
Abstract
The present study reports a rare case of a 65-year-old male patient with an exophytic ulcerative lesion in the gastric antrum. After performing a radical subtotal gastrectomy with D2 lymph node dissection and Billroth I gastrojejunostomy, histological analysis revealed a poorly differentiated adenocarcinoma combined with a biphasic pattern consisting of cytotrophoblasts and syncytiotrophoblasts. Immunohistochemical analysis showed a positive reaction with an anti-β-human chorionic gonadotropin antibody, and an abnormal increase in reproductive hormones. Furthermore, the patient succumbed to upper gastrointestinal hemorrhage in less than 3 months after the initial diagnosis, although the rupture of his liver metastasis was successfully treated by transhepatic artery embolization during the second admission.
Keywords
Background
Choricarcinoma is a rapidly progressive, widely metastatic, β-human chorionic gonadotropin (β-hCG)-secreting neoplasm, 1 which typically occurs in females at the origin of the chorionic epithelium of the placenta, and is commonly correlated with gestation. 2 However, it can also occur as a non-gestational malignancy, which can be gonadal or extragonadal in origin. Primary gastric choriocarcinoma is a rare tumor that accounts for approximately 0.08% of all gastric cancers. Similarly, choriocarcinoma of the testis accounts for only 0.9% of testicular tumors, 3 and gastric metastases deriving from the testes are rare. The traits of latency and high malignancy often make it difficult to obtain an early accurate diagnosis, resulting in the best treatment opportunity being missed. 4 The present study reports a 65-year-old male patient with gastric choriocarcinoma combined with a poorly differentiated adenocarcinoma component and reproductive hormone secretion.
Case presentation
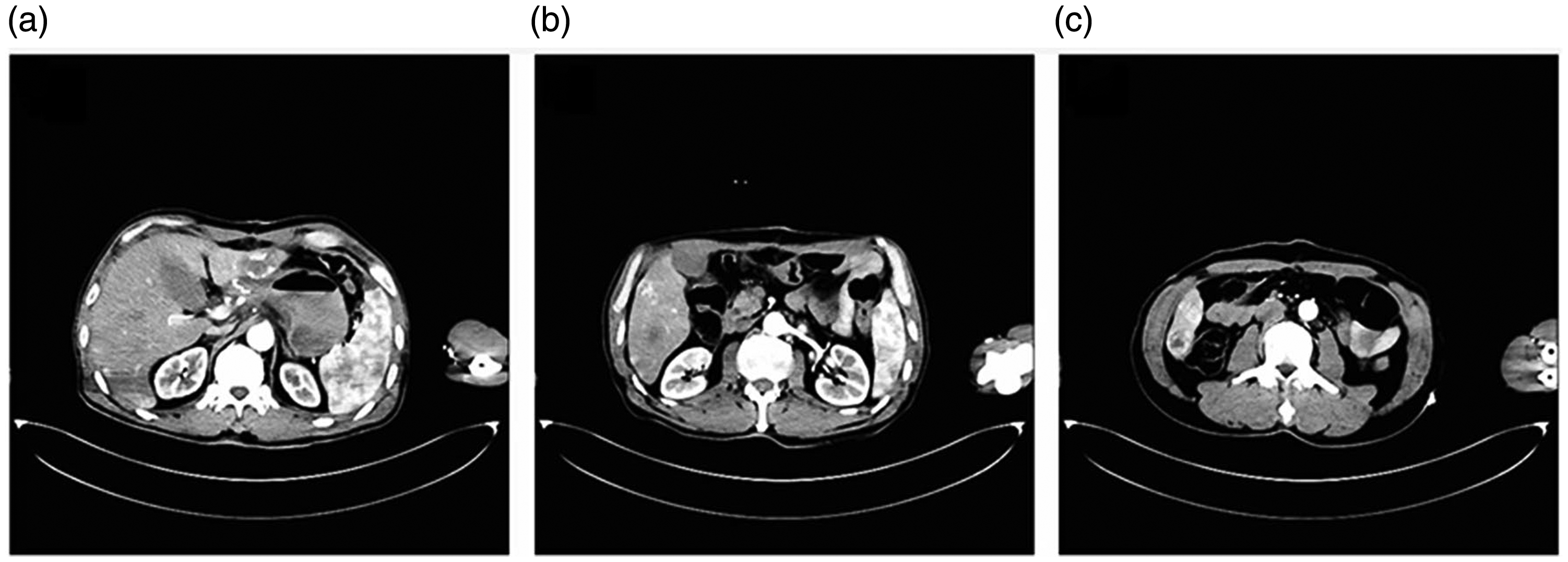
A 65-year-old male was referred to Qilu Hospital of Shandong University (Qingdao) in 2015 for definitive surgery for gastric adenocarcinoma. Three months earlier, he had suffered from epigastric discomfort and tarry stools with no obvious predisposing causes. However, he did not seek medical attention until several weeks before admission for a progressively aggravated condition. Endoscopic biopsy showed the presence of adenocarcinoma. A computerized axial tomography (CAT) scan revealed a cord-like opacity in the middle lobe of the right lung, and localized emphysema in the inferior lobe of the right lung; multiple hepatic cysts and a suspicious low density focus in segment VI (Figure 1); a thick gastric antrum wall; and a low attenuation nodular lesion in the sacrum. However, no lymph node metastasis or testicular abnormalities were observed.

