etoposide i.v. and 20 mg/m2 cisplatin i.v. once daily on day 2. The tracheal intubation was removed the next day in the ICU after the patient regained consciousness. At that time, the pupils were equally contoured on both sides and the left limb muscle tension was level 0. The patient was subsequently moved out of the ICU.
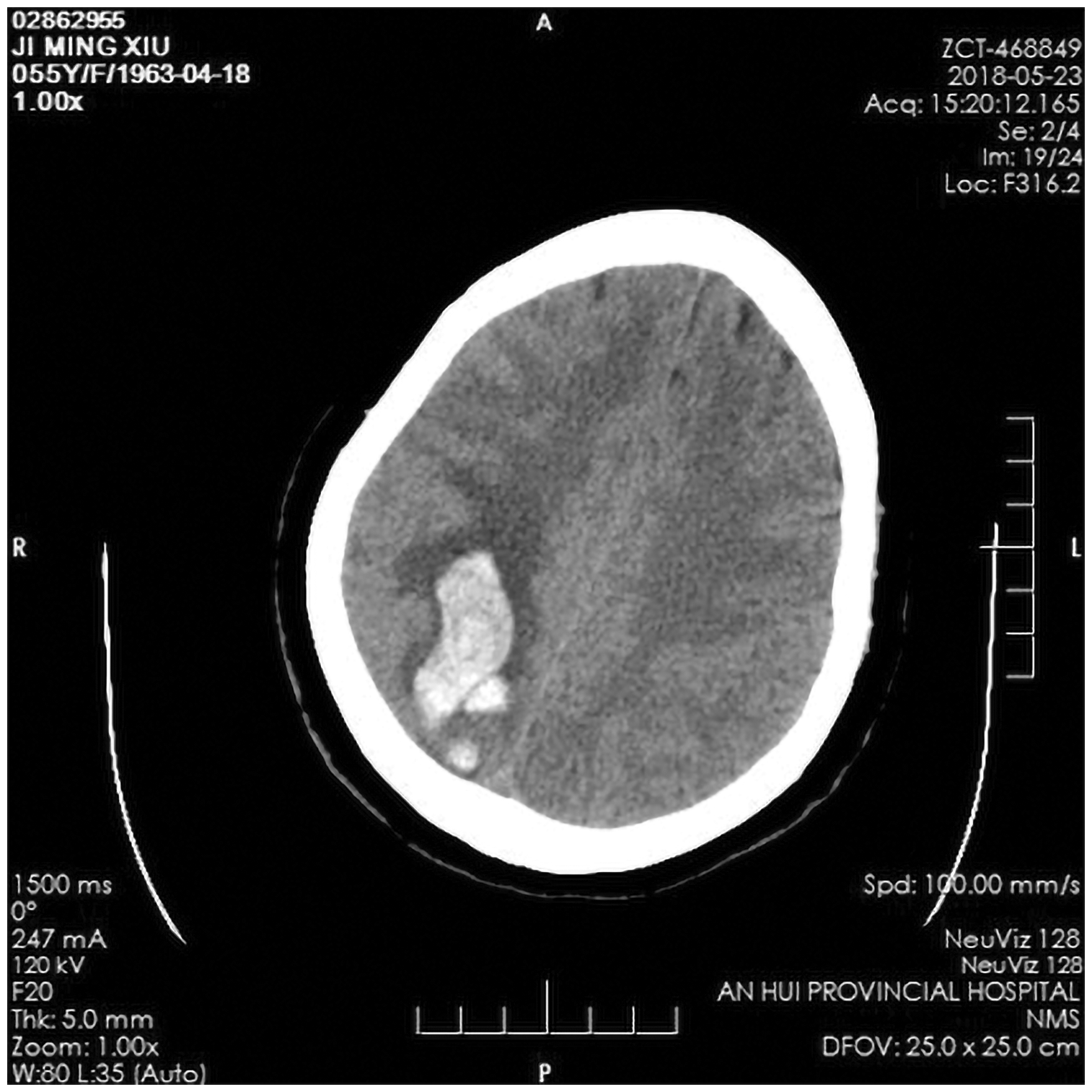
Computed tomography imaging of a 55-year-old Chinese woman that presented with sudden numbness and weakness of her left limbs on admission showing a right intracerebral haematoma.

