
Abstract
Objective
To evaluate the impact of an enhanced recovery after surgery (ERAS) pathway on patients undergoing minimally invasive radical prostatectomy at a single institute.
Methods
In this retrospective study, 301 patients who underwent laparoscopic or robot-assisted laparoscopic radical prostatectomy from May 2014 to September 2018 were consecutively recruited. Before April 2017, the patients were treated with conventional care; all patients were treated with the ERAS pathway thereafter. The primary outcome was the postoperative length of hospital stay (LOS). The secondary outcomes were hospitalization costs and postoperative complications.
Results
In total, 138 patients were treated with the ERAS pathway, and the remaining patients underwent conventional care. The postoperative LOS was significantly shorter in the ERAS group than in the conventional group (median, 6 vs. 8 days). The hospitalization costs were also significantly lower in the ERAS group ($4086 vs. $5530). Ten (6.1%) patients in the ERAS group and 17 (12.3%) patients in the conventional group developed postoperative complications. The multivariable analysis showed that ERAS care was a significant independent predictive factor for a shortened LOS and reduced hospitalization costs.
Conclusions
The ERAS pathway was associated with a shortened LOS and reduced hospitalization costs for patients undergoing minimally invasive radical prostatectomy.
Keywords
Introduction
Prostate cancer is one of the most frequently occurring malignant tumors in men. 1 In recent decades, minimally invasive radical prostatectomy (MIRP), namely laparoscopic radical prostatectomy (LRP) and robot-assisted LRP (RALRP), has been widely performed and is now the gold standard treatment for local prostate cancer. 2
Enhanced recovery after surgery (ERAS) is a multimodal perioperative care program. 3 This approach includes several key elements that aim to reduce surgical stress and accelerate patient recovery. The ERAS concept was introduced in the 1990s in Europe. 4 Successful results were first obtained in colorectal surgery. 5 The ERAS pathway is now widely accepted by different surgical specialties and is recommended by clinical practice guidelines (www.erassociety.org). The key concepts of the ERAS pathway are avoidance of preoperative fasting and implementation of carbohydrate loading, multimodal analgesia, early oral feeding, and early ambulation.
Studies have shown that the ERAS pathway may lead to a significant reduction in the length of hospital stay (LOS) and the cost of hospitalization without increasing the surgical complication rate. A recent meta-analysis showed that ERAS pathways in major surgery reduced the LOS by 2.5 days and rate of complications by 30%. 6 Widespread protocols and outcomes for procedures such as radical cystectomy have recently been published. 7 The application of ERAS has shown promise in improving patient outcomes in selected minimally invasive surgeries. 8 However, many ERAS components are specific to abdominal surgery; their application in urological surgery, especially prostatectomy, is very limited. Whether the ERAS pathway can benefit patients with prostate cancer undergoing laparoscopic or robotic surgery remains inconclusive.
The objective of the present study was to compare the efficacy and safety of ERAS and conventional postoperative care in patients undergoing LRP or RALRP. Additionally, we evaluated whether ERAS care is an independent factor affecting the LOS and hospitalization cost.
Materials and methods
Patients and study design
We retrospectively analyzed consecutive patients who underwent LRP or RALRP at our institution from May 2014 to September 2018. The ERAS pathway was instituted on 1 April 2017. All urologists agreed to use the ERAS pathway for patients undergoing LRP or RALRP after this date. The relevant patient demographics and operative and pathological data were summarized. We compared the differences in the postoperative LOS, hospitalization cost, and postoperative complications before and after implementation of the ERAS pathway. Other indicators relevant to postoperative recovery were also compared. Univariate and multivariate regression analyses were used to evaluate the association of each factor with the LOS and overall hospitalization cost.
The principles of the conventional and ERAS pathways are shown in Table 1. The key principles of the ERAS pathway include preoperative nutrition, a shortened preoperative fasting time, selective bowel preparation, a minimally invasive surgical approach, and early postoperative mobilization.
Protocols of conventional and ERAS groups.

ERAS, enhanced recovery after surgery; POD, postoperative day.
Conventional pathway
All patients were instructed to fast for 12 hours before surgery. They underwent preoperative bowel preparation the night before surgery and the morning of the day of surgery (oral laxative and cleansing enema). Intraoperatively, all patients received liberal fluid therapy. LRP or RALRP was performed using the standard technique. Postoperatively, the patients started drinking water after anal exhaust and strictly did not restart solids until after defecation. The first ambulation was always carried out on postoperative day (POD) 5 or 6, and drainage tube removal occurred when the drainage volume was <10 mL for 3 consecutive days.
ERAS pathway
Preoperative patient education was a critical intervention. The other preoperative features were a short fasting time, selective bowel preparation, and normal oral nutrition until 10:00
This study was approved by the Institutional Review Board of Ruijin Hospital, Shanghai Jiao Tong University School of Medicine. Written informed consent was obtained from each participant.
