
Abstract
Perivascular epithelioid cell tumor (PEComa) is a rare mesenchymal tumor with unique histological and immunohistochemical characteristics. Malignant renal cell carcinoma is even rarer and its biological behavior is still not clear. We report here a case of malignant PEComa in a male patient. The first symptom of the patient was intermittent hematuria. Ultrasound and computed tomography scan showed a solid mass in the left kidney. Fibrosarcoma was initially diagnosed after radical resection of the tumor. Six years later, the patient had a tumor recurrence and underwent a second operation, through which the diagnosis of renal malignant PEComa was made. Since then, the patient received chemotherapy, a third operation, and interventional treatment because of recurrence and metastasis of the tumor, which prolonged the life of the patient for another 6 years. Malignant PEComa involving the kidney is very rare; it seems to develop slowly but will recur and metastasize. At present, surgical resection remains the best treatment.
Keywords
Background
Perivascular epithelioid cell tumor (PEComa) is a rare tumor originating in mesenchymal tissues; PEComas were defined by the World Health Organization in 2002 as “mesenchymal tumors composed of histologically and immunohistochemically distinctive perivascular epithelioid cells.” 1 The PEComa family includes angiomyolipoma, clear-cell “sugar” tumors of the lung and other organs, lymphangiomyomatosis, as well as a rare group of morphologically and immunophenotypically similar tumors occurring in soft tissues, viscera, and bones, in most body locations. 2 Evidence indicates that PEComa rarely arises in the retroperitoneum; moreover, the majority of tumors are benign and predominantly affect women. 3 We present here a case report of a male patient with malignant retroperitoneal PEComas involving the left kidney, for which the patient underwent multiple operations and treatments. To the best of our knowledge, studies on PEComa involving malignant tumors of the kidney are still rare.4–6
Case presentation
In January 2006, a 55-year-old man was admitted to a local hospital for intermittent gross hematuria. Two years before admittance, a small mass was found on the patient’s left kidney on ultrasound, but he declined further evaluation or treatment at that time. This time, ultrasound and computed tomography (CT) showed a large mass of the left kidney (130 mm × 110 mm × 80 mm). A pathological diagnosis of left renal fibrosarcoma was made after surgical removal of the tumor. Six years later, the patient was found to have a large mass behind the left peritoneum and came to our hospital for further treatment. Magnetic resonance imaging showed a large, irregular, dumbbell-shaped heterogeneous mass with poorly demarcated tumor margins, measuring 88.8 mm × 205.4 mm × 93.7 mm (Figure 1). The patient underwent a second surgery in our hospital to remove the recurrent left posterior peritoneal tumor. Histopathologic examination showed that the tumor was composed of spindle-shaped and large epithelioid cells (Figure 2). The epithelioid component was about 70%, and immunohistochemical analysis indicated the epithelioid cells in the tumor tissue were diffusely positive for HMB45 (Figure 3a, b) and melan-A, and were focally positive for vimentin, epithelial membrane antigen (EMA), and CD117. In the sarcomatoid area, the spindle cells were negative for smooth muscle actin (Figure 3c, d), desmin, chromogranin A (CgA), synaptophysin (Syn), S100, CD34, cytokeratin, and inhibin α. Thus, the final diagnosis was retroperitoneal PEComa of the kidney. Ten months after the second operation, recurrence of the left retroperitoneal tumor and right renal metastasis were found on CT scan. The patient received paclitaxel (330 mg/d) plus bevacizumab (500 mg/d) chemotherapy on March 26, April 18, and May 10, 2013. In December 2013, the patient underwent a third operation at another hospital to remove the recurrent tumor from the left retroperitoneum. One year later, the patient had another recurrence in the left retroperitoneum. He accepted interventional therapy, and the recurrent tumor grew gradually. A solitary liver metastasis was found in February 2016, and multiple liver metastases were found 6 months later. No special treatment measures were taken and the patient died 10 months later. The patient’s son consented to publication of this case report.
