
Abstract
Objective
We compared the diagnostic values of mammography and magnetic resonance imaging (MRI) for evaluating breast masses.
Methods
We retrospectively analyzed mammography, MRI, and histopathological data for 377 patients with breast masses on mammography, including 73 benign and 304 malignant masses.
Results
The sensitivities and negative predictive values (NPVs) were significantly higher for MRI compared with mammography for detecting breast cancer (98.4% vs. 89.8% and 87.8% vs. 46.6%, respectively). The specificity and positive predictive values (PPV) were similar for both techniques. Compared with mammography alone, mammography plus MRI improved the specificity (67.1% vs. 37.0%) and PPV (91.8% vs. 85.6%), but there was no significant difference in sensitivity or NPV. Compared with MRI alone, the combination significantly improved the specificity (67.1% vs. 49.3%), but the sensitivity (88.5% vs. 98.4%) and NPV (58.3% vs. 87.8%) were reduced, and the PPV was similar in both groups. There was no significant difference between mammography and MRI in terms of sensitivity or specificity among 81 patients with breast masses with calcification.
Conclusion
Breast MRI improved the sensitivity and NPV for breast cancer detection. Combining MRI and mammography improved the specificity and PPV, but MRI offered no advantage in patients with breast masses with calcification.
Keywords
Introduction
The International Agency for Research on Cancer estimated that there were nearly 2.09 million new cases of breast cancer in women worldwide in 2018, accounting for 24% of all new malignant tumors in women. Nearly 630,000 women died of breast cancer, representing 15% of all cancer-related deaths in women. Breast cancer has the highest rates of both morbidity and mortality among cancers in women. 1 The China National Cancer Center reported 300,000 new cases of female breast cancer in China in 2015. It was the most common malignant tumor in women in China, accounting for 17% of all new malignant tumors, with 70,000 breast cancer-related deaths in the same year, representing 8% (ranked 5th) of all cancer-related deaths in women. 2 Mammography and magnetic resonance imaging (MRI) are currently the conventional clinical methods for screening and diagnostic purposes. 3 However, although a recent study analyzed the diagnostic values of ultrasound and MRI in breast cancer masses, 4 comparisons of mammography and MRI for diagnosing breast cancer are lacking. Breast masses are a common symptom of breast cancer, and we therefore focused on patients with mass-type breast disease. In this study, we compared the performances of mammography and MRI for diagnosing breast cancer by retrospectively analyzing data pertaining to 377 patients with breast lumps.
Materials and methods
Patients and data
This study was approved by the ethics committee of the First Affiliated Hospital of Chongqing Medical University. All processes implemented in the study were in keeping with the institutional and national research committee’s ethical standards and with the 1964 Helsinki Declaration. This was a retrospective study with no risk to the patients, and the patients’ safety and privacy were protected. The patients provided consent for use of their data.
Mammography, MRI, and pathological data were collected for inpatients at our hospital with breast lumps detected by physical examination or screening tests and confirmed by mammography between January 2016 and December 2018. This was a retrospective study and patients were required to meet the following inclusion criteria: 1) female; 2) no history of breast disease or surgery; 3) undergone mammography and MRI within 1 month before operation (excluding puncture) in our hospital; and 4) confirmed pathological diagnosis. The exclusion criteria were: 1) metastatic breast tumors; 2) simple axillary mass; 3) Breast Image-Reporting and Data System (BI-RADS) 1 under mammography; 4) incomplete data; and 5) simple calcification detected by mammography.
Imaging examination
All patients underwent mammography using a Siemens Mammomat Inspiration digital mammography machine (Wittelsbacherplatz 2, DE-80333; Siemens AG, München, Germany). Both craniocaudal and mediolateral-oblique views were obtained. MRI was carried out using a GE Signa HD × 3T magnetic resonance scanner and 8-channel phased array surface coil (General Electric Company, Waukesha, WI, USA). The patients were placed in a prone position allowing natural overhang of both two breasts, with the nipples aligned to the center of the coil. There was no need for breast compression. The patients were instructed to breathe as calmly as possible.
