
Abstract
Pulmonary sarcomatoid carcinoma (PSC) is a rare and highly invasive malignant tumour. It has similar clinical manifestations and imaging features to ordinary lung cancer. This current case report describes a 65-year-old male patient who had a mass in the apicoposterior segment of the left upper lobe with haemoptysis. Imaging studies revealed a central parenchymal mass surrounded by areas of ground-glass opacity, strongly indicating the presence of a pulmonary malignancy. Intraoperatively, the tumour was discovered to have invaded the chest wall and exhibited a significant propensity for bleeding. Consequently, a left upper lobe resection accompanied by extensive pleural debridement were performed. Subsequent postoperative histopathological examination confirmed the diagnosis of PSC. Unfortunately, 1 month after the surgery, the patient presented with left-sided haemothorax. Despite employing various haemostatic interventions, the patient eventually succumbed to haemorrhagic shock. This study provides a treatment strategy reference for patients with PSC presenting as haemothorax.
Introduction
Pulmonary sarcomatoid carcinoma (PSC) is an exceedingly rare and highly aggressive form of lung cancer, with a poorer prognosis compared with nonsmall-cell lung cancer (NSCLC), which accounts for less than 1% of all lung cancer cases.1,2 Due to the challenges in differentiating PSC from ordinary NSCLC in terms of imaging, there is a propensity for clinical misdiagnosis. This can lead to lobectomy, which is typically the first-line treatment option for early-stage lung cancer, being mistakenly performed on these patients. 3 Additionally, the occurrence of refractory haemothorax resulting from PSC recurrence is rarely documented and warrants careful clinical attention. This current case report presents a patient with PSC located in the left upper lobe who initially presenting with haemoptysis. The patient underwent video-assisted thoracoscopic surgery and was discharged without any complications. However, 1 month after the surgery, the patient experienced a massive haemothorax on the surgical side.
Case report
In April 2022, a 65-year-old male patient presented to Department of Cardiothoracic Surgery, Wujin Hospital Affiliated with Jiangsu University, Changzhou, Jiangsu Province, China with a 1-month history of productive cough, followed by progressive haemoptysis lasting for 10 days. He had a history of hypertension and had quit smoking 10 years ago after smoking for a duration of 20 years. There was no significant family history of lung cancer. Upon arrival, the patient's vital signs were normal. Blood tests and tumour marker levels were within normal ranges. Chest computed tomography (CT) revealed a mass of approximately 3.0 cm in the apicoposterior segment of the left upper lobe, accompanied by ground-glass changes around the lesion (Figure 1). On the fourth day of admission, the haemoptysis symptoms worsened. The initial diagnosis was NSCLC. Subsequently, following a comprehensive discussion with the patient and with his explicit consent, he underwent thoracoscopic left upper lobectomy and mediastinal lymph node dissection. The tumour was found to have invaded the cervical pleura and exhibited haemorrhagic characteristics. Considering its proximity to the subclavian vessels, efforts were made to cauterize the bleeding pleura and perform extensive pleural debridement. Pathological examination (Figure 2A) and immunohistochemical staining confirmed the presence of PSC, with positive results for cytokeratin, thyroid transcription factor-1 and vimentin; and negative results for napsin A.
