
Abstract
Background
To evaluate the clinical characteristics and indications for surgery for bezoar-induced small bowel obstruction (BI-SBO).
Methods
Forty patients with BI-SBO were treated at our hospital from January 2017 to December 2019, and these patients’ clinical and computed tomography (CT) data were analyzed.
Results
Twenty-seven and 13 BI-SBO patients constituted the non-ST group and ST group, respectively. The clinical manifestations of BI-SBO in both groups were abdominal pain, nausea, vomiting, and lack of defecation. Comparing the non-ST vs ST groups, respectively: mean age (years): 63.15 ± 16.15 vs 60.38 ± 12.47; duration of symptoms (hours): 55.11 ± 44.08 vs 59.33 ± 72.90; mean bezoar length (cm): 5.31 ± 0.74 vs 3.72 ± 0.53; mean bezoar width (cm): 3.74 ± 0.48 vs 2.9 ± 0.64; bezoar CT maximum Hounsfield units (HU): 97.23 ± 12.36 vs 21.11 ± 7.27; total hospital stay (days): 5.56 ± 4.23 vs 7.12 ± 6.12 (mean: 8.62 ± 2.81); and total hospitalization costs (RMB): 6378.02 ± 3015.68 vs 8213.71 ± 5564.29. Mean operation time was 85.00 ± 8.90 minutes, and mean operation blood loss was 32.31 ± 19.64 mL. Bezoars were located 60 to 160 cm from the ileocecal junction. Univariate analysis demonstrated that bezoar length and width and maximum CT value were significant risk factors for surgery.
Conclusion
Large bezoar size and high CT values may be indications for surgery. Surgery is necessary and effective when nonsurgical treatment is ineffective.
Keywords
Introduction
Small bowel obstruction (SBO) is a common clinical disorder caused by various conditions, such as adhesions, volvulus, intussusception, hernia, and tumors. SIBO occurs when the flow of intraluminal contents is disrupted, causing the proximal loops to dilate and the distal loops to decompress. 1 Rarely, bowel obstruction can be caused by a bezoar, or a mass of undigested foreign material. 2 Bezoars are gastrointestinal intraluminal stones, 3 and their formation is related to various factors, such as gastrointestinal motility disorders and gastrointestinal surgery for intestinal diverticula, surgical enteroanastomoses, blind pouches, afferent loops, and stenosing or strictures secondary to Crohn’s disease and intestinal tuberculosis. 4 Bezoars may be found anywhere in the gut but most reside in the stomach 5 and enter the small intestine via the pylorus. The incidence of bezoar-induced SBO (BI-SBO) is less than 1% in the general population.6,7 Several previous studies have described extremely rare SBO due to bezoar impaction.8–10 The associated clinical signs and symptoms of BI-SBO are vomiting, nausea, abdominal pain, fever, and elevated leukocyte count, which are not easily distinguished from other causes of SBO. Imaging examinations play an important role in the diagnosis of BI-SBO, especially computed tomography (CT). Abdominal CT can locate the position of the bezoar and determine the obstructive degree. Conservative treatment is the main therapy for BI-SBO; however, surgical procedures are useful for removing bezoars, and delayed surgery may increase the incidence of complications and mortality.11–13
In this study, we retrospectively analyzed patients with BI-SBO who were treated in our hospital. We aimed to identify the clinical characteristics of BI-SBO and the indications for surgery to enhance clinicians’ understanding of this disease.
Methods
This study was approved by the Ethics Committee for Human Research, The Fourth Affiliated Hospital, Zhejiang University School of Medicine. Written informed consent was obtained from the patients for the treatments that they received.