Dynamic contrast-enhanced MRI was carried out by 3D-breast volumetric imaging sequence T1WI fat suppression scan (TR = 4.5 ms; TE = 2.2 ms; TI = 14 ms; acquisition matrix: 416 × 320; thickness = 1.2 mm; spacing = 0 mm; NEX = 0.71; field of view 34 cm×34 cm). The contrast agent gadolinium diethylenetriamine pentaacetic acid (20 mL) was injected into the median cubital vein using a pressure syringe at a flow rate of 2.0 mL/s, followed by 20 mL normal saline flush at 2 mL/s. One phase of plain scanning was carried out before enhancement, followed by starting scanning 5 s after injection of the contrast agent, and nine further phases of continuous scanning, with a single scanning time of 58 to 75 s. The largest level of the lesion was used as the region of interest, and grossly identifiable bleeding, liquefaction necrosis, cystic degeneration, and blood vessels were avoided. The time-intensity curve (TIC) was generated automatically by the Functool software in the GE ADW4.4 workstation (General Electric Company). We divided the curves into three types according to the Kuh1 classification 5 : type I (continuously rising; continuous strengthening, 2–7-minute signal intensity increases >10%); type II (rising platform; after early increase, signal strength maintained at a plateau level in the middle and late stages of enhancement, signal strength increases or decreases between ±10% from 2–7 minutes); and type III (fast-in and fast-out; after early enhancement, signal intensity decreased in the middle and late stages of the enhanced scan, signal intensity decreased by >10% in 2–7 minutes).
The images were interpreted by two senior breast imaging diagnostic physicians, at intermediate and senior professional levels. The results of mammography and MRI were classified and evaluated using the BI-RADS classification system, version 5. 6
Pathological examination
All patients underwent core needle biopsy and the excised specimens were fixed with 4% neutral formaldehyde, soaked in paraffin, and thin tissue sections were cut and stained with hematoxylin–eosin. The pathological results were considered as the diagnostic gold standard for this study.
Statistical analysis
Statistical analysis was carried out using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA). Categorical variables were expressed as percentages, and intergroup differences were assessed using χ2 or Fisher’s exact tests. The diagnostic values of mammography, MRI, and combined mammography and MRI were assessed based on receiver operating characteristic (ROC) curve analysis. A value of P < 0.05 was considered significant.
Results
Clinical features of all patients based on mammography
Based on the inclusion criteria, we collected data for 591 cases, of which 214 were excluded based on the following exclusion criteria: metastatic breast tumors (n = 15), simple axillary mass (n = 4), patients with BI-RADS 1 under mammography (n = 120), patients with incomplete data (n = 23), and simple calcification detected by mammography (n = 52). A total of 377 patients were therefore included in the analysis, including 73 patients with benign and 304 with malignant breast tumors (Table 1). Only 15 patients (15/73, 20.5%) with benign tumors and 66 (66/304, 21.7%) patients with malignant tumors showed masses with calcification. The mammography results were classified into seven categories from 0 to 6 according to the American College of Radiology BI-RADS. 6 The proportion of malignant lesions gradually increased with increasing category, with most malignant tumors in categories 4 and 5 and most benign lesions in categories 3 and 4 (P < 0.001) (Table 1).
Clinical features of all patients based on mammography.

BI-RADS, Breast Image-Reporting and Data System.
Patterns of masses with calcification
Calcifications occurred inside or outside the breast masses in some patients, and some calcification patterns were more common in malignant tumors. Forty-four (44/66, 66.7%) malignant tumors showed round calcifications, nine (9/66, 13.6%) showed large rod-like calcifications, six (6/66, 9.1%) showed amorphous calcifications, five (5/66, 7.6%) showed fine pleomorphic calcifications, and two (2/66, 3.0%) showed coarse heterogeneous calcifications (Table 2).
