
Abstract
Introduction
Data regarding the role of dual antiplatelet therapy in patients with ischemic stroke or transient ischemic attack are limited. This study aimed to systematically review and analyze the efficacy and safety of dual antiplatelet therapy compared with aspirin alone in patients with acute ischemic stroke or transient ischemic attack.
Methods
We searched PubMed, Embase, Scopus, Cochrane, and Web of Science databases from inception to August 2024 and identified randomized controlled trials comparing dual antiplatelet therapy with aspirin alone in patients with stroke. Pooled risk ratios with 95% confidence interval were calculated. Trial sequential analysis was conducted for the main outcomes to weigh the risks of type I and type II errors.
Results
Five studies involving 27,563 patients were included. Dual antiplatelet therapy was associated with a significantly reduced risk of recurrent ischemic stroke (risk ratio: 0.74, 95% confidence interval: 0.68–0.81) and major adverse cardiovascular events (risk ratio: 0.77, 95% confidence interval: 0.71–0.84). However, it was associated with a significantly higher risk of recurrent hemorrhagic stroke (risk ratio: 2.13, 95% confidence interval: 1.09–4.17) and bleeding (risk ratio: 2.21, 95% confidence interval: 1.48–3.32). Trial sequential analysis revealed that sufficient evidence for recurrent ischemic stroke, major adverse cardiovascular events, and bleeding was achieved.
Conclusion
Dual antiplatelet therapy demonstrated a lower incidence of recurrent ischemic stroke and major adverse cardiovascular events compared with aspirin alone. However, further studies are warranted to provide sufficient evidence regarding recurrent hemorrhagic stroke and all-cause mortality.
Keywords
Introduction
Ischemic stroke and transient ischemic attack (TIA) are major causes of morbidity and mortality worldwide, with the World Stroke Organization reporting that one in four adults aged over 25 years will experience a stroke. According to the American Stroke Association, ischemic stroke is a critical condition in which a blocked blood vessel leads to brain cell death due to a lack of oxygen and nutrients. Conversely, although TIA involves a temporary blockage without permanent damage, it is associated with a high risk of imminent stroke, emphasizing the urgent need for treatment within the first 48 h. 1 These conditions can arise from various causes, including atherosclerotic, cardiogenic, lacunar, cryptogenic, and hemorrhagic mechanisms, 2 along with modifiable (such as diet, hypertension, and smoking) and unmodifiable (such as age and genetics) risk factors.1,3
Pathophysiologically, vessel occlusion leads to rapid cell death in the ischemic core, whereas the surrounding penumbra, which may still harbor salvageable cells, undergoes neuroinflammation, excitotoxicity, oxidative stress, and processes leading to apoptosis or autophagy.4,5 The substantial burden of ischemic stroke and TIA greatly impacts the quality of life of patients, thus placing considerable strain on the healthcare system.
Recurrent stroke poses a high risk of severe outcomes, highlighting the need for effective secondary prevention. In this regard, antiplatelet therapy is of paramount importance. Agents such as aspirin, clopidogrel, and ticagrelor inhibit platelet aggregation, thereby reducing the likelihood of ischemic events. 6 Evidence from the International Stroke Trial (IST) and the Chinese Acute Stroke Trial (CAST) supports the use of aspirin within 48 h of onset,7–9 whereas recent trials, such as CHANCE and POINT, emphasize the benefits of dual antiplatelet therapy (DAPT) in reducing stroke recurrence.10,11 However, the increased bleeding risk associated with DAPT is attributed to its widespread use. 12
Our study aimed to evaluate the efficacy and safety of DAPT in secondary stroke prevention through a robust statistical analysis of current randomized controlled trial (RCT) evidence, focusing on recurrent ischemic strokes, major bleeding events, and all-cause mortality. Moreover, subgroup analyses of age, sex, comorbidities, and therapy timing and duration were conducted to assess the impact of DAPT, aiming to guide clinical practice and inform guidelines for personalized treatment approaches, thus enhancing therapeutic success and minimizing side effects.
Methods
We conducted a systematic review and meta-analysis, according to the Cochrane Handbook for Systematic Reviews of Intervention and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 13 As our study is a systematic review, ethical approval or permission was not needed. However, we registered the study protocol in PROSPERO (CRD42024587084).
