
Abstract
Osteonecrosis is a pathological condition that could lead to a debilitating physical disease and impede daily activities. It is generally categorised into aetiology – primary (idiopathic) or secondary. When direct damage to the bone vasculature or direct injury of the bone marrow is related to an identifiable cause such as traumatic injuries, steroid or bisphosphonate use, increased alcohol intake, sickle cell disease, autoimmune diseases, chemotherapy or malignancy, it is categorised as secondary osteonecrosis. On the other hand, osteonecrosis wherein the mechanisms of development are not fully understood is categorised as primary or idiopathic osteonecrosis. This category includes inherited thrombophilia and hypofibrinolysis as potential causes. There are no clear guidelines or general agreements about anticoagulation treatment and duration in primary osteonecrosis due to thrombophilia or hypofibrinolysis. We report a case of primary osteonecrosis associated with hypofibrinolysis and successful control with lifelong direct oral anticoagulation therapy.
Keywords
Introduction
Osteonecrosis is generally categorised into its aetiological development – primary (idiopathic) or secondary causes. Secondary osteonecrosis occurs when direct damage to the bone vasculature or direct injury of the bone marrow is related to an identifiable cause such as traumatic injuries, steroid or bisphosphonate use, increased alcohol intake, sickle cell disease, autoimmune diseases, chemotherapy or malignancy. 1 On the other hand, osteonecrosis is categorised as primary or idiopathic when the development of the osteonecrosis is not fully understood. In this category, inherited thrombophilia and hypofibrinolysis are reported in medical literatures as potential causes. 2
The abnormalities and gene mutations of the proteins in the coagulation and fibrinolytic pathways are well described in the pathogenesis of osteonecrosis. Studies and retrospective reports suggest an increased prevalence of the Factor V Leiden mutation in patients with hip or knee osteonecrosis compared with healthy controls.3–6 In an observational study of patients with osteonecrosis, 82% of osteonecrosis patients were found to have at least one coagulopathy compared with 30% of controls, and 47% of patients with osteonecrosis had two or more coagulopathies, compared with 3% of controls. 7
Many studies have recently been done on thrombophilia and hypofibrinolysis associated with osteonecrosis. These are mostly related to problems within the coagulation cascade. Two separate studies found that 12 of 32 patients diagnosed with primary osteonecrosis of the knee and 10 of 35 patients diagnosed with primary osteonecrosis of the femoral head had Factor V Leiden or mutations on the prothrombin 20210A gene.5,6 Both studies suggested that coagulation abnormalities may play a role in osteonecrosis of the knee and the femoral head. Another problem that leads to thrombophilia is the resistance to activated protein C or low levels of protein C. 8 These have been found in patients with primary or secondary osteonecrosis of the femoral head. High levels of Factor VIII is another heritable thrombophilic condition that increases the risk for both primary and secondary osteonecrosis of the femoral head.9,10 It has also been suggested that hypofibrinolysis (i.e. increased levels of lipoprotein(a), high levels of plasminogen activator inhibitor and subsequently low levels of stimulated tissue plasminogen activator (tPA)) leads to inadequate lysis of venous thrombi in bone, compromised bone venous circulation, venous hypertension of the bone and, ultimately, hypoxia within the bone leading to osteonecrosis. 8
In our search of the literature, we found several reports wherein anticoagulation, including direct oral anticoagulants (DOACs), was used in primary osteonecrosis. Currently, the main treatment of osteonecrosis due to hypofibrinolysis is with a low-molecular-weight heparin (LMWH), enoxaparin. One study showed that patients with primary osteonecrosis of the hip treated with LMWH had lower rates of progression from the pre-collapsed to the collapsed stage of the hip. 11 Studies also reported that long-term use of anticoagulation prevents the progression of idiopathic osteonecrosis, helps with pain and improves functionality.12,13 In one study, patients with Factor V Leiden or resistance to activated protein C who developed osteonecrosis of the hip and were started on long-term (4–16 years) anticoagulation therapy did not show signs of radiological progression and remained at low Ficat (I and II) stages. 13 Most of the samples in the same study were treated with warfarin (Coumadin). DOACs were utilised in only two patients – one patient was treated with dabigatran (Pradaxa) 150 mg twice daily after completion of 90 days treatment with enoxaparin (Lovenox), while the other patient was on warfarin, then switched to rivaroxaban (Xarelto) 20 mg. In another case, apixaban (Eliquis) 5 mg twice daily was used to treat primary osteonecrosis associated with thrombophilia–hypofibrinolysis instead of warfarin. 14
Several studies also supported that despite being asymptomatic, untreated osteonecrosis progresses to symptomatic disease. One study found that, in general, regardless of underlying cause (primary or secondary), asymptomatic osteonecrosis has a high prevalence of progression to symptomatic disease. 15 In another study, a subgroup of patients with asymptomatic idiopathic osteonecrosis, 46.2% progressed to symptomatic osteonecrosis. 16 Similarly, in a study mentioned previously, 50% to 80% of patients’ hips, initially Ficat stage II, progressed to Ficat stages III to IV within 2 years without anticoagulation treatment. 13
Our report focuses on a case of primary osteonecrosis associated with hypofibrinolysis and successful control with lifelong direct oral anticoagulation therapy of low-dose apixaban.