Computed tomography imaging of a 55-year-old Chinese woman that presented with sudden numbness and weakness of her left limbs on admission showing a left lung metastasis.

Computed tomography imaging of a 55-year-old Chinese woman that presented with sudden numbness and weakness of her left limbs on admission showing increased cerebral haemorrhage after initiation of chemotherapy, which suggested a brain hernia.

Photograph of the excised brain tissue from a 55-year-old Chinese woman that presented with sudden numbness and weakness of her left limbs on admission. The colour version of this figure is available at: http://imr.sagepub.com.
A week later, the patient received a second cycle of the EP regimen (100 mg/m2 etoposide i.v. and 20 mg/m2 cisplatin i.v. once daily on days 1 and 2 over a 1-week interval). The postoperative pathology indicated brain metastasis of choriocarcinoma (Figures 5 and 6) and a craniotomy CT scan showed that the focus area of haemorrhage disappeared and was low-density and softened (Figure 7). The patient suddenly developed a cough and a sputum culture test revealed a Klebsiella pneumoniae and Acinetobacter baumannii infection, which were multidrug resistant bacteria. The antibiotic amikacin was used to treat this infection (0.8 g amikacin i.v. once daily for 10 days). Low activity, colour ultrasound of both lower extremities suggested intermuscular venous thrombosis, so the patient was then given 4000 IU low molecular weight heparin subcutaneous injection once daily for 20 days. After consultation with a rehabilitation doctor and the multidisciplinary team, the patient received rehabilitation exercises such as practiced breathing training, comprehensive training of left hemiplegia limbs, swallowing therapy, posture adaptation training, sitting training and daily living ability training. Considering the lung infection and venous thrombosis, the patient was given a third cycle of the EP regimen (100 mg/m2 etoposide i.v. and 20 mg/m2 cisplatin i.v. once daily on days 1 and 2 over a 1-week interval). After this, CT imaging showed that the lung lesions were significantly reduced (Figure 8). Meanwhile, after antibiotic treatment, the rehabilitation therapy significantly improved the symptoms of cough and expectoration. The serum levels of β-hCG declined to 2971 IU/l. After three cycles of chemotherapy, the conventional EMA-CO regimen was not selected but the patient was given a 5-day standard EP regimen (100 mg/m2 etoposide i.v. and 20 mg/m2 cisplatin i.v. once daily on days 1–5 over a 3-week interval). 6 As the patient's lung infection was not completely cured at this time, it was thought that the use of the EMA-CO regimen would likely cause severe bone marrow suppression and induce sepsis. At the same time, it was difficult to determine when the EP chemotherapy regimen could be replaced by the EMA-CO regimen. It was decided that the patient should continue to receive the 5-day EP chemotherapy regimen as recommended by Peking Union Medical College Hospital. Blood tests were undertaken on the third day to determine if there was bone marrow suppression as the chemotherapy could be suspended at any time. A week later, the serum β-hCG level was 297.73 IU/l. Although the decrease in β-hCG was satisfactory, the patient experienced severe bone marrow suppression, including reduced white blood cells (1.31 × 109/l), platelets (37 × 109/l) and haemoglobin (56 g/l). Because of the significant reduction in platelets, the low molecular weight heparin treatment was temporarily discontinued. After giving the patient 75 µg granulocyte-monocyte colony-stimulating factor i.m. once daily on days 1–3, and blood and platelet transfusions, her condition improved.

Representative photomicrograph of the excised brain tissue from a 55-year-old Chinese woman that presented with sudden numbness and weakness of her left limbs showing typical polygonal cells in the haemorrhagic tissues, with obvious cell atypia (haematoxylin and eosin staining). The colour version of this figure is available at: http://imr.sagepub.com. Scale bar 50 µm.