Patterns of masses with calcification (n = 81).

TIC
The TIC identifies powerful risk-indicators of malignant breast tumors. The TIC for MRI reflects the dynamic characteristics of lesions. 5 In this study, 23 (33/58, 39.7%) benign lesions were type I (ascending), 18 (18/58, 31.0%) were type II (plateau), and 17 (17/58, 29.3%) were type III (outflow). Among the malignant lesions, 4 (4/281, 1.4%) were type I, 52 (52/281, 18.5%) were type II (plateau), and 225 (255/281, 80.1%) were type III (outflow) (P < 0.001) (Table 3).
Time-intensity curves in patients with benign and malignant tumors.

TIC, time-intensity curve.
Diagnostic values of mammography, MRI, and combined mammography and MRI
Out of the 377 patients, 73 had benign breast tumors and 304 had malignant breast tumors. We compared the diagnostic values of mammography and MRI for identifying categories 4 and 5 (BI-RADS 4 and 5) breast cancer lesions (clinically defined as malignant in this study), and lesions that were identified as category 4 or 5 by both mammography and MRI were considered as malignant based on joint use of MRI and mammography. The pathology results served as the gold standard. The performances of mammography, MRI, and combined mammography and MRI for detecting breast cancer were compared in terms of sensitivity, specificity, PPV, and NPV (Table 4).
Diagnostic value of mammography magnetic resonance imaging, alone or combined.
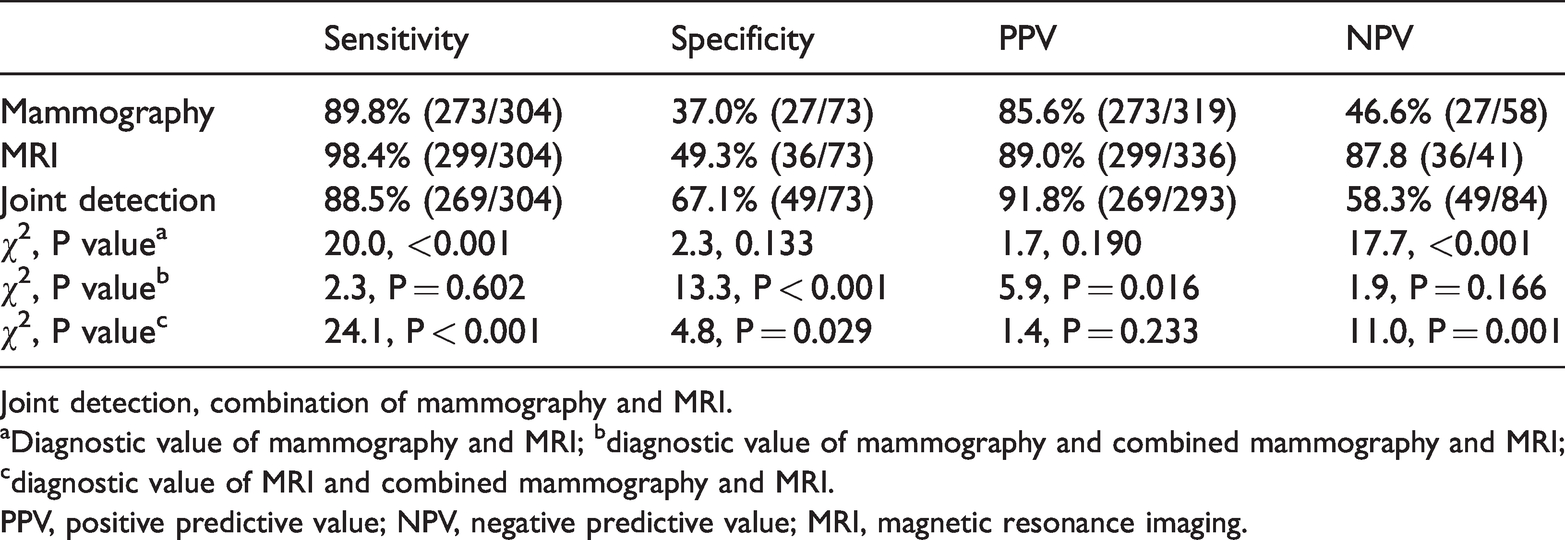
Joint detection, combination of mammography and MRI.