Case presentation
A 40-year-old Caucasian female with no significant medical morbidities presented in 2013 with persistent left leg pain after she twisted her left ankle. An evaluation with plain X-ray and magnetic resonance imaging (MRI) of her left lower extremity revealed abnormal densities, suggesting osteonecrosis, in the distal femur (see Figures 1 and 2).
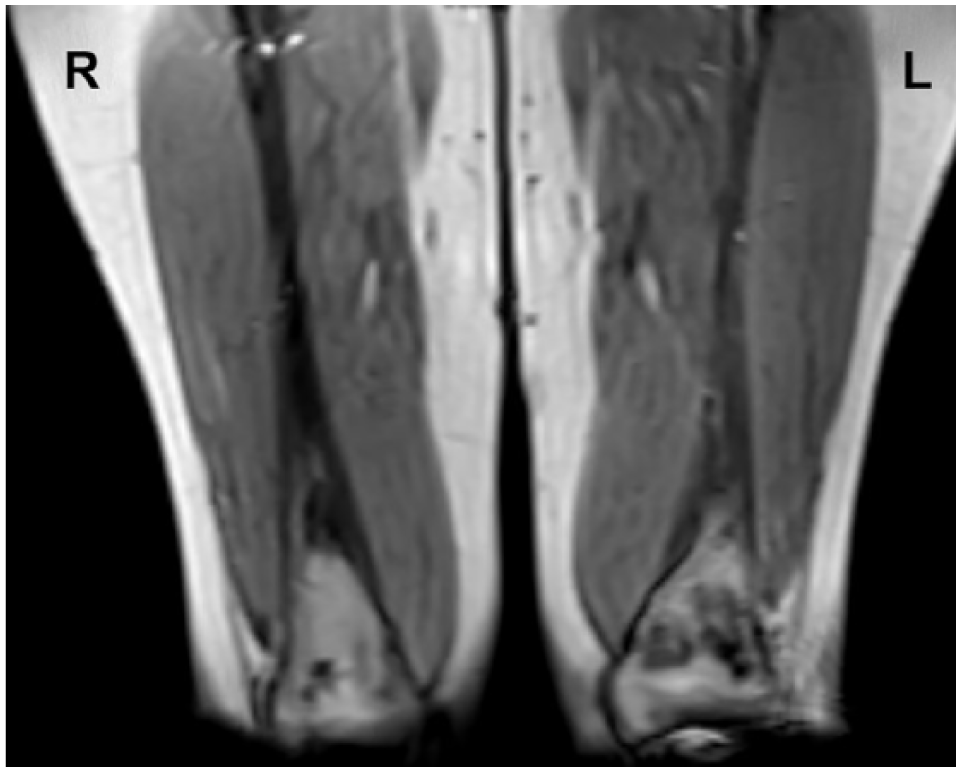
MRI revealed bilateral abnormal signal intensities in the distal femurs, suggesting osteonecrosis.