This was a retrospective study of the clinical characteristics and indications for surgery for BI-SBO. All patients were diagnosed with BI-SBO using CT, and we patients’ data were retrieved from our inpatient database. We reviewed the patients’ medical records and recorded their demographic data, clinical characteristics, and CT findings. The diagnosis of BI-SBO was made according to the clinical manifestations and CT findings, which showed the bezoar size and location. We divided the patients into two a non-surgery group (non-ST) and a surgery group (ST) and classified their symptoms according to the major clinical manifestations of abdominal pain, nausea and vomiting, and abdominal distention with lack of defecation. The duration of symptoms was defined as the time interval (hours) from disease onset to admission. Preoperative hospital stay was defined as the days between admission to the date of surgery. The size of the bezoar in the CT image was measured using imaging software (Laida Information Technology Co., LTD., Zhejiang, China), and the actual size of the bezoar in the ST group was measured using a gauge, postoperatively. The length of the bezoar in the CT image was defined as the maximum diameter in cross section, and the width was the minimum diameter of the same bezoar cross section. The bezoar CT value in Hounsfield units (HU) was measured as the maximum, average, and minimum values. The bezoar location in the ST group was defined as the distance from the bezoar to the ileocecal junction. SBO recurrence was defined as SBO relapse owing to another bezoar within 6 months after discharge.
Categorical variables in both groups were analyzed statistically using the χ2 test, and P values <0.05 were considered statistically significant. All analyses were performed using SPSS 19.0 (Armonk, NY, USA).
Results
From January 2017 to December 2019, 40 patients with BI-SBO were managed at our hospital and were included in this study; 27 and 13 patients constituted the non-ST and ST groups, respectively. The baseline demographic data for both groups are shown in Table 1. Eleven (27.5%) patients had a history of gastrointestinal surgery, such as subtotal gastrectomy, radical resection of gastric cancer, and partial enterectomy. The mean age in the non-ST group was 63.15 ± 16.15 years vs 60.38 ± 12.47 years in the ST group. The clinical manifestations of BI-SBO in both groups were abdominal pain, nausea, vomiting, and lack of defecation. The duration of symptoms in the non-ST group was 55.11 ± 44.08 hours, which was similar to that in the ST group at 59.33 ± 72.90 hours. The mean bezoar length in the ST group was 5.31 ± 0.74 cm vs 3.72 ± 0.53 cm in the non-ST group (P = 0.041). The mean bezoar width in the ST group was 3.74 ± 0.48 cm vs 2.9 ± 0.64 cm in the non-ST group (P = 0.017). Bezoars in the ST group had a higher maximum CT value compared with the non-ST group (97.23 ± 12.36 HU vs 21.11 ± 7.27 HU, respectively; P = 0.039). Five (12.5%) patients underwent ileal tube placement, and four (80%) were treated successfully. Bezoars presented as round or oval masses with well-coated envelopes located in the intestinal lumen with asymmetrical densities and mottled gas densities inside the cavity on CT. The bezoar CT values were asymmetrical, with higher values in the encapsulating wall and lower values inside the bezoars. The bezoar CT radiological appearances in partial BI-SBO cases is shown in Figure 1. Total hospital stay in the non-ST group was shorter than in the ST group (5.56 ± 4.23 days vs 7.12 ± 6.12 days, respectively; P = 0.402), and hospitalization costs in the non-ST group were lower than in the ST group (6378.02 ± 3015.68 RMB vs 8213.71 ± 5564.29 RMB, respectively; P = 0.674). Two patients in the non-ST group developed BI-SBO again within 6 months after discharge, compared with no patients in the ST group (P = 0.298).
Baseline demographic, clinical, and CT statistics for the non-ST and ST groups.

*Statistically significant: P < 0.05.
CT, computed tomography; GI, gastrointestinal; HU, Hounsfield units; RMB, renminbi.

Radiologic appearances of the bezoars in CT planar scans.