Data sources and search strategy
A comprehensive systematic literature search of Cochrane, Scopus, PubMed (MEDLINE), Web of Science, and Embase was performed from inception until 15 August 2024. The search was conducted without specific limitations on criteria. Details of the search strategy are reported in Table S1.
Eligibility criteria
We utilized the PICO (Population, Intervention, Comparison, and Outcome) framework to include studies based on the following inclusion criteria: (a) the population included patients with acute ischemic stroke (minor or mild) or TIA; (b) the intervention was DAPT; (c) the comparator was the use of aspirin alone; and (d) the outcomes included recurrent ischemic stroke, recurrent hemorrhagic stroke, all-cause mortality, cardiovascular-related death, major adverse cardiovascular events (MACE), myocardial infarction, and bleeding. Regarding the study design, clinical trials (RCTs) were included. Observational studies, review articles, animal trials, letters to editors, commentaries, editorials, case reports, conference abstracts, studies with overlapping data, and in vitro studies were excluded from the analysis.
Study selection
The articles obtained through the systematic search were uploaded to EndNote Reference Library, where duplicates were identified and removed. After removal of duplicates, the titles and abstracts of the searched articles were uploaded to the Rayyan website and screened for relevance by two authors (S.A. and Z.B.). 14 Potentially eligible studies were then retrieved for full-text screening. The final list of included studies was determined through discussion and consensus among all authors. Disagreement among authors was resolved by a senior author (R.O.). The reference lists of the retrieved studies were manually screened for any additional eligible studies.
Data extraction
Data extraction forms were created using Excel Sheets (Microsoft Corporation, Microsoft Excel, United States). The data were extracted separately by three authors (Z.B., M.H., and O.J.), and any differences among authors were resolved by a senior author (R.O). For each study, the following information was extracted: (a) year; (b) country; (c) study design; (d) number of patients in each group; (e) DAPT and aspirin doses; (f) time of treatment initiation; and (g) conclusion. Baseline characteristics of the patients, including sex, age, smoking history, hypertension, diabetes, history of ischemia or myocardial infarction, and history of stroke or TIA, were extracted. We extracted the efficacy and available safety outcomes; primary safety outcomes included recurrent ischemic stroke, recurrent hemorrhagic stroke, all-cause mortality, cardiovascular-related death, MACE, myocardial infarction, and bleeding.
Risk of bias and certainty of evidence
Two authors (M.O. and B.B.K.) assessed the RCTs’ quality according to the Cochrane Risk of Bias 2 (ROB2) assessment tool. 15 The following items were assessed: (a) randomization process; (b) deviation from intended interventions; (c) missing outcome data; (d) measurement of the outcome and patients; (e) selection of reported bias; and (f) overall bias. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) scale was used to evaluate the strength and level of evidence for recommendations and was stratified into the following four categories: 16 (a) high quality, indicating no further research is needed and that further research is unlikely to change the confidence of the effects estimation; (b) moderate quality, indicating that more studies can affect the confidence of the effects estimation; (c) low quality, indicating further research is likely to have a critical impact on the confidence of the effects estimation; and (d) very low quality, indicating uncertainty about the effects estimation.
Statistical analysis
We used RStudio software (Public Benefit Corporation (PBC), United States) version 4.3.2 for statistical analyses. 17 To compare dichotomous outcomes, we used risk ratios (RR) with 95% confidence intervals (CIs) using the inverse variance (IV) method and random effect. P-values of <0.05 were considered to indicate statistical significance. Absolute effect size was calculated using the difference in the event rates between the DAPT and aspirin alone groups. To assess statistical heterogeneity, we used the inconsistency test (I2), and the heterogeneity was considered significant when the I2 statistic exceeded 50% or had a P-value of <0.10. For trial sequential analysis (TSA), we comprehensively assessed the magnitude of effect sizes rather than relying on binary outcome significance. TSA was performed using TSA software version 0.9.5.10 Beta (Copenhagen Trial Unit, Copenhagen, Denmark). Detailed guidelines for the software are available in the user manual. 18 We estimated the required sample size for the meta-analysis with a power of 80% and a two-sided type I error rate of 5%, employing the O’Brien-Fleming α-spending function. For the superiority analysis, a definitive outcome was confirmed when the cumulative Z-curve crossed the superiority boundary. The risk difference in each outcome between the DAPT and aspirin alone groups was assumed to follow the specified values, and the minimum sample size was calculated to ensure that the Z-curve crossed the superiority boundary.