A suspicious low density focus in segment VI (white arrow).
No notable medical history was identified, except for alcoholic hepatitis for more than 20 years which was untreated. His family history was also negative for familial or hereditary disease. On physical examination the patient was pale because of severe anemia, and slight abdominal tenderness on the right quadrant was detected. Neither gynecomastia nor testicular abnormalities were clinically noted. The rectal digital examination was normal, except for the presence of dark brown stools. Furthermore, hemoglobin levels were 40.0 g/L (normal range, 130–175 g/L) and albumin was 33.5 g/L (normal range, 35.0–55.0 g/L). The levels of other tumor markers were within normal ranges. The primary diagnosis was gastric carcinoma complicated by hemorrhage.
The patient’s anemia was corrected by the transfusion of 12 U of concentrated red blood cells, then radical subtotal gastrectomy with D2 lymph node dissection and Billroth I gastrojejunostomy were performed. Grossly, a 2.5 × 2.1 × 1.0 cm exophytic lesion was found in the antrum along the greater curvature. On the section surface, this was red and gray in color, indicating that it was a solid and soft tissue. Histological examination of the paraffin sections of the lesion revealed the involvement of all layers (T4a) of the gastric wall. However, metastases to the other tissues were not found, except for those to blood and lymph vessels. Both resected margins were free of tumors. The gastric tumor exhibited two main microscopic patterns. The poorly differentiated adenocarcinoma was contiguous to the choriocarcinoma component, with relatively well-defined edges (Figure 2). Furthermore, one of the 38 (N1) demonstrable perigastric lymph nodes exhibited metastasis through the tumor.

(a–c) Hematoxylin and eosin staining of the gastric biopsy showing a choriocarcinomatous component consisting of cytotrophoblastic and syncytiotrophoblastic cells with hemorrhagic lesions (magnification ×100).
Immunohistochemistry was positive for antibodies to p53, CK10, CKpan, CK7, Her-2, and a Ki-67 labelling index of 70%, which was strong but presented a focally positive reaction with placental alkaline phosphatase. A much stronger and diffuse staining of the specimen with human chorionic gonadotropin (hCG) was observed, and the adenocarcinoma component was stained with CK20, p53, CKpan, CK10, and a Ki-67 labelling index of 60%. These findings confirmed the presence of gastric choriocarcinoma admixed with adenocarcinoma (Figure 3).

Positive staining for an antibody to CK7 (a), which had a focally positive reaction with placental alkaline phosphatase (b). Strong and diffuse staining with an anti-hCG antibody (c).