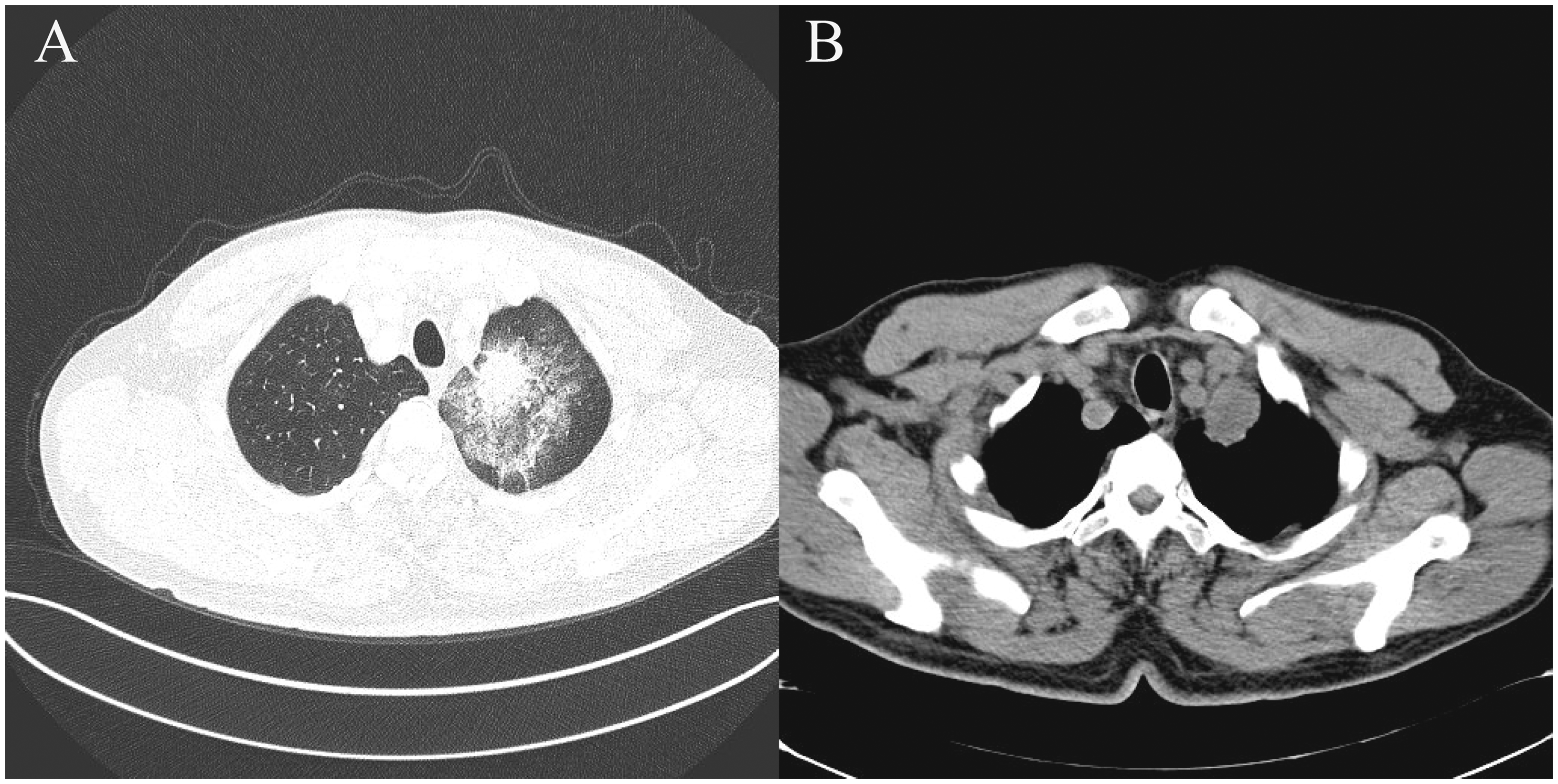
Chest computed tomography scans of a 65-year-old male patient that presented with a 1-month history of productive cough, followed by progressive haemoptysis lasting for 10 days show a 3 cm mass located at the apex of the left upper lung, close to the subclavian vessels. The mass appears to have a surrounding ground glass opacity and shows spiculation and pleural traction signs.