The lesion on the left distal femur was larger and was the main source of the patient’s pain.
Detailed review of her history of present illness, past medical history and medication did not reveal apparent secondary causes. Subsequently, an evaluation to rule out primary causes of osteonecrosis was initiated and revealed that she was homozygous for the 4G variant in the Plasminogen Activator Inhibitor–1 (PAI-1) gene.
Neoplastic process was ruled out with positron emission tomography/computed tomography (PET/CT) scan, which also revealed osteonecrosis with no evidence of other abnormal bone activity.
Diagnosis of primary osteonecrosis was made based on her hypofibrinolytic status due to homozygosity for the 4G variant in the PAI-1 gene. As genetic testing confirmed 4G/4G mutation of the PAI-1 gene, plasminogen activator inhibitor activity was not measured in this patient. She was accordingly seen in the bone health clinic and, with the absence of other thrombophilic abnormalities, we started her on full anticoagulation treatment with enoxaparin, 1 mg/kg twice daily for 6 months. She reported that her symptoms improved drastically while on enoxaparin. A few months following completion of the 6-month course, her symptoms, specifically bone pain, recurred. She was re-evaluated with imaging studies including MRI of the lower extremities, which showed osteonecrosis. She was then referred to the haematology clinic for recommendations.
Based on the patient’s history and presentation, it was strongly felt that the only real solution would be to pursue lifelong anticoagulation. The nature of the condition was discussed with the patient, highlighting the chronicity of the problem and the expected course of the disease. The benefits and risks of lifelong anticoagulation were discussed with the patient. Her continued deterioration and worsening symptoms when she is off anticoagulation convinced her to consider lifelong anticoagulation. After discussing the options for anticoagulation, it was decided to start her on a prophylactic dose of apixaban, 2.5 mg twice daily.
She continued to follow up regularly with the haematology clinic. Her symptoms immediately resolved with DOAC therapy and subsequent radiological imaging showed no further disease progression. After 1 year of apixaban therapy, the patient still reports no bone or joint pain. She has had no complications with her anticoagulation. At the time of the diagnosis, the MRI revealed multiple focal lesions in the intramedullary canal of both right and left distal femurs. The lesions were more prominent in the left distal femur with the largest lesion measuring 4.9 cm maximum length by 2.2 cm transverse by 1.1 cm anterior–posterior, which was roughly estimated to be 30% involvement of distal femur. Six-monthly follow-up imaging studies within a 2 year period indicated stable bone changes in the femurs bilaterally with no progression. Considering her marked improvement, the patient has remained on anticoagulation and plans were set to follow up every 6 months with X-ray imaging to monitor lesions and MRI imaging if needed.
Discussion
When the fibrin clot is formed downstream of the clotting cascade, plasminogen is converted to plasmin by tPA. Plasmin then begins to break up the fibrin clot. PAI-1 plays a role in controlling plasmin activity by inhibiting tPA, ultimately preventing haemorrhagic events. In cases wherein there is an elevation in PAI-1 level, a decrease in activity of stimulated tPA becomes imminent, and subsequently clot degradation becomes impaired. This state of hypofibrinolysis ultimately leads to increased clot formation, decreased blood flow and hypoxia within the bone structure, which may lead to osteonecrosis.
The presentation of leg pain in our patient is typical of osteonecrosis. This pain is often embedded deep within the bone structure and can potentially be debilitating. After further studies of the diagnosis of idiopathic osteonecrosis, genetic testing (i.e. DNA PCR assay) revealed that our patient had a homozygous 4G/4G polymorphism in the PAI-1 gene, predisposing her to an increase in production and, subsequently, elevated levels of PAI-1. A study of patients with osteonecrosis of the hip, whose genes were analysed for associations with thrombophilia or hypofibrinolysis, found that there was no difference in Factor V Leiden, prothrombin or methylenetetrahydrofolate reductase mutation between patients and healthy subjects. 9 However, the same study revealed that 41% of the patients with osteonecrosis were homozygous for 4G/4G polymorphism in the PAI-1 gene compared with 20% of healthy subjects. In comparison, only 19% of patients with osteonecrosis had 5G/5G homozygosity compared with 36% of healthy subjects. A meta-analysis has also shown that a 4G/5G polymorphism in the PAI-1 gene increases the susceptibility of osteonecrosis of the femoral head. 17 A study within the Korean population found that three single nucleotide polymorphisms (SNPs) of the PAI-1 gene, including one in the 4G allele, were associated with increased risk of osteonecrosis of the femoral head. 18 As suggested in the studies mentioned, although homozygosity for 4G polymorphism in the PAI-1 gene predisposes patients to have both high PAI-1 antigen and high PAI-1 activity, increasing the risk of hypofibrinolysis, not all will develop osteonecrosis.