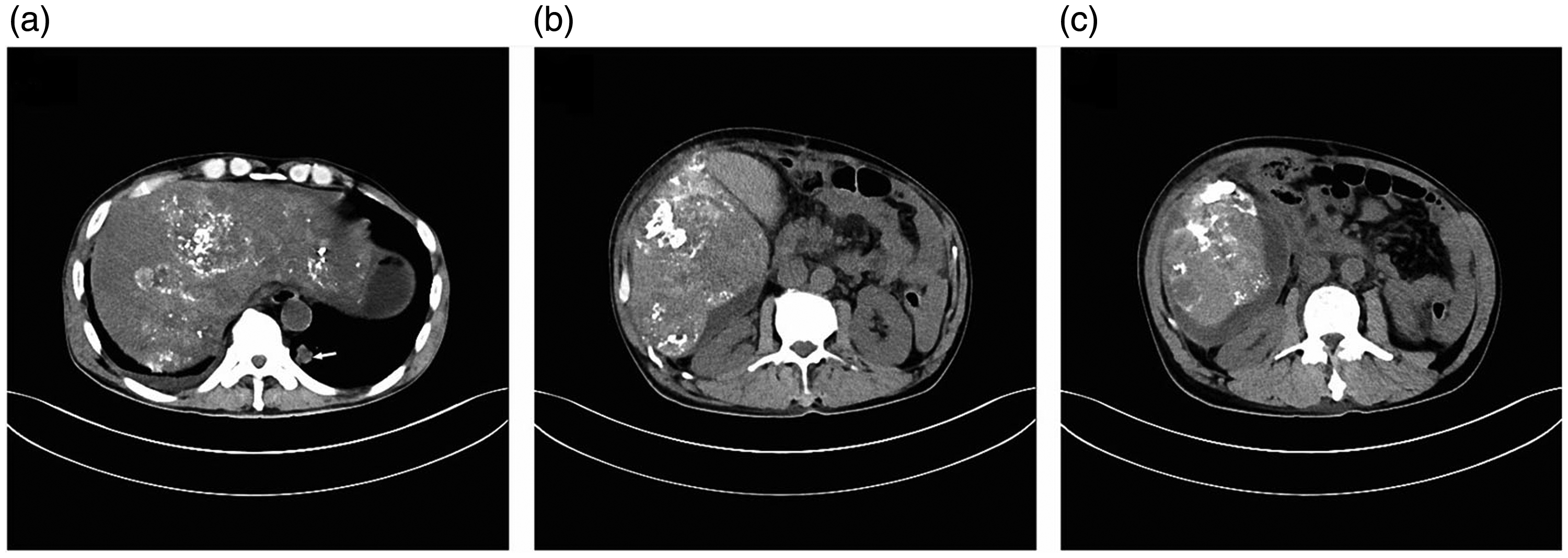
The β-hCG level was 215,297.0 mIU/mL, serum estradiol was 414 pg/dL, prolactin was 23.70 ng/mL, and follicle-stimulating hormone was 22.00 mIU/mL. The CAT scan revealed a 1.3-cm diameter nodule in the inferior lobe of the left lung and a small amount of pleural effusion on the left area, as well as multiple low density areas suggesting hepatic metastases (Figure 4). The patient was recommended to receive chemotherapy (5-Fu) after 1 week, and was then discharged.
(a–c) An abdominal computerized axial tomography scan of the arterial and portal venous phases showing multiple low density areas, suggestive of hepatic metastases.
After 10 days, the patient was re-admitted with complaints of sudden epigastric pain. Physical examination revealed tenderness and tension in the extensive abdominal region. The liver was palpable at five fingerbreadths below the costal margin. A CAT scan of the thorax and abdomen was immediately performed, revealing multiple lung and liver metastases, enlargement of the abdominal lymph nodes, and a patch-shaped high-density area in the right posterior lobe of the liver, suggestive of a bleeding site caused by the rupture of a subcapsular metastatic nodule (Figure 5). This was ultimately confirmed by angiography during transhepatic artery embolization. Lipiodol (20 mL) and gelfoam (510 mg) were administered after superselective catheterization of the bleeding branch artery of the right hepatic artery. The postoperative recovery was unremarkable. The patient declined further treatment, and was discharged on request on postoperative day 11. However, he had a rapid downhill course, and passed away 18 days after discharge from hemorrhagic shock. Written consent for publication of this study was obtained from the patient’s guardian, and the study was approved by the Ethics Committee of Qilu Hospital of Shandong University (Qingdao).