Results
Search results
We obtained 2278 studies from 4 electronic databases. Using EndNote software, 1296 duplicate studies were removed, and 982 studies remained. After screening by titles and abstracts, 977 studies were excluded. We evaluated the full texts of the remaining five studies for eligibility. Finally, five papers10,11,19–21 were included in our meta-analysis. The study selection process is shown in Figure S1.
Summary of the included studies
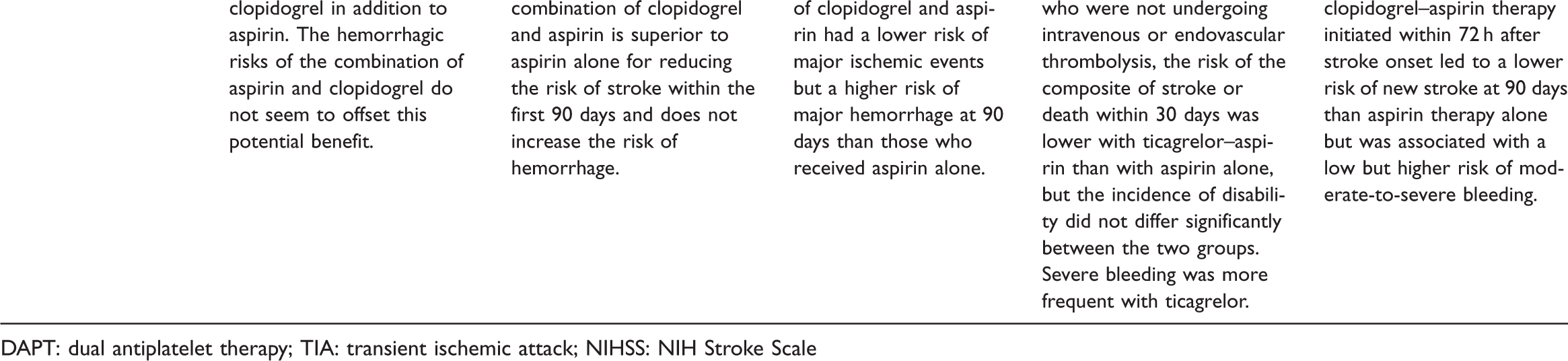
Five RCTs involving a total of 27,563 patients were included in this systematic review and meta-analysis. Three of the included studies were published before 2020,10,11,20 and two were published after 2020.19,21 Two of the included studies were conducted in China,10,19 two in a multinational population,11,21 and one in the northern United States. 20 All studies were double-blinded RCTs. The treatment group was administered aspirin and clopidogrel in four studies,10,11,19,20 whereas the treatment group in the fifth study included aspirin and ticagrelor. 21 The control group was constant (aspirin alone) in all studies. Participants in two of the included studies received antiplatelet therapy for 90 days,11,20 those in another two studies received it for 21 days,10,19 and those in one study received it for 30 days. 21 Antiplatelet therapy was initiated within 24 h in three studies,10,20,21 within 12 h in one study, 11 and within 72 h in one study. 19 The duration of follow-up was 90 days in four studies10,11,19,20 and 30 days in the fifth study. 21 The characteristics of all included studies are summarized in Table 1.
Characteristics of the included studies.

DAPT: dual antiplatelet therapy; TIA: transient ischemic attack; NIHSS: NIH Stroke Scale
The patient age ranged from 63 to 68 years in the DAPT group and from 62.0 to 68.2 years in the aspirin alone group. The proportions of females in the DAPT and aspirin alone groups were 33.0%–42.5% and 34.7%–50.0%, respectively. Comorbidities included hypertension (DAPT group: 46.0%–77.8%, aspirin alone group: 53.0%–76.9%) and diabetes (DAPT group: 12.0%–28.8%, aspirin alone group: 9.0%–28.3%). The proportions of patients with a history of current or previous smoking ranged from 27% to 43.2% in the DAPT group and from 24.0% to 42.7% in the aspirin alone group. The proportions of patients with myocardial infarction/ischemia ranged from 1.7% to 10.6% in the DAPT group and from 2.0% to 9.8% in the aspirin alone group. The detailed characteristics of the included patients are summarized in Table 2.
Characteristics of the included patients.
