
Abstract
Situs inversus totalis (SIT) is a rare congenital anatomical variation. However, patients with SIT combined with cancer are rare and these patients with two types of lung cancer have not been reported. We report here a case of combined lung adenocarcinoma and solitary fibrous tumor of the pleura with SIT and discuss its clinicopathological features and outcomes. A 68-year-old asymptomatic woman was referred to the Affiliated Hospital of Qingdao University because of an abnormal shadow on chest radiography. Computed tomography showed SIT and an irregularly shaped nodule (measuring 38 × 27 mm in diameter) in the pleural area of the left lower lobe and a 5-mm nodule in the dorsal segment of the lower lobe of the left lung. Surgery was then performed. For such patients, we should eliminate anxiety in patients, perform regular reexaminations, focus on the individual features of these patients, and avoid misdiagnosis because of habitual thinking. At the same time, the lymph nodes should be completely removed and different parts of the tumor with different properties should be treated differently according to the situation.
Keywords
Introduction
Situs inversus totalis (SIT) is a rare congenital anatomical variation, which was first reported by Fabricus in 1600 and first named by Sherk et al. in 1922. 1 SIT manifests as complete mirror image transpositions of the thoracic and abdominal viscera, with an incidence in 1/8000 to 1/25,000 of the normal population. 2 However, the incidence of SIT is not consistent, ranging from 1: 4000 to 1: 60,000.3–5 The first reports of lung cancer with SIT were found in 1952 6 and 1963. 7 Generally, this rare anomaly is discovered or diagnosed incidentally during thoracic and abdominal imaging. Although the exact etiology of SIT remains unknown, SIT is thought to result from chromosomal abnormalities that lead to a reversal of right–left polarity. 8 , 9
There have been no reports on combined lung adenocarcinoma (LUAD) and a solitary fibrous tumor of the pleura (SFTP) with SIT. We report here a case of combined LUAD and SFTP with SIT and discuss its clinicopathological features and outcomes.
Case report
A 68-year-old non-smoking Chinese woman with SIT was referred to our hospital because of an abnormal shadow on chest radiography for 4 days. Chest computed tomography (CT) showed an irregularly shaped nodule (measuring 38 × 27 mm in diameter) in the pleural area of the left lower lobe and SIT (Figure 1a) and a 5-mm nodule in the dorsal segment of the lower lobe of the left lung (Figure 1b). Bronchoscopy confirmed that the left and right bronchial branches were mirror images of each other. Because we were unable to obtain a definitive diagnosis by the bronchoscopic approach, we performed CT-guided percutaneous lung biopsy and surgery was planned for diagnosis and treatment. Intraoperatively, we established that the location of the superior vena cava and azygos vein mirrored the normal distribution, and that the aortic arch was absent from the left thoracic cavity. The left lung was well lobulated into three lobes and the anatomy of the left side of the pulmonary artery had features typical of the normal right side.

Chest computed tomography shows an irregularly shaped nodule (measuring 38 × 27 mm in diameter) in the pleural area of the left lower lobe and situs inversus totalis (a), and a 5-mm nodule in the dorsal segment of the lower lobe of the left lung (b).
On 9 January 2018, the patient underwent thoracoscopic wedge resection of the left lower lobe of the lung plus lymphadenectomy. The tumor was located in the lower left lobe. The location of the lesion in the basal segment was obvious and the interlobar fissure was removed. Wedge resection of the two lesions was performed to remove the lesions and they were sent for rapid pathology. Pathology showed that the tumor in the dorsal segment of the left lower lobe was adenocarcinoma in situ (0.5 cm in diameter) and the mass in the basal segment was a fusiform cell soft tissue tumor with sclerotic, slightly heteromorphic cells. These findings suggested that we should treat the lesions as borderline tumors. Precise diagnosis needed to be performed by immunohistochemistry. The lymph nodes of 11 groups were removed.
Postoperative pathology showed that the tumor in the dorsal segment of the lower left lobe was adenocarcinoma in situ (0.6 × 0.5 cm), without invasion of the local pulmonary capsule and without involvement of the end of the lung. The mass in the basal segment was a solitary fibrous tumor (5.5 × 4×2 cm). Most of the tumor showed collagenous sclerosis, and some areas had abundant cells, active growth, and mitotic cells >4/10 high power fields. There was no clear hemorrhage and necrosis, and atypical and malignant fibrous tissue cells were found. No metastasis was found in the lymph nodes of 11 groups. Immunohistochemical results showed the following: pan-cytokeratin (−), vimentin (+), synaptophsin (−), CD56 (−), CD34 (+), CD99 (+), S100 (−), desmin (−), smooth muscle actin (−), and Ki-67 (+) 10% (Figure 2).