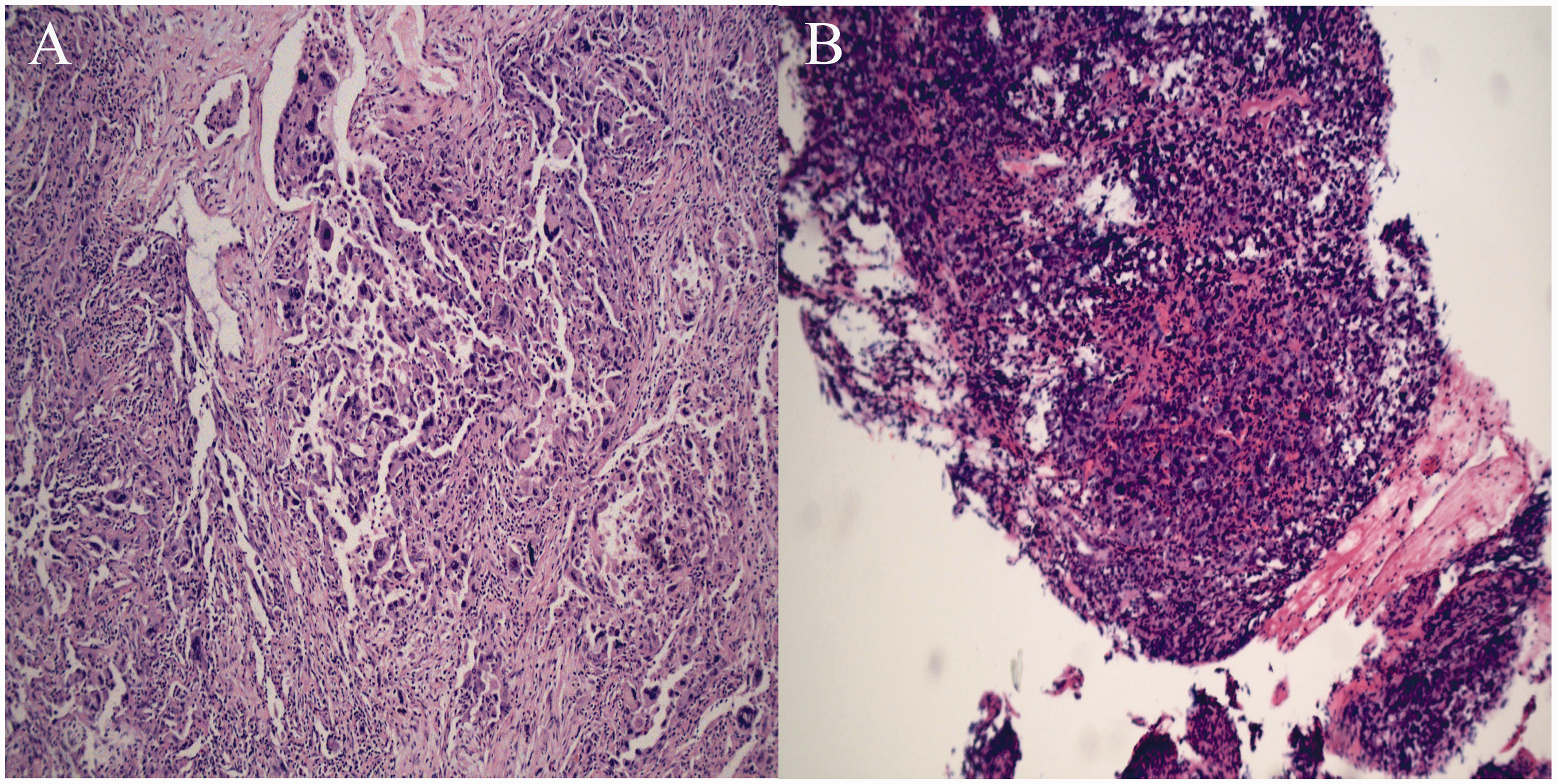
Histopathological examinations of the tissue samples removed from a 65-year-old male patient that presented with a 1-month history of productive cough, followed by progressive haemoptysis lasting for 10 days: (A) haematoxylin-eosin (H&E) staining of the original mass from the apicoposterior segment of the left upper lobe revealed pleomorphic cells with abundant cytoplasm. These cells exhibited a spindle-shaped morphology and displayed significant variation in size and morphology (scale bar 100 µm); (B) histopathological examination of bleeding-prone occupying lesions in the pleural cavity using H&E staining revealed cellular nuclear heterogeneity (scale bar 250 µm). The colour version of this figure is available at: http://imr.sagepub.com.
The patient was discharged without complications. However, when he returned for targeted therapy 1 month after discharge, he complained of recurrent haemoptysis. Chest CT revealed massive pleural effusions on the left side with heterogeneous density (Figure 3) and blood tests showed a haemoglobin level below 70 g/L. A chest tube was promptly inserted, draining more than 2 liters of bloody effusions in a short time. Subsequent emergency surgical exploration revealed the presence of multiple bleeding-prone occupying lesions in the pleural cavity and postoperative pathology confirmed the recurrence of PSC lesions (Figure 2B). Despite various interventions attempted to control bleeding, the patient's clinical condition deteriorated, with new massive haemothorax and severe anaemia, ultimately leading to his death 2 months after hospitalization. All patient details have been de-identified, so a signed patient consent form for publication was unnecessary. The reporting of this study conforms to CARE guidelines. 4

Chest computed tomography scans of a 65-year-old male patient that presented with a 1-month history of productive cough, followed by progressive haemoptysis lasting for 10 days show a large left pleural effusion accompanied by left lung atelectasis. The high density is consistent with the presence of blood clots.