aDiagnostic value of mammography and MRI; bdiagnostic value of mammography and combined mammography and MRI; cdiagnostic value of MRI and combined mammography and MRI.
PPV, positive predictive value; NPV, negative predictive value; MRI, magnetic resonance imaging.
Diagnostic values of mammography and MRI
The sensitivity of mammography for detecting breast cancer was lower than that of MRI (89.8% (273/304) vs. 98.4% (299/304), χ2 = 20.0, P < 0.001) and its specificity was similar to that of MRI (37.0% (27/73) vs. 49.3% (36/73), χ2 = 2.3). The NPV of MRI was significantly higher than that of mammography (87.8% (36/41) vs. 46.6% (27/58), χ2 = 17.7, P < 0.001), while the PPVs of mammography and MRI were similar (85.6% (273/319) vs. 89.0% (299/336), χ2 = 1.7) (Table 4).
Diagnostic values of mammography with and without MRI
Compared with mammography alone, the joint use of mammography and MRI improved the specificity (67.1% (49/73) vs. 37.0% (27/73), χ2 = 13.3, P < 0.001) and PPV (91.8% (269/293) vs. 85.6% (273/319), χ2 = 5.9, P = 0.016), but the sensitivity and NPV were not significantly different (Table 4).
Diagnostic values of MRI with and without mammography
Compared with MRI alone, joint use of mammography and MRI reduced the sensitivity (88.5% (269/304) vs. 98.4% (299/304), χ2 = 24.1, P < 0.001) and NPV (58.3% (49/84) vs. 87.8% (36/41), χ2 = 11.0, P = 0.001), and increased the specificity (67.1% (48/73) vs. 49.3% (36/73), χ2 = 4.8, P = 0.029); however, there was no significant difference in terms of PPV (Table 4). The ROC curves for mammography, MRI, and joint use of these two methods are shown in Figure 1. The areas under the curves were 0.634, 0.738, and 0,776, respectively (P < 0.001).

Receiver operating characteristic curves for mammography, magnetic resonance imaging (MRI), and joint use of these two methods. (a) Mammography; (b) MRI; (c) combined use of mammography and MRI.
Diagnostic value of mammography and MRI for calcified lesions
Eighty-one patients showed calcified masses on mammography. The diagnostic sensitivities of mammography and MRI for calcified masses were 97.0% (64/66) and 100.0% (66/66) and the specificities were 33.3% (5/15) and 60.0% (9/15), respectively (Table 5). There was no significant difference in sensitivity or specificity between these two methods.
Diagnostic performance of mammography and magnetic resonance imaging for calcified lesions (n = 81).

PPV, positive predictive value; NPV, negative predictive value; MRI, magnetic resonance imaging.
Discussion
This study compared the diagnostic values of mammography, MRI, and the combined modality in 377 patients with breast masses. MRI showed greater sensitivity and NPV for breast cancer compared with mammography, while joint detection improved the specificity and PPV compared with mammography alone, and improved the specificity but reduced the sensitivity and NPV compared with MRI alone. There was no significant difference in sensitivity or specificity between mammography and MRI alone in 81 patients with calcified breast masses.