Data collection and definitions
To evaluate the safety and efficacy of the ERAS protocol, our primary outcome was the postoperative LOS. The secondary outcomes were the total hospitalization cost and complication rate. The other observed indicators were the highest postoperative pain score, single drainage tube placement rate, drainage tube removal day, and catheter removal day. Postoperative functional recovery was assessed based on the time point at which independent activity was regained after surgery (defined as a Barthel score of >59). Additionally, we analyzed the factors associated with a prolonged LOS (defined as an LOS of >8 days, which was the median LOS in the conventional group) and high hospitalization cost (defined as $5530, which was the median cost in the conventional group).
The LOS was defined as the number of nights in the hospital postoperatively. The total cost for each patient included the costs of blood tests, imaging examinations, surgery, drugs, nursing, and others. The cost of the robotic platform was excluded from the analysis. The cost and LOS data for the patients in this study were obtained from the hospital administrative database. Pain was assessed using a 0- to 10-point verbal response scale, where “0” represents no pain and “10” represents the worst possible pain; the highest pain score was reported.
Statistical analysis
Non-normally distributed variables are reported as median with interquartile range and were evaluated with the Mann–Whitney U test. Categorical variables are reported as frequency and percentage and were evaluated with the chi-square test. Multivariate linear and logistic regression analyses were used to determine the factors that contributed to the highest postoperative pain score, a prolonged postoperative LOS, and high total costs. A two-sided P value of <0.05 was considered statistically significant. All analyses were performed using Stata® 15.1 Special Edition (StataCorp, College Station, TX, USA).
Results
In total, 301 patients who underwent LRP or RALRP were recruited in the present study. Among them, 138 patients were in the conventional group and 163 patients were in the ERAS group. The patients’ demographic characteristics are shown in Table 2. No significant differences were observed in age, body mass index, total prostate-specific antigen concentration, prostate volume, alcohol intake, smoking, history of abdominal surgery, lower urinary tract symptoms, androgen deprivation therapy, concomitant disease, Gleason score, or pathologic T stage between the two groups.
Characteristics of patients in conventional and ERAS groups.

Data are presented as median (interquartile range) or n (%).
ERAS, enhanced recovery after surgery; BMI, body mass index; tPSA, total prostate-specific antigen; LUTS, lower urinary tract symptoms; ADT, androgen deprivation therapy; LND, lymph node dissection.
*Concomitant disease included hypertension, diabetes mellitus, and coronary atherosclerotic cardiopathy.
As shown in Table 3, the postoperative LOS was significantly shorter in the ERAS group than in the conventional group (median, 6 vs. 8 days, respectively; P < 0.001). Furthermore, there was a significant difference in hospitalization costs between the two groups ($5530 in the conventional group vs. $4086 in the ERAS group, P < 0.001), representing a 26% difference. Interestingly, the highest postoperative pain scores were significantly higher in the ERAS group than in the conventional group (P = 0.001). However, after adjusting for covariables, the association between ERAS and pain scores was not significant (Table 4). The percentage of a single drainage tube in the conventional group was significantly lower than that in the ERAS group (54.3% vs. 88.3%, respectively; P < 0.001). The mean duration until drainage tube removal was significantly shorter in the ERAS group than in the conventional group (4 vs. 7 days, respectively; P < 0.001). The median duration until catheter removal in the conventional group was also significantly longer than that in the ERAS group (P < 0.001). There was a significant difference in the number of days needed to achieve independent activity after surgery between the two groups (5 days in the conventional group vs. 4 days in the ERAS group, P < 0.001).
Comparison of postoperative parameters in conventional and ERAS groups.

Data are presented as n, n (%), or median (interquartile range).
ERAS, enhanced recovery after surgery; LOS, length of hospital stay.
*Independent activity was defined as a Barthel score of >59.
Multivariable linear regression between several factors and highest postoperative pain score.