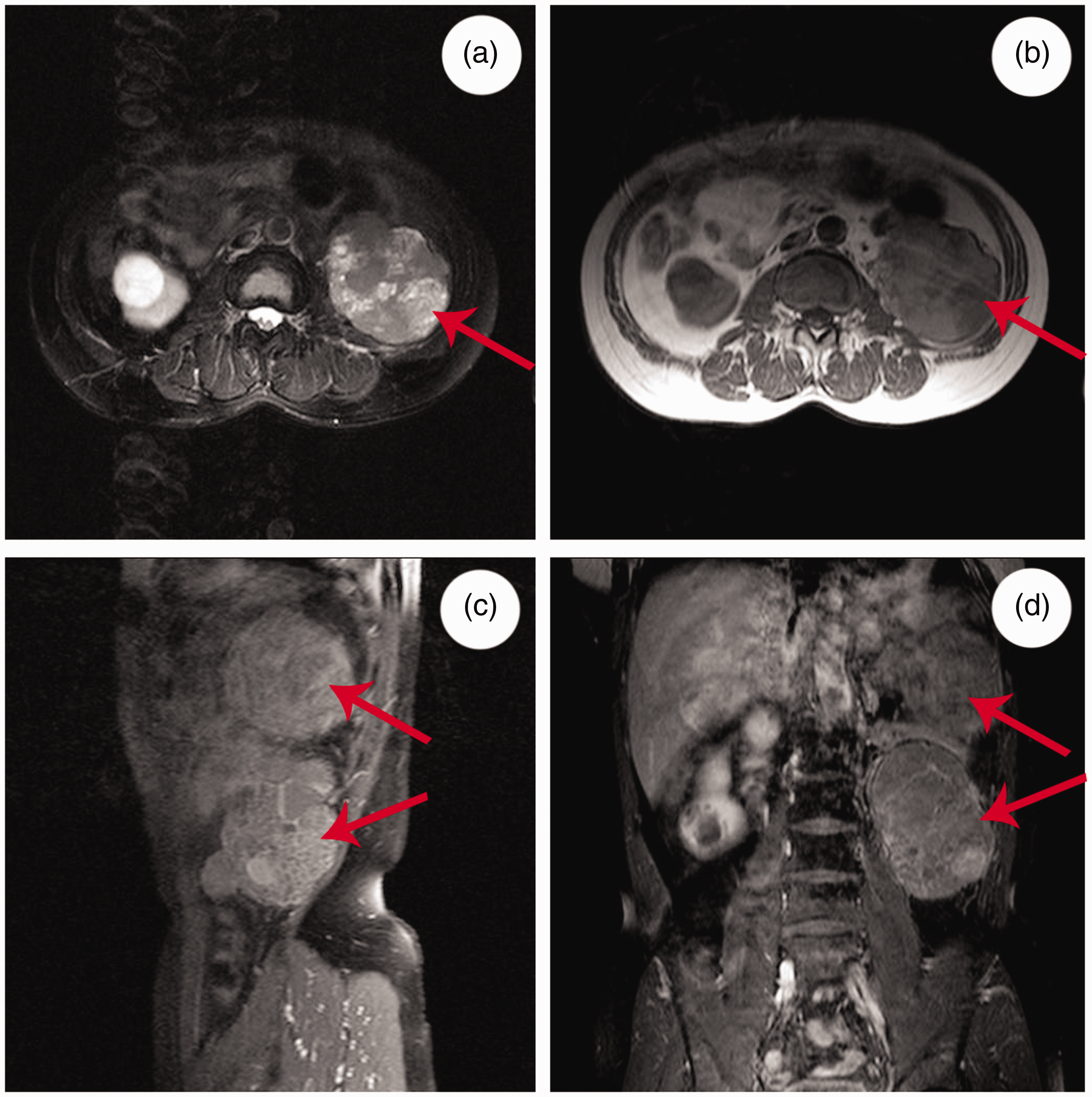
Magnetic resonance imaging of a 61-year-old man with a recurrent perivascular epithelioid cell tumor of the left kidney. (a) Axial T2 weighted image (WI) fat saturation showing slightly higher signal and higher signal (arrow); (b) axial T1WI showing slightly higher signal and lower signal (arrow); (c) enhanced sagittal T1WI fat saturation; and (d) enhanced coronal T1WI fat saturation showing the irregular mass (arrow) with moderately heterogeneous enhancement.

Hematoxylin–eosin staining of recurrent perivascular epithelioid cell tumor of the kidney (magnification, 200×; circle indicates high nuclear grade).

Immunohistochemistry demonstrating that tumor cells were positive for HMB45 (a: 200×; b: 400×) and negative for smooth muscle actin (c: 200×; d: 400×).
Discussion
Because of the rarity of PEComa, the diagnostic criteria to distinguish benign from malignant tumors have not been elaborated until recently. 7 Folpe et al. proposed criteria that are currently accepted for the diagnosis of benign or malignant PEComas. PEComas that are <5 cm with low cellularity, low nuclear grade, mitotic rate <1/50 high-power fields, and lacking infiltration, necrosis, and vascular invasion should be considered benign. Tumors that show two or more of the following are considered malignant: size >5 cm, infiltrative growth, high nuclear grade, high mitotic rate, pleomorphism, necrosis, or vascular invasion. 8 In our case, at the first two surgeries, the diameters of the primary and recurrent tumors were >10 cm. The pathology results indicated cytological atypia, evident mitotic activity, and large areas of necrosis, bleeding, and cystic changes in the mesenchyme. Therefore, the diagnosis in our case was malignant renal PEComa.
Surgery is still the main and most effective treatment for PEComa. Other than surgical resection, chemotherapy and radiotherapy are still not clear and definite for malignant tumors and the prognosis is poor. 9 In our case, the tumor recurred 6 years after the initial operation. The patient then underwent two further surgeries plus chemotherapy and vascular interventional therapy. Although developing slowly, the tumor recurred repeatedly and metastasized to the contralateral kidney and liver. The patient died due to metastatic disease 12 years after onset. Several recent studies have suggested the role of the inhibitors of the mammalian target of rapamycin (mTOR) pathway (such as sirolimus) for treating malignant PEComas. 10 Moreover, overexpression of microRNA miR-501-5p stimulates cell proliferation in kidney cells by inhibiting p53 function in a mechanism driven by mTOR signaling. In fact, downregulation of this microRNA and pharmacological treatment with proteasome and mTOR inhibitors in PEComa cells reduce cell growth by activating apoptosis. 11
In conclusion, primary renal malignant PEComa is a rare mesenchymal tumor with unique histological and immunohistochemical features. In the present study, we reported a male patient with malignant and recurrent renal PEComas. Given the rarity of malignant PEComas, their pathogenesis and biological behavior are unclear at present; surgery remains the main approach for optimal treatment. Further studies of additional cases and long-term follow-up are necessary to completely understand the behavior of malignant renal PEComa.
Footnotes
Acknowledgements
We thank the patient’s son for permission to publish this case report.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.