The initial clinical symptoms of breast cancer are not obvious, and most patients visit a doctor after finding a breast mass. 7 Mammography and MRI are currently the main diagnostic methods for breast disease and are widely used in clinical practice. Kaiser and Zeitler reported the first case of breast cancer detected by enhanced MRI in 19898,9 and since that time, several studies have investigated the application of MRI, which is currently recognized as the most sensitive method for detecting breast cancer.10–13 Compared with traditional mammography, MRI is playing an increasingly important role in breast screening. 14 However, studies evaluating the diagnostic roles of mammography and MRI for breast masses are lacking. Clinicians tend to use MRI, irrespective of the nature of the breast lesion as a mass or calcification, even though MRI has some disadvantages, including its unsuitability in patients with ferromagnetic implants or claustrophobia. 15 The current study included 377 patients with breast masses with or without calcification, and the results showed that MRI improved the diagnosis of breast cancer compared with mammography. Notably however, MRI did not improve the sensitivity or specificity in patients with breast masses with calcification. Patients should thus have the option to choose whether or not to undergo both MRI and mammography, given that rejecting MRI could reduce the financial burden on patients, save medical resources, and improve the efficiency of diagnosis and treatment.
A previous retrospective analysis of 172 patients 16 found that the sensitivity of combined MRI and mammography was 97.8%, compared with 78.3% for mammography alone. Kriege et al. 17 compared the diagnostic values of mammography and MRI in 1909 normal subjects and found sensitivities of 33.3% and 79.5% and specificities of 95.0% and 89.8%, respectively (P < 0.05). In general, the sensitivity of MRI for detecting breast cancer was higher than that of mammography. This finding is consistent with that of the present study. Researchers 18 conducted immediate MRI in 2021 breast patients with newly diagnosed cancer based on pathological examination and identified 285 new cancerous lesions that were missed by mammography. Constance et al. 12 also reported similar findings. Similarly, in the current study, 32 new cases were detected as benign lesions by mammography but as malignant lesions by MRI, and the final pathological diagnoses confirmed malignant breast tumors. Compared with mammography, breast MRI is thus more likely to discover breast lesions at an early stage.
Although breast MRI offers a prominent advantage in terms of detecting breast cancer,10,19–21 its specificity is similar to or even poorer than mammography.22,23 A prior study 15 found that breast MRI may lead to missed and/or misdiagnoses. Comparing MRI before and after obtaining pathological diagnoses of 58 breast tumors, six patients were missed by the initial MRI and 15 patients were misdiagnosed. In addition, MRI has demonstrated false positive rates of 37% to 100%.9,24,25 MRI is much more expensive than mammography, and cannot be used in people with metal implants.19,23,26–28 Discretion should thus be applied before recommending MRI, and it should not be used as a routine screening imaging modality. 29 Furthermore, MRI did not increase the diagnostic sensitivity or specificity for breast masses with calcification detected by mammography in the present study.
Three types of TICs 30 are distinguished based on signal changes in the breast lesions during dynamic enhancement MRI. Lesions with type I TIC are considered benign, while type II or III TIC lesions are considered as suspicious malignant lesions. 30 TIC type was significantly associated with the nature of the lesion (benign or malignant) (P < 0.05). Most malignant breast tumors in the current study were type III, which was consistent with previous studies. 19 This feature could thus be used for preliminary prediction of breast lesions.
This study has some limitations. This was a retrospective study, and therefore, the images were interpreted by different physicians with different habits and levels of experience. In addition, this was a single-institution study and the sample size was relatively small, especially in terms of patients with calcified masses.
Conclusions
In general, MRI can improve the diagnosis of breast cancer compared with mammography, and has been widely used in clinical settings. However, MRI did not improve the diagnostic sensitivity or specificity in patients with breast masses with calcification compared with mammography, and MRI should thus not be routinely recommended for these patients.
Footnotes
Acknowledgments
We thank all of the patients who participated in this study. We greatly appreciate the excellent assistance of Zubin Ouyang at the Department of Radiology. We also appreciate Medjaden Bioscience Limited for English language review.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.