Discussion
Pulmonary sarcomatoid carcinoma is a rare and highly aggressive malignant tumour known for its widespread metastatic potential. 5 Due to the difficulties in preoperative imaging diagnosis to differentiate it from ordinary NSCLC, surgical resection of the nodule or lobectomy is often necessary to obtain an accurate diagnosis. In this particular case, the solitary nodule in the left upper lobe presented challenges in obtaining specific preoperative pathology results through percutaneous pulmonary biopsy. The surgery was successful, but the patient unexpectedly developed refractory haemothorax, leading to his death 3 months after the operation. To the best of our knowledge, this is the first reported case of PSC recurrence presenting as haemothorax.
Pulmonary sarcomatoid carcinoma has a propensity for bleeding and its radiological appearance typically manifests as a peripheral mass with well-defined, rounded margins that exhibit heterogeneity due to necrotic or haemorrhagic areas. 6 As seen in this current case, the imaging findings of a substantial mass with irregular ground-glass opacity surrounding it raise a high suspicion of PSC. Additionally, PSC has the potential to invade the pleura and thoracic wall at an early stage. 7 Therefore, prompt surgical intervention without hesitation is crucial when such manifestations are observed. The primary treatment for early-stage PSC is surgical excision. 8 However, due to the aggressive nature of the tumour, the median survival of patients with PSC has been reported to range from 8 to 19 months, which is inferior to that of ordinary NSCLC.9,10 The efficacy of chemotherapy and radiotherapy in treating PSC remains unclear. Studies have shown that MET gene exon 14 mutations can occur in PSC and overexpression of programmed cell death receptor ligand 1 is observed in more than half of patients.11,12 Therefore, immunotherapy and targeted therapy may represent promising approaches in the treatment of advanced or recurrent PSC. A limitation of this current case report is that the exclusive focus on addressing the clinical issue of refractory haemothorax resulted in a failure to collect epigenetic, biochemical and metabolic data related to the patient.
The occurrence of haemothorax in the presence of malignant disease is indeed a rare and complex medical condition. Also, haemothorax in the presence of lung cancer has limited documentation in the literature. A previous case report described a patient with a spontaneous massive haemothorax that was confirmed postoperatively to be a poorly differentiated sarcomatoid squamous cell carcinoma originating from the right lung with metastases to the pleural wall. 13 The patient was diagnosed with stage IV lung cancer and underwent palliative care before eventually being lost to follow-up. 13 The key finding of their research suggests that haemothorax could potentially serve as a rare clinical indication of advanced-stage lung cancer. 13 Theoretically, en bloc resection of the tumour was expected to significantly reduce the risk of postoperative bleeding. However, the current case presented with an atypical situation where the tumour invaded the pleura of the parietal wall, displaying a notable propensity for haemorrhage. The mechanism underlying refractory haemothorax 1 month after surgery may be attributed to the necrosis of the pleura and tumour or invasion of the subclavian vessels. Various strategies were employed to manage the haemothorax, including re-exploring the chest to control bleeding, extensive pleural debridement, blood transfusions and angiography. Unfortunately, despite our best efforts, these interventions did not successfully reverse the haemothorax. The patient ultimately succumbed to haemorrhagic shock in the third month after the operation, highlighting the severity and complexity of the case.
In conclusion, this current case report underscores the diagnostic challenges associated with PSC and its potential to present with rare and complex clinical manifestations. The difficulty in preoperative diagnosis necessitates the adoption of individualized treatment strategies. Furthermore, the occurrence of haemothorax as a manifestation of advanced lung malignancy highlights the therapeutic complexities in managing tumour-induced refractory haemothorax. This current case underscores the need for further research and exploration in this area to improve diagnostic accuracy and treatment outcomes.
Footnotes
Acknowledgement
We thank all those who contributed to this work.
Author contributions
All the authors have made a substantial contribution to the acquisition, analysis or interpretation of data. All the authors contributed to the writing and revising of the manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research was funded by Changzhou Science & Technology Programme (no. CJ20220165), Young Talent Development Plan of Changzhou Health Commission (no. CZQM2022027) and Changzhou ‘Longcheng Medical Star’ Health Youth Sci & Tech Talent Support Project.