DAPT: dual antiplatelet therapy; TIA: transient ischemic attack
Quality assessment and GRADE summary
ROB-2 quality assessment tool was used to assess the quality of the included RCTs. Four of the five included studies had a low risk of bias.10,11,19,21 Only one study 20 had a moderate risk of bias. This concern was due to issues identified in the second domain, specifically due to deviations from the intended intervention. The details of the quality assessment are reported in Figure S2. We conducted GRADE assessment of the main outcomes such as recurrent ischemic stroke, recurrent hemorrhagic stroke, all-cause mortality, MACE, and bleeding. The findings of the GRADE assessment are summarized in Table S2.
Outcomes
Recurrent stroke
All studies reported the recurrence of stroke (ischemic or hemorrhagic stroke).10,11,19–21 Upon comparison between DAPT and aspirin alone, the pooled RR of 0.77 (95% CI: 0.70–0.83, P < 0.01) indicated that DAPT significantly reduced the risk of stroke recurrence. No heterogeneity was observed between the studies (I2 = 0%) (Figure 1(a)). Subgroup analyses were conducted for the type of stroke; all studies reported the recurrence of ischemic stroke.10,11,19–21 Upon comparison between DAPT and aspirin alone, the pooled RR of 0.74 (95% CI: 0.68–0.81, P < 0.01) indicated that DAPT significantly reduced the risk of ischemic stroke recurrence. No heterogeneity was observed between the studies (I2 = 0%) (Figure 1(b)). Recurrence of hemorrhagic stroke was reported in all RCTs. 10,11,19–21 The pooled RR of 2.13 (95% CI: 1.09–4.17, P = 0.03) indicated that DAPT was significantly associated with a higher risk of hemorrhagic stroke recurrence. Low heterogeneity was detected between the studies (I2 = 7%) (Figure 1(c)).

Pooled meta-analysis for (a) recurrent stroke (ischemic or hemorrhagic); (b) ischemic stroke; and (c) hemorrhagic stroke.
We conducted a TSA of the five trials assessing the recurrence of ischemic and hemorrhagic stroke with an overall sample size of 27,563. For hemorrhagic stroke, the required sample size was 28,925 patients, and the cumulative Z-line crossed the conventional and superiority boundaries, favoring the use of aspirin alone; however, the overall sample size was less than that required for achieving a definitive result despite the statistically significant pooled effect (Figure 2(a)). For ischemic stroke, the required sample size was 5043, and the final point on the cumulative Z-line crossed the conventional and superiority boundaries, favoring the use of DAPT; the sample size surpassed the required sample size, thus indicating sufficient evidence (true positive) (Figure 2(b)).

Trial sequential analysis of dual antiplatelet therapy and aspirin alone using 80% power and 5% significance: (a) recurrent hemorrhagic stroke; (b) recurrent ischemic stroke; (c) all-cause mortality; (d) major adverse cardiovascular events and (e) bleeding.
All-cause mortality
Four studies reported the all-cause mortality outcome10,11,19,21 (Figure 3(a)). Upon comparison between DAPT and aspirin alone, the pooled RR of 1.28 (95% CI: 0.95–1.71, P = 0.1) indicated no statistically significant differences between the two groups. No heterogeneity was observed between the studies (I2 = 0%). We conducted a TSA of the four trials assessing all-cause mortality. The required sample size was 80,408 patients, and the number of patients in the 4 included studies was 27,167. The cumulative Z-line did not cross the conventional or superiority boundaries, and the final point was not within the inner boundary, suggesting a lack of evidence to confirm the negative result (insignificance) and indicating the possibility of a false negative (Figure 2(c)).

Pooled meta-analysis of (a) all-cause mortality; (b) cardiovascular-related death; and (c) major adverse cardiovascular events.
Cardiovascular-related death
Three studies reported cardiovascular death19,11,10 (Figure 3(b)). Upon comparison between DAPT and aspirin alone, the pooled RR of 1.38 (95% CI: 0.81–2.33, P = 0.23) indicated no statistically significant differences between the two groups. No heterogeneity was observed between the studies (I2 = 0%).
MACE
All studies reported MACE10–11,19–21 (Figure 3(c)). Upon comparison between DAPT and aspirin alone, the pooled RR of 0.77 (95% CI: 0.71–0.84, P < 0.01) indicated that DAPT significantly reduced the risk of MACE. No heterogeneity was observed between the studies (I2 = 0%). TSA suggested that a required sample size of 6215. The final point on the cumulative Z-line crossed the conventional and superiority boundaries, favoring DAPT with an overall sample size (27,563) greater than that required for a definitive result; thus, the evidence was considered sufficient (true positive) (Figure 2(d)).