Thoracic and abdominal computerized axial tomography scans showing multiple hepatic metastases (a–c) and lung metastases indicated by a white arrow (a). A patch-shaped high-density area in the right posterior lobe of the liver suggested bleeding (b, c).
Discussion
No autopsy was performed in the present case, so it remains uncertain whether the patient’s choriocarcinoma developed locally or was a metastasis of the testicular tumor. 5 Hence, we mainly discuss the primary non-gestational, extragonadal gastric choriocarcinoma (PGC), which is notoriously difficult to diagnose. Furthermore, this is an extremely rare and highly malignant tumor from which most patients die within a year of diagnosis. 6
Several hypotheses have previously been proposed to explain the pathogenesis of PGC: an origin in an abdominally displaced gonadal anlage postulated by Davidson in 1905; the peculiar degenerative change of a gastric carcinoma by Risel in 1907; 7 dislocation of totipotential germ cells during the blastula or morula stage; and de-differentiation in hCG-producing cells of the normal gastric mucosa without a preceding adenocarcinoma. 7
Among these, the most widely accepted theory is retro-differentiation. Further support of this theory comes from the following: comparative genomic hybridization and fluorescence in situ hybridization applied in the study of primary gastric choriocarcinoma by Liu et al. 8 suggest that that the tumor genetically possesses the characteristics of both adenocarcinoma and choriocarcinoma; morphologically that there is a gradual transition from adenocarcinoma to choriocarcinoma; and epidemiologically that PGC possesses similar clinical characteristics to those of gastric adenocarcinoma in terms of mean age of onset, male-to-female ratio, and tumor location in Japan. 9 However, the distribution of β-hCG immunoreactive cells in the noncancerous gastric mucosa did not differ in terms of degree of reactivity or in the localization of positive cells, when compared with findings in typical adenocarcinomas. 10
Nevertheless, it remains difficult to obtain a definite preoperative diagnosis of PGC.11,12 Indeed, because of the coexistence of gastric choriocarcinoma and adenocarcinoma, this can be easily mistaken as adenocarcinoma by preoperative endoscopic biopsy, and only 8% of PGC cases have been correctly diagnosed.13,14 The diagnosis of gastric choriocarcinoma and its classification must first be based on histologic and immunohistochemical features, elevated serum β-hCG levels, and the absence of clinically apparent testicular abnormalities. Then, a diagnosis of PGC can be made. 15 It remains uncertain whether serum levels of β-hCG have prognostic significance, but the consecutive measurements of these levels may be useful in confirming and complementing the morphologic diagnosis, 15 following the response to treatment and tumor recurrence. 16
Gastric choriocarcinoma is a considerably malignant disease, with an average survival of only 2.5 months after admission for PGC patients. 17 Furthermore, no effective regimens have yet been established, and the therapeutic effects of chemotherapy and radiotherapy have been proven to be ineffective. For cases with hepatic metastasis, incontrollable hemorrhagic complications are the most common causes of death. Ligation of the hepatic artery or hepatic lobectomy, or angioembolization could be an effective approach to cease the bleeding as a potentially life-saving measure. 18
There were some limitations to the present study. First, there were no sufficient data on hematoxylin and eosin staining or immunohistochemistry images, the topographic distribution of adenocarcinoma and choriocarcinoma components, the intermingled immunohistochemical features of these components, and the histology of lymph node metastases. Second, there were no sufficient data on the microscopic morphology, necrosis, mitotic count, bleeding range and proportion of these two components. Finally, there were no sufficient data on computed tomography and immunohistochemistry for Ki-67, vascular density, and vascular invasion.
In conclusion, the present case could be a reference for researching the pathogenesis and treatment of gastric choriocarcinoma, particularly when it develops locally, with a view to improving its prognosis.