Representative photomicrographs of the excised brain tissue from a 55-year-old Chinese woman that presented with sudden numbness and weakness of her left limbs showing the results of immunochemical staining: β-human chorionic gonadotrophin-positive (a), CD10-positive (b) and Ki67-positive (60%) (c). The colour version of this figure is available at: http://imr.sagepub.com. Scale bar 50 µm.

Computed tomography imaging of a 55-year-old Chinese woman that presented with sudden numbness and weakness of her left limbs on admission. Imaging at 2 weeks after surgery that showed that the bleeding had disappeared in the focus area and the focus area showed a low-density softened shadow.
Computed tomography imaging of a 55-year-old Chinese woman that presented with sudden numbness and weakness of her left limbs on admission. Imaging after three cycles of the etoposide and cisplatin induction chemotherapy regimen showing that the pulmonary lesions were reduced significantly.
After rehabilitation treatment, the patient’s left upper limb muscle strength became level 2 and her left lower limb strength level 1. After the fifth round of the EP regimen (100 mg/m2 etoposide i.v. and 20 mg/m2 cisplatin i.v. once daily on days 1–5 over a 3-week interval), the serum β-hCG level had reached the normal range (12.66 IU/l) and she was discharged. Chemotherapy was delivered according to these standard protocols and for a further three cycles of consolidation chemotherapy after the serum β-hCG level reached the normal range (Table 1). After rehabilitation training, the patient could walk on her own and her neurological status was completely normal. Moreover, examination of the veins of both lower extremities indicated that blood flow in both lower extremities was smooth. During regular follow-up, the patient has had normal serum β-hCG levels, is generally in good condition and has returned to a normal life. At present, the patient is 1 year and 10 months without relapse.
Laboratory tests and clinical data during the treatment for a 55-year-old Chinese woman that presented with sudden numbness and weakness of her left limbs.