Moderate-to-severe bleeding
All studies reported bleeding events10–11,19–21 (Figure 4(a)). Upon comparison between DAPT and aspirin alone, the pooled RR of 2.21 (95% CI: 1.48–3.32, P < 0.01) indicated that DAPT significantly increased the risk of bleeding events. Low heterogeneity was detected between the studies (I2 = 29%). TSA suggested that a sample size of 14,902 was required. The final point on the cumulative Z-line crossed the conventional and superiority boundaries, favoring aspirin alone, and the overall sample size of 27,561 was greater than that required for sufficient and definitive evidence (true positive) (Figure 2(e)).

Pooled meta-analysis of (a) moderate-to-severe bleeding and (b) myocardial infarction.
Myocardial infarction
Four studies reported myocardial infarction19,11,10,21 (Figure 4(b)). Upon comparison between DAPT and aspirin alone, the pooled RR of 1.63 (95% CI: 0.77–3.46, P = 0.2) indicated no statistically significant differences between the two groups. No heterogeneity was observed between the studies (I2 = 0%).
Discussion
DAPT reduces ischemic events during stroke management by inhibiting platelet aggregation via cyclooxygenase (COX)-1 suppression and P2Y12 receptor obstruction. This combination is crucial for preventing thrombosis in patients with minor strokes or those with TIA. Additionally, DAPT attenuates inflammation via the regulation of cytokines, particularly IL-6, decreases neutrophil infiltration, improves recovery, and diminishes pyroptosis and inflammation-related tissue damage.22,23 Our findings indicate that DAPT reduces ischemic stroke recurrence. However, the increased risk of hemorrhagic stroke warrants careful patient selection, particularly in patients prone to bleeding or resistance to antiplatelet therapy.
Evidence regarding DAPT for secondary ischemic stroke prevention underscores the importance of short-term DAPT in reducing recurrent ischemic events (e.g. combining aspirin with clopidogrel or other agents). DAPT is especially effective in high-risk patients following minor ischemic stroke or TIA. The READAPT study demonstrated the short-term efficacy of DAPT in real-world settings, reporting a low ischemic recurrence rate (3.3%) and moderate bleeding complication rate (2.7%), despite wider application beyond RCT protocols. 24 Long-term DAPT, such as acetylsalicylic acid and dipyridamole, considerably enhances neurological and cognitive outcomes with good tolerability, reducing the risk of recurrent ischemic stroke and severe bleeding. 25 A meta-analysis conducted among patients undergoing thrombolysis revealed that DAPT improved their 90-day functional outcomes without increasing intracranial hemorrhage or mortality; however, it did not lower the stroke recurrence rates. 26 These findings indicate the benefits of DAPT in secondary stroke prevention, with optimal use varying by patient characteristics such as stroke severity and therapy initiation timing. Our study corroborates these findings, demonstrating that DAPT significantly reduces the risk of recurrent ischemic stroke (RR: 0.74, P < 0.01) without significant heterogeneity and is linked to a higher risk of hemorrhagic stroke (RR: 2.13, P = 0.03).
The CHANCE and POINT trials demonstrated the efficacy of short-term DAPT in reducing recurrent ischemic events within 90 days of minor ischemic stroke or high-risk TIA. The CHANCE trial demonstrated a 32% reduction in stroke recurrence with DAPT compared with aspirin alone, without a significant increase in major bleeding risks, whereas the POINT trial reported a 25% reduction in stroke recurrence or death, with a higher risk of major hemorrhage. The CHANCE-2 trial highlighted that the benefits of DAPT may be less pronounced in patients aged over 80 years with higher bleeding and mortality risks. 27 Our study findings align with those of CHANCE and POINT trials, demonstrating that DAPT reduces recurrent ischemic events; however, the increased bleeding risk warrants further consideration, especially in older populations.