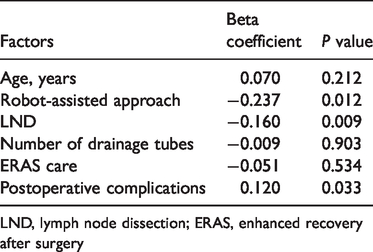
LND, lymph node dissection; ERAS, enhanced recovery after surgery
Univariate and multivariate analyses were performed to determine the factors that impact postoperative LOS and hospitalization costs. In the univariate analysis, the predictors related to a prolonged LOS were the prostate volume, lymph node dissection (LND), a robot-assisted approach, postoperative complications, and a non-ERAS pathway. Furthermore, in the multivariate analysis, LND [odds ratio (OR), 2.569; 95% confidence interval (CI), 1.224–5.394; P = 0.013)], a robot-assisted approach (OR, 8.884; 95% CI, 3.219–24.521; P < 0.001), postoperative complications (OR, 33.473; 95% CI, 9.274–120.817; P < 0.001), and a non-ERAS pathway (OR, 0.285; 95% CI, 0.086–0.945; P = 0.040) were still significantly associated with a prolonged postoperative LOS. The application of ERAS was independently protective against a prolonged LOS, decreasing that risk by 71.5% (Table 5). Similarly, the multivariate analysis showed that LND (OR, 2.525; 95% CI, 1.103–5.782; P = 0.028), a robot-assisted approach (OR, 14.524; 95% CI, 4.963–42.508; P < 0.001), and postoperative complications (OR, 4.993; 95% CI, 1.345–18.533; P = 0.016) were significantly associated with excessive hospitalization costs (Table 6). However, the use of an ERAS pathway remained protective against high hospitalization costs, decreasing the risk by 80.1% (OR, 0.199; 95% CI, 0.051–0.778; P = 0.020).
Univariate and multivariate logistic regression analysis of factors associated with a prolonged LOS.*

LOS, length of hospital stay; OR, odds ratio; CI, confidence interval; NA, not applicable; BMI, body mass index; tPSA, total prostate-specific antigen; LUTS, lower urinary tract symptoms; ADT, androgen deprivation therapy; LND, lymph node dissection; ERAS, enhanced recovery after surgery.
*Prolonged LOS was defined as >8 days (median LOS in the conventional group).
Univariate and multivariate logistic regression analysis of factors associated with high hospitalization cost.*

OR, odds ratio; CI, confidence interval; NA, not applicable; BMI, body mass index; tPSA, total prostate-specific antigen; LUTS, lower urinary tract symptoms; ADT, androgen deprivation therapy; LND, lymph node dissection; ERAS, enhanced recovery after surgery.
*High hospitalization cost was defined as >$5530 (median cost in the conventional group).
The complications that occurred during the hospitalization period are presented in Table 7. There were 17 (12.3%) complications in the conventional group and 10 (6.1%) in the ERAS group. There was no significant difference in the complication rates between the two groups. In the ERAS group, one patient developed intestinal obstruction, four developed hematuria, four developed persistent fever, and one developed urine leakage during the hospitalization period, and none of these patients required readmission or reoperation. In the conventional group, one, two, six, and four patients developed intestinal obstruction, hematuria, persistent fever, and urine leakage, respectively, and four patients developed other complications (urethral strictures, drainage tube fractures, hyponatremia, and insanity). One patient with urethral strictures was successfully treated by urethral dilatation, and the patient with a drainage tube fracture underwent a reoperation. All other patients with complications in the conventional group were treated conservatively. No mortality was observed in either group.
Incidence of overall and separate postoperative complications in conventional and ERAS groups.
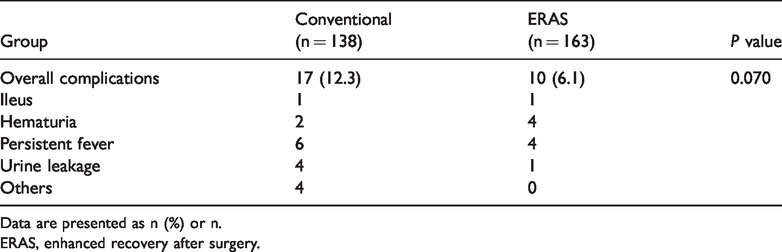
Data are presented as n (%) or n.
ERAS, enhanced recovery after surgery.
Discussion
Previous studies have demonstrated the advantages of ERAS pathways in laparoscopic or open colorectal surgery.9,10 However, the efficiency and safety of ERAS in prostatectomy still lacks definitive data, especially in minimally invasive surgery. This novel analysis evaluated the outcomes of the ERAS pathway applied to LRP and RALRP. Our study showed a significant reduction in the postoperative LOS and a median cost savings of approximately 26.1% in the ERAS group. Importantly, the perioperative complication rates were also lower in the ERAS than conventional group, although the differences were not statistically significant. Not surprisingly, after the univariate and multivariate logistic regression analysis, the non-ERAS pathway was confirmed as an independent factor associated with a prolonged LOS and excessive hospitalization costs. To the best of our knowledge, this is the largest study to analyze the safety and efficacy of the ERAS pathway in patients undergoing minimally invasive prostatectomy.