The 27 patients in the non-ST group passed the bezoars spontaneously after 2 to 6 days of conservative treatment. All 13 surgery cases underwent open surgery, which consisted of two main procedures: partial small bowel resection and intestinal incision. The mean operation time was 85.00 ± 8.90 minutes, with a mean operation blood loss of 32.31 ± 19.64 mL. The mean size of the bezoars found during surgery was 5.69 ± 0.63 cm in length and 4.15 ± 0.72 cm in width, and bezoars were located 60 to 160 cm from the ileocecal junction. All of the patients in the ST group underwent conservative treatment, namely drug therapy and ileal tube placement, prior to surgery. When these measures were ineffective, patients underwent surgery after a mean waiting time of 7.92 ± 10.23 days. The mean postoperative hospital stay was 8.62 ± 2.81 days (Table 2). All the operations and patients’ recoveries were uncomplicated other than incisional pain, which was relieved with pain medications. Univariate analysis demonstrated that bezoar length (P = 0.001, odds ratio (OR) = 35.866, 95% confidence interval (CI): 4.008–320.959) and width (P = 0.003, OR = 9.536, 95% CI: 2.195–41.433) and high CT value (P = 0.046, OR = 1.185, 95% CI: 1.003–1.401) were significant risk factors for surgery (Table 3).
Surgical data and bezoar characteristics in the 13 BI-SBO cases.

SD, standard deviation.
Estimated hazard ratios for surgery by univariate Cox regression analyses.
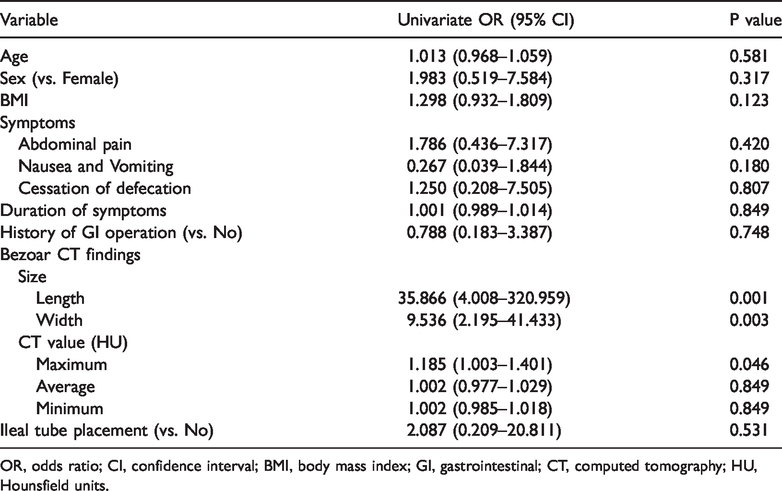
OR, odds ratio; CI, confidence interval; BMI, body mass index; GI, gastrointestinal; CT, computed tomography; HU, Hounsfield units.
Discussion
Despite BI-SBO being rare, this emergency abdomenal condition is encountered frequently worldwide, and accounts for approximately 4% of all SBO cases.14–16 Gastrointestinal surgery, such as gastroenterostomy, gastrojejunostomy, or pyloroplasty may expand the stomach outlet, which may result in undigested vegetable or fruit fiber masses easily entering the small intestine and forming masses in the small intestinal lumen, resulting in incarceration and obstruction. 17 The clinical manifestations are manifold, and the most common clinical manifestations of BI-SBO are abdominal pain, bloating, nausea, and vomiting or/and defecation cessation, manifesting as complete mechanical intestinal obstruction. In our study, patients were generally older, with defective dentition and a preference for vegetables, which contributed to the bezoar formation. Eleven patients had a history of gastrointestinal surgery, which carries a high risk for BI-SBO. The clinical manifestations in our cases were atypical compared with the literature, which influenced the diagnosis.
There currently is no specific modality for diagnosing a bezoar; however, imaging examination, especially CT, plays a significant role in the diagnosis of BI-SBO. Several imaging examinations, such as abdominal X-ray, barium enema, and endoscopy have been used to clarify a diagnosis of BI-SBO; however, these modalities exhibit poor diagnostic accuracy. CT is used most commonly and is useful in the diagnosis of BI-SBO. The bezoar locations and number, intestinal ischemia, strangulation, perforation, and other potential intestinal complications can be determined concurrently, using CT. Characteristically, with CT imaging, bezoars usually appear as round, oval, or tubular masses with clear boundaries, located within the intestinal lumen. Bezoars often display different densities with CT, with mottled gas densities inside the bezoar; other CT features varied in the literature. Kim et al. 18 suggested that an encapsulating wall could be seen in CT images, which was determined to be a gelatinous membrane on the bezoar surface that was formed by gastrointestinal mucosal secretions. All of the patients in our study underwent CT examination to clarify the diagnosis of BI-SBO, and the scans revealed that all of the bezoars were oval or round masses with clearly-enhanced encapsulating walls, similar to the description in previous reports. Furthermore, the enhanced wall of the bezoar commonly presented with high CT values, which indicated strong rigidity of the bezoar. The maximum CT values of the bezoars in our ST group were significantly higher than those in the non-ST group, indicating that more rigid bezoars were less likely to decompose and required surgery.