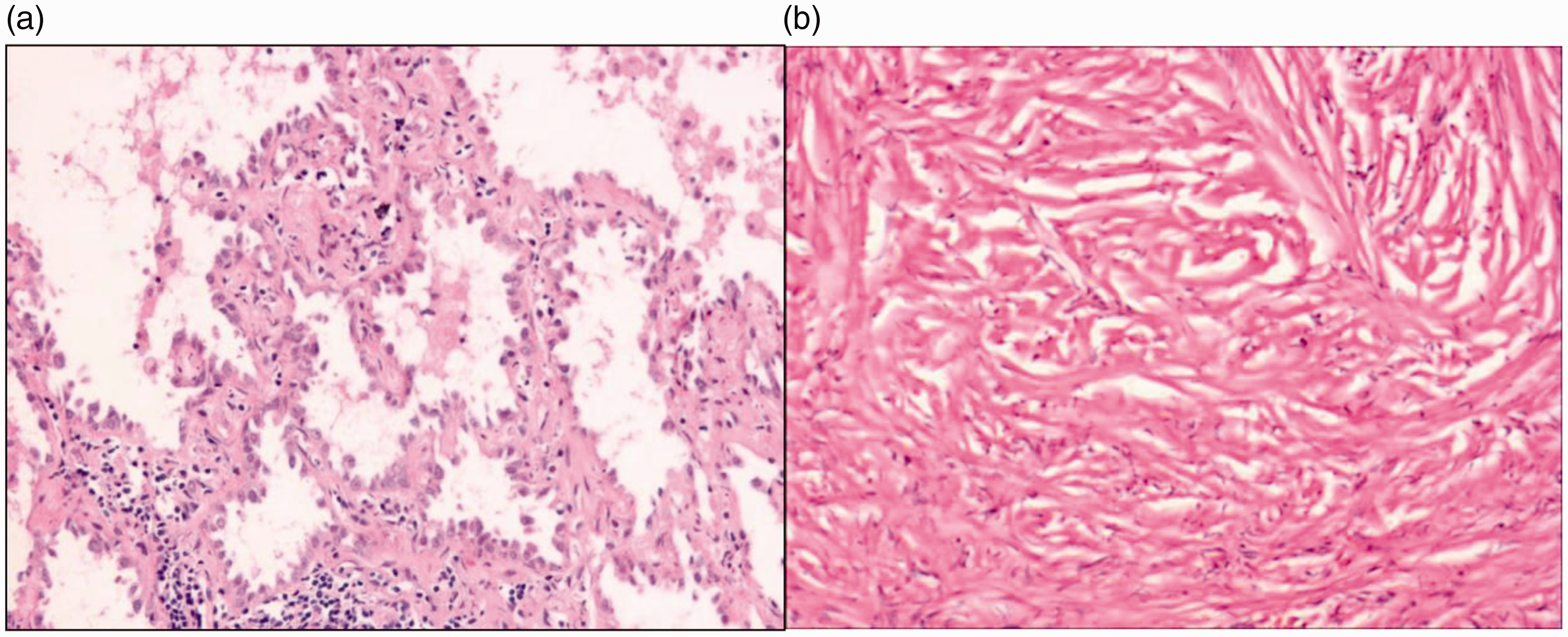
Hematoxylin and eosin staining. The tumor in the dorsal segment of the lower left lobe is adenocarcinoma in situ (0.6 × 0.5 cm) (a) and the mass in the basal segment is a solitary fibrous tumor (5.5 × 4×2 cm) (b). Magnification, ×200.
Discussion
To the best of our knowledge, we report the first case of coexistence of two types of tumors and SIT, which were surgically treated in China, and also the first patient to be reported in PubMed with two types of tumors from different sources. A previous report showed that a patient with SIT had the same tumor in two locations of the lung. 10
In multiple primary lung cancer (MPLC), Beyreuther 11 reported the first definite case of double primary lung cancer in 1924, and more cases of multiple primary lung cancer have since been found. Our patients had the combination of adenocarcinoma and a solid fibrous tumor, which is in accordance with the diagnostic criteria of MPLC. At present, the 5-year survival rate of MPLC is 12.5% to 27.1%, 12 , 13 which is better than that of lung metastasis. Riquet et al. 12 believed that when the histological type of multiple primary tumors is cancer, the prognosis is not conducive to the occurrence of MPLC, which may be more serious than lung metastasis of squamous cell carcinoma and adenocarcinoma.