β-hCG, β-human chorionic gonadotrophin; CT, computed tomography.
Discussion
Gestational trophoblastic neoplasia often develops aggressive and extensive metastasis with approximately 30% of GTN patients diagnosed with metastases in other organs.7,8The International Federation of Gynecology and Obstetrics (FIGO) 2015 Cancer Report proposed an ultra high-risk GTN category based on the following criteria: FIGO prognosis score ≥12 points and liver or brain metastasis or patients with extensively transferred GTN. 9 Ultra high-risk GTN patients are classified because of poor treatment and high mortality. 9 The principal causes of death in high-risk GTN patients are: (i) extensive drug-resistant lesions; (ii) lung infections and respiratory failure caused by the progression of lung lesions; (iii) massive bleeding in the lesions including intracranial haemorrhage and hepatic metastasis rupture bleeding. 10 A previous study suggested that gestational trophoblastic diseases with a FIGO score ≥13 had an increased risk of early death. 11 These patients should be treated in a highly specialized gestational trophoblastic disease centre. The treatment principle for ultra high-risk GTN patients remains primarily composed of systemic chemotherapy, supplemented by surgery, radiotherapy or interventional therapy. 12
Brain metastasis from malignant trophoblastic tumours is not uncommon and the literature reports incidence rates ranging from 8% to 28%. 13 The diagnosis of brain metastasis in patients is not difficult due to the associated clinical symptoms and corresponding auxiliary examination measures. The occurrence and development of choriocarcinoma brain metastasis can be divided into three stages: (i) tumour thrombus stage (initial stage); (ii) brain tumour stage (advanced stage); and (iii) cerebral hernia stage (end stage). Through this understanding, the early diagnosis rate and cure rate of brain metastasis in patients with choriocarcinoma has been improving. 13 Multidrug combination systemic chemotherapy, combined with intrathecal chemotherapy, remains the main treatment approach for brain metastasis. 13 As the brain tumour stage continues to develop and the intracranial pressure continues to rise, the patient will enter the cerebral hernia stage. To prevent the occurrence of cerebral hernia, the patient should be actively treated to reduce the intracranial pressure. While it is difficult to achieve the effect of lowering intracranial pressure with active medical treatment, or if there is increased cerebral haemorrhage and coma, emergency craniotomy can be used to enable patients to receive continual chemotherapy. Craniotomy plays an important role in some patients. The treatment of intracranial haemorrhage or an intracerebral haemorrhage crisis should not be given to patients with intracranial metastases. 5 A combination of surgical resection and chemotherapy can improve prognosis and survival. 14 A previous study showed that the incidence of brain metastasis from malignant trophoblastic tumours ranges from 6.3% to 8.5%. 15 Moreover, this disease form is dangerous and can easily lead to brain hernia and death. 14 Patients with high-risk gestational trophoblastic tumours usually receive chemotherapy with EMA-CO (i.e. etoposide, methotrexate and actinomycin D with cyclophosphamide and vincristine).16,17 This regimen was initiated by Charing Cross Hospital, UK and is mainly used for high-risk and/or drug-resistant cases. 6 Methotrexate is frequently used and attention must be paid to hydration and the use of calcium folinate for detoxification when needed. For patients with choriocarcinoma and solitary brain metastasis, craniotomy can be considered, followed by EMA-CO and high-dose intravenous methotrexate treatment. 18 Some studies suggest that craniotomy or stereotactic radiosurgery combined with etoposide, cisplatin and medium/high-dose methotrexate combined with chemotherapy can stabilize patients in the early stage of treatment and avoid whole brain radiotherapy or intrathecal chemotherapy.19,20
A previous study reported that among 140 newly admitted high-risk patients with GTN admitted to the Charing Cross Centre, UK from 1995 to 2010, 33 of the very high-risk patients with a high tumour burden were given a low-dose EP transition before starting EMA-CO chemotherapy. 21 These investigators noted that the early mortality rate in 140 patients was only 0.7%, while the early mortality rate of the 151 high-risk patients who were not given low-dose EP regimen before 1995 was 7.2%. 21 The authors also found that in high-risk patients, induction chemotherapy using EP regimens reduced early mortality. 21 Another study also reported that extremely high-risk patients could benefit from the use of induction low-dose etoposide and cisplatin. 11 In this current case, the EP regimen was first adopted as induction chemotherapy and the patient experienced a sudden and dangerous brain hernia during treatment, which was deemed to be seriously life-threatening. A craniotomy was performed to save the patient' s life. Following this, the patient developed severe bone marrow suppression and infection with multidrug resistant bacteria during EP induction chemotherapy. If the patient had been changed to the traditional EMA-CO chemotherapy regimen at this time, they might have experienced comorbidities, many of which might have been intolerable and could have led to early death. Therefore, the patient continued to receive the EP regimen and there was a satisfactory decrease of serum β-hCG level after chemotherapy. A retrospective study found that GTN patients with brain metastases had a high survival rate with intravenous multidrug chemotherapy, without the need for whole-brain radiotherapy. 22 If indicated, emergency brain surgery could be performed for severe neurological symptoms. In our clinic, the EMA-CO regimen combined with intrathecal methotrexate injection is used in patients with brain metastases but without cerebral haemorrhage and the effects are generally quite good.
In conclusion, if brain hernia occurs in patients with brain metastases from primary trophoblastic tumours then the disease is likely to develop rapidly, making rescue difficult and the risk of death extremely high. Usually, the patient dies from respiratory arrest during cerebral hernia. Emergency craniotomy combined with chemotherapy is an important way to save the life of patients with cerebral hernia formation. For these very high-risk patients, the chemotherapy regimen should be individually selected according to the situation presented. It is likely that the delivery of prompt care in specialized centres using brain surgery to relieve intracranial pressure, together with EP induction chemotherapy, can help to reduce early mortality.