Our research was partly motivated by the quality goal of the medical center to discharge patients by noon. The ERAS pathway outlined in this report can be divided into three components: preoperative, intraoperative, and postoperative measures. Preoperative communication empowers patients to become active participants in their course of treatment. We utilized carbohydrate loading and a short duration of fasting before surgery to avoid perioperative insulin resistance as well as postoperative nausea or vomiting.11,12 Moreover, we believe that simple bowel preparation contributes to intestinal function recovery. 13 Our ERAS pathway has several notable intraoperative features: preheating the intravenous transfusion fluids and providing a hot blanket may help reduce the risk of incision wound infection or hemorrhage. 14 It seems that minimally invasive surgery (we applied distal urethral-sparing technology) can protect more functional tissue than open radical prostatectomy, though this is still under debate. 15 In our series, a single drainage tube was used for 88.3% of the patients in the ERAS group compared with only 54.3% in the conventional group. Many scholars have emphasized that drainage tubes may increase the rate of infections and the incidence of fistulas rather than reduce the postoperative complication rate. 11 Another novel feature of pain management was the use of the elastomeric analgesia pump, which aims to control postoperative pain and seems to decrease surgical trauma and facilitate early mobilization. 16 In our series, early mobilization strategies included keeping the head of the bed at 30° at all times, sitting up in bed on POD 0, getting out of bed and walking on POD 1, and encouraging ambulation as soon as possible. An oral diet was recovered as tolerated in the ERAS group, whereas the patients could drink water after anal exhaust and intake solids after defecation in the conventional group. Our results suggest that early oral feeding and mobilization are feasible and do not increase the incidence of cystourethral anastomosis leakage or hematuria. Early removal of unnecessary drainage tubes seems to facilitate early mobilization, 17 which may lead to more rapid return to independent activity (defined as a Barthel score of >59). As an important item in the ERAS pathway is perioperative goal-directed fluid management, which limits visceral edema and may avoid severe postoperative complications such as nausea, pulmonary edema, and vomiting. 18 ERAS care is a multidisciplinary and multimodal pathway. Based on our experience, the key elements of ERAS should include an anesthesia plan for pain and fluid management. 19
We explored the factors significantly affecting postoperative LOS and overall hospitalization costs, two of our primary outcomes. We confirmed that ERAS is an independent impact factor by the univariate and multivariate analyses. Delayed discharge was defined as a prolonged LOS beyond the median number of days in the conventional group (≥8 days), and excessive costs were defined as those beyond the median cost in the conventional group (>$5530). After balancing all covariates, our results suggest that implementation of the ERAS pathway reduced the postoperative LOS by 26.3% and decreased the risk of high costs by 80.1%. Our results are consistent with other similar studies. Gralla et al. 20 reported that the ERAS protocol led to a shorter LOS and fewer postoperative complications than the conventional protocol in LRP. Huang et al. 21 demonstrated that fast-track surgery was feasible and safe for Chinese patients undergoing RALP because patients treated by ERAS had significantly earlier flatus, a shorter period until resuming a regular diet, a shorter postoperative LOS, and a lower incidence of complications than those treated by conventional care. Summarizing the overall impact of ERAS implementation, a meta-analysis in urological surgery indicated that the ERAS pathway seems clinically effective and cost-effective. 19 To our knowledge, most publications to date support the use of the ERAS pathway, and very few reports have described a different point of view.
The current study suggested the safety of the ERAS pathway, and there was no significant difference in overall complications between the two groups. Complications were more common in the conventional group than in the ERAS group. Minimally invasive surgery may play a role in the lower incidence of complications with ERAS, 22 and the combined use of laparoscopy and the ERAS protocol has positive effects on surgical outcomes. 23 A randomized controlled trial compared open and minimally invasive approaches with and without ERAS management and concluded that a combination of the laparoscopic approach and ERAS led to a significant reduction in LOS and overall complications. 24 Certainly, goal-directed fluid management and early oral feeding can also be considered equally important. 11 Articles comparing open and minimally invasive approaches in gynecologic, esophageal, and gastric surgery also presented optimized outcomes with the use of ERAS.25–27
This retrospective study is limited by inherent selection and information biases. We attempted to balance these biases by including all consecutive LRPs and RALRPs performed during the study period and by performing a multivariate analysis, which confirmed that the ERAS protocol was an independent factor. Another limitation of our study is the small number of patients from a single institution. Whether our results can be appropriately applied to worldwide populations remains unclear. Furthermore, we only compared the total costs during hospitalization rather than analyzing costs by category. We recommend further research to identify crucial elements of the protocol. Despite these limitations, this study’s conclusion is convincing because we explored the difference between two groups and confirmed the protocol’s influence after balancing the other covariates.
Conclusions
Our results are important and summarized the efficiency and safety of ERAS pathways in patients with prostate cancer undergoing MIRP. Compared with the conservative approach, ERAS implementation was associated with more rapid discharge and lower hospitalization costs without increasing the incidence of complications. The ERAS pathway might provide a practical approach to optimize postoperative outcomes.
Footnotes
Acknowledgements
We thank all of the patients included in this study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by a grant from the Medical Guidance Science and Technology Support Project (Grant No. 18411960100) to Danfeng Xu.