Better understanding of primary osteonecrosis associated with thrombophilia and hypofibrinolysis has paved the way for studies using anticoagulants as standard treatment. Studies and case reports have demonstrated benefits in using warfarin, heparin or LMWH in these cases. A patient with protein S deficiency who developed idiopathic osteonecrosis became asymptomatic after 1 year of treatment with warfarin. 19 In a patient with protein S deficiency who developed multifocal osteonecrosis, heparin was used as the initial treatment and converted to warfarin. 20 Enoxaparin has also shown to be beneficial in patients with osteonecrosis of the hip or the knee associated with thrombophilia or hypofibrinolysis. 21 Symptom improvement (e.g. reduction of pain) and regression of joint damage were evident after 3 months of treatment with enoxaparin.
The role of DOACs is now well established in thromboembolic disease and in stroke prevention associated with cardiac arrhythmias. While these conditions have historically been treated with warfarin or heparin, the emergence of the DOACs have now offered more options in treatment and have also been found to be more beneficial in some respects. One major benefit is the reduction in risk of intracranial bleeding compared with warfarin. However, trials have shown that rivaroxaban and dabigatran (but not apixaban) increase the risk of gastrointestinal bleed compared with warfarin.22,23 DOACs may also be more convenient for patients as they are taken orally compared with heparin, which is administered subcutaneously. Coagulation testing is minimal compared with warfarin, wherein patients need periodic blood tests to check their international normalised ratio (INR) or prothrombin time (PT) and readjust the next dose accordingly. Furthermore, the DOACs have fewer drug interactions than warfarin, which benefit patients who are taking several medications.
The benefits of DOACs have made them a more preferable option compared with heparin and warfarin. However, there are also limitations to using DOACs. As they are still comparatively new in the market, antidotes are not yet readily available when needing immediate reversal. Two antidotes in the market are idarucizumab (Praxbind) and andexanet alfa (Andexxa). Idarucizumab is a reversal direct thrombin inhibitor specifically for dabigatran. In May 2018, Food and Drug Administration (FDA) approved andexanet alfa as an antidote for two Factor Xa inhibitors apixaban and rivaroxaban, when life-threatening or uncontrolled bleeding occurs. 24 Compared with testing PT or INR for warfarin or the activated partial thromboplastin time (APTT) for heparin, DOACs cannot be readily measured quantitatively. 25 However, they generally have a shorter half-life compared with warfarin. Dose reduction of DOACs is recommended in all patients with renal impairment (e.g. as it is excreted by the kidneys, dabigatran is not advisable for use in patients with severe renal impairment). 26 Risks and benefits need to be evaluated when starting patients on DOACs.
Conclusion
In the case presented, the patient had homozygous 4G variant in the PAI-1 gene, which increased her risk of hypofibrinolysis leading to osteonecrosis. Although osteonecrosis associated with thrombophilia and hypofibrinolysis has historically been successfully treated with warfarin or LMWH, our patient’s osteonecrosis continued to recur despite treatment with enoxaparin. However, since commencing daily low-dose apixaban, the disease has been under control and she is able to resume her daily activities without further pain or difficulty.
Footnotes
Acknowledgements
MMH is the primary author of the case report. SE contributed significantly to the case presentation. MA is the medical oncologist providing care to the patient, has contributed to the abstract and case presentation, and is the primary advisor of the case report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Verbal informed consent was initially obtained from the patient(s) for their anonymised information to be published in this article. In addition, a written consent was obtained and signed by the patient on 10 July 2018.