Patient demographics substantially influenced the DAPT outcomes in stroke prevention, with factors such as age, comorbidities, and geographical location affecting treatment patterns and adherence. Studies have shown that older patients, particularly those aged over 80 years, experience higher rates of adverse outcomes, such as bleeding, while receiving DAPT. A UK-based study reported that 13.9% of patients did not receive antiplatelet therapy within 90 days of hospitalization for ischemic stroke or TIA. Furthermore, among those who received the therapy, 62.3% switched to single antiplatelet therapy within a year, potentially owing to concerns regarding DAPT-related complications. 28 A US-based study revealed that DAPT was less frequently prescribed than single antiplatelet therapy, and patients remained at high risk of recurrent ischemic stroke within 90 days, suggesting that demographic and systemic factors contribute to suboptimal therapy initiation and adherence. 29 Our study reported these findings, with subgroup analyses identifying variations in the outcomes based on patient demographics, indicating that DAPT requires adjustments based on age and comorbidities to minimize adverse events while maximizing efficacy.
Risk–benefit analysis of DAPT in post-stroke patients highlights a delicate balance between reducing ischemic stroke recurrence and increasing bleeding risks. DAPT, typically involving aspirin and clopidogrel, effectively improves functional outcomes within 90 days of minor ischemic stroke or TIA. A meta-analysis revealed that DAPT post-intravenous thrombolysis did not increase the risk of intracranial hemorrhage or 90-day mortality risk while enhancing neurological outcomes. 26 However, prolonged DAPT, especially in procedures such as carotid endarterectomy, raises bleeding risks despite slightly lowering the stroke incidence. 30 For high-risk patients, the OPT-CAD study indicated that extending DAPT beyond 12 months reduces stroke recurrence without significantly increasing severe bleeding risks, suggesting benefits for well-monitored patients. 31 Our findings align with this balance. Although DAPT reduces ischemic stroke recurrence, it notably increases moderate-to-severe bleeding risks (RR: 2.21, P < 0.01).
Updated clinical guidelines for DAPT in secondary stroke prevention emphasize optimizing the therapy duration and balancing efficacy with bleeding risk. DAPT, combined with aspirin and clopidogrel, is most effective for short durations (21–30 days) in patients with minor ischemic stroke or high-risk TIA, as demonstrated by several RCTs.10,19 Prolonged DAPT increases the risk of hemorrhagic events without further reducing the incidence of recurrent strokes, necessitating personalized approaches based on individual bleeding and thrombotic risk. The CHANCE and POINT trials demonstrated that short-term DAPT is more effective than single antiplatelet therapy in preventing early recurrent ischemic events; however, prolonged therapy does not offer additional protection and increases the incidence of bleeding complications. 6 Our study supports these guidelines, demonstrating that short-term DAPT significantly reduces ischemic stroke recurrence, while extended use may increase bleeding risk, underscoring the need for individualized treatment.
Conclusion
This meta-analysis demonstrated that DAPT significantly reduces the risk of recurrent ischemic stroke and MACE compared with aspirin alone. However, the use of DAPT is associated with an increased risk of hemorrhagic stroke and bleeding events. TSA revealed that sufficient evidence for recurrent ischemic stroke, MACE, and bleeding was achieved. These findings highlight the importance of careful patient selection while prescribing DAPT, particularly for individuals at high risk of bleeding. Further studies are warranted to provide sufficient evidence regarding recurrent hemorrhagic stroke and all-cause mortality.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251337035 - Supplemental material for Dual antiplatelet therapy versus aspirin alone in acute ischemic stroke or transient ischemic attack: A meta-analysis and trial sequential analysis of randomized controlled trials
Supplemental material, sj-pdf-1-imr-10.1177_03000605251337035 for Dual antiplatelet therapy versus aspirin alone in acute ischemic stroke or transient ischemic attack: A meta-analysis and trial sequential analysis of randomized controlled trials by Ramez M Odat, Sakhr Alshwayyat, Zainab I Bahdar, Mohammad Abdelraheem, Basma B Khalefa, Omar Jarah, Mohammad H Obeidat, Mohammad E Bani Khalaf, Aon J Bani Khalaf, Ayham Mohammad Hussein, Jehad A Yasin, Hamdah Hanifa and Hritvik Jain in Journal of International Medical Research
Footnotes
Acknowledgements
None.
Author contributions
R.O., S.A., Z.B., M.A., B.K., H.J., and O.J. developed the concept and designed the systematic review. R.O., M.O., and M.B. contributed to acquisition, analysis, or interpretation of data. A.K., A.H., H.H, and J.Y. wrote the initial manuscript. All authors contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declare no competing financial interests.
Data availability statement
The data generated in this study are available upon reasonable request from the corresponding author.
Funding
None.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.