SIT is a rare genetic abnormality. The first report of a patient with SIT and lung cancer was in 1952, 14 and in 1990, the first lung cancer surgery was performed in patients with SIT. 4 SIT is characterized by mirror images of the normal position of organs. However, the altered position of the organs may lead to difficulty in diagnosis and orientation and dissection during surgery. This increases the operative difficulty, thus increasing the risk of iatrogenic injures and the operative time. 15 , 16
There have been 28 cases of SIT and lung cancer reported in the literature.3–7, 10 ,16–22 There were 24 men and 4 women. The mean age of the patients was 65.1 ± 9.3 years. Six (6/21.4%) of the patients presented with Kartagener syndrome. There were 16 left and 12 right lung cancer cases. Many (28%–32.1%) of these patients were diagnosed with adenocarcinoma, with a similar rate to that in the general population.
Twenty cases of SIT cases were operated on, with 8 on the right and 12 on the left. Upper lobectomy was performed in four cases, lower lobectomy in three cases, and thoracotomy in one case. There were three cases of pulmonary resection, five cases of upper lobectomy, two cases of lower lobectomy, one case of lower lobectomy, and one case of middle lobectomy. One patient underwent right laparoscopic adrenalectomy. Eight patients did not have an operation. Five patients received adjuvant treatment, four patients received symptomatic treatment, and treatment was unknown in one patient. The patients’ characteristic are shown in Table 1. Correct preoperative evaluation ensures the safety of the operation. 19 In an abdominal emergency operation, understanding the anatomical abnormality is important to prevent complications of the operation, and appendectomy and cholecystectomy should be correctly chosen. 19 All patients with lung cancer/SIT were treated selectively and with appropriate preoperative diagnosis. The left side was a radical operation and the right side was exploratory thoracotomy. In all cases, the lungs and mediastinum had contralateral anatomical features in the description of the surgical field. The lungs also showed typical changes in the interlobar fissure, bronchial tree, and pulmonary vessels. Ten cases of thoracotomy and five cases of video-assisted thoracic surgery were performed.
Characteristics of patients with SIT and lung cancer.

M, male; F, female; Kartagener S, Kartagener syndrome + SIT; SIT, situs inversus totalis; SCLC, small cell lung cancer; NSCLC, non-small cell lung cancer; NSCLC(s), squamous cell carcinoma; NSCLC(a), adenocarcinoma; NSCLC(l), large cell carcinoma; NSCLC(as), adenosquamous cell carcinoma; NSCLC(le), lymphoepithelioma-like carcinoma.
In all cases of SIT and lung cancer, the lungs and the mediastinum had anatomical features of the opposite side in the description of the operative field. Because of technical conditions, left pneumonectomy was performed and no other vessel anomalies were described. 19 SIT is more common in Japan and Eastern Europe, and its symptoms and clinical course are similar to other lung cancers. The most difficult cases to diagnose and treat are patients with lung cancer/Kartagener syndrome because this disease can have the form of recurrent bronchitis and hemoptysis. 3 There is little experience of treatment in the 28 patients with lung cancer/SIT, although the symptoms and the clinical course of this disease are similar to other lung cancer cases. The majority of these patients were men (24/28% to 85.7%), although in previous reports of SIT only, 19 the occurrence of this disease was equally distributed across the sexes.
Conclusions
The association between SIT and malignant tumors is controversial. Because of the limitation of the number of cases and other objective aspects, this relationship requires further clinical and epidemiological studies. For such patients, we should eliminate tension of patients, perform regular reexaminations, focus on the individual features of these patients, and avoid misdiagnosis of habitual thinking. Additionally, the lymph nodes need to be thoroughly removed and different parts of the tumor with different properties should be treated differently according to the situation.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics
The study protocol conformed to the ethical guidelines of the 1975 declaration of Helsinki and was approved by the ethics committee of the Qingdao Haici Medical Treatment Group (Qingdao, China). The patient provided written informed consent for publication of this report and accompanying images.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.