Previous studies reported that the bezoars contained calcium phosphate, bilirubin, and cholesterol, and the HU values on CT ranged from 31 to 134 HU. 19 Calcified and non-calcified bezoars have different reported CT values of 105 and 31 HU, respectively.20,21 In our study, the bezoar CT values differed widely. The mean maximum value was significantly lower in the non-ST group vs the ST group (P = 0.039), and univariate analysis demonstrated that high bezoar CT value was a significant risk factor for surgery. High values may indicate greater bezoar rigidity and less likelihood of being dissolved, resulting in complete incarceration in the intestinal lumen. Therefore, we surmised that high CT values in the bezoar encapsulating wall was a predictive factor for surgery. In addition, the mean bezoar size in the ST group evaluated in the CT image was significantly larger than in the non-ST group, in our study. Univariate analysis demonstrated that bezoar length and width were significant risk factors for surgery. Essentially, larger bezoars were also harder and more likely to migrate into the small intestine, incarcerate, and require surgery.
Bezoars usually become trapped in narrow sections of the small intestine, inducing SBO. The most common obstructed bezoar location is the distal ileum, 50 to 70 cm from the ileocecal valve because the lumen of this small intestinal segment is narrow. 22 In our cases, bezoars were found 60 to 160 cm from the ileocecal junction, which differed from the location in previous reports. In our opinion, the bezoar incarceration site depends on both bezoar size and intestinal luminal diameter.
Several non-surgical methods have been proposed for the treatment of bezoars, namely a liquid diet, oral sodium bicarbonate powder, enzymatic digestion with various agents, and endoscopic fragmentation. Zheng et al. 23 reported a successful case of “sandwich” treatment for diospyrobezoar intestinal obstruction. The reported success rate of endoscopic treatment for bezoars is high, ranging from 71.5% to 100%, in some studies.24,25 Because of this increased success rate, surgical treatment for bezoars decreased correspondingly. In our opinion, surgical intervention remains necessary in cases where there is a failure of nonsurgical treatment. Bedioui et al. performed a retrospective study evaluating 15 patients with BI-SBO; 12 patients underwent laparotomy and digital fragmentation of the bezoar. 17 We adopted a variety of treatments aimed at relieving the SBO, namely fasting, appropriate medications, and ileal tube placement, but outcomes of these treatments in the 13 cases in the ST group were unsatisfactory. These patients underwent surgery, and the bezoars were removed, which effectively restored the patency of the gastrointestinal tract.
There are two limitations in our study. The first is the potential for individual reporting bias, which may lead to under- or overestimation of the results. Another limitation is the small study size, which may have affected the incidence of BI-SBO and the surgery rate.
Conclusion
BI-SBO is relatively rare among SBO cases, and patients may exhibit different imaging characteristics than with other causes of SBO. Therefore, clinicians should understand the features of BI-SBO to determine whether to perform conservative treatment or surgery. CT is the main method of diagnosis. Large bezoar size and high CT values may be indications for surgery, and surgery may be necessary and effective, when nonsurgical treatment is ineffective. Further exploratory research is required to acquire more clinical experience with BI-SBO.
Footnotes
Acknowledgements
The authors gratefully acknowledge the assistance of our corresponding author (Dr Yulian Wu, MD, PhD) for her critical review of this manuscript. Furthermore, we are grateful to the members of the Department of General Surgery of our institution.
Authors’ contributions
WS acquired the data and drafted and revised the manuscript. WS, YXH, and ZYX were the treatment team members. WYL was responsible for the patients’ surgical management and revised the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.