
Abstract
Spontaneous unilateral quadriceps tendon rupture is an uncommon injury that is generally associated with chronic kidney disease and metabolic disorders. The current case involved a 50-year-old man with a painful right knee that he was unable to extend as a result of minor trauma sustained in an accident. Physical examination combined with radiographic and ultrasonographic investigations led to a diagnosis of quadriceps tendon rupture of the right knee. The patient had a 7-year history of hemodialysis for treatment of chronic kidney disease, leading to secondary hyperparathyroidism. He underwent successful tendon repair surgery, and his right knee was immobilized with splints for 6 weeks postoperatively. He gradually resumed full weight bearing and then normal walking.
Introduction
Quadriceps tendon rupture is a rare orthopedic injury that most often occurs secondary to traffic accidents among people aged <40 years. 1 Spontaneous tendon rupture, however, is relatively uncommon, 2 and the exact mechanism remains controversial. 3 Risk factors for spontaneous quadriceps tendon rupture include metabolic disorders and predisposing medical conditions such as diabetes, gout, hyperparathyroidism, 4 severe vitamin D deficiency, 5 and chronic kidney disease 6 as well as other unknown factors. Early and systemic treatment of a ruptured tendon may achieve satisfactory results. We herein report a case of spontaneous rupture of the right quadriceps tendon in a patient with hyperparathyroidism secondary to 7 years of hemodialysis.
Case presentation
A 50-year-old man with kidney disease due to chronic glomerulonephritis presented with pain and the inability to extend his right knee following a minor trauma caused by sudden braking while he rode an electric bicycle at an extremely slow speed. The patient had been undergoing hemodialysis at our hospital for the previous 7 years because of uremia; his Kt/V value was 1.2 and his urea reduction ratio was 65%. He was 175 cm tall and weighed 65 kg. The patient had no history of smoking, drinking, hypertension, diabetes, or gout.
Physical examination demonstrated a palpable defect in the right quadriceps tendon, the complete loss of active extension of the right knee, and a lower right than left patella. Radiographic examination of the right knee showed inferior displacement of the right patella with calcified deposits in the quadriceps tendon (Figure 1(a)). Ultrasonic examination was used to observe the appearance of the overlying tendon and muscle (Figure 1(b)). Complete rupture of the right quadriceps tendon at the patellar insertion was confirmed. Laboratory examination revealed a creatinine concentration of 980 µmol/L (reference range, 40–120 µmol/L), serum parathyroid hormone (PTH) concentration of 2080.6 pg/mL (reference range, 12–88 pg/mL), serum calcium concentration of 2.74 mmol/L (reference range, 2–2.7 mmol/L), serum phosphorus concentration of 2.13 mmol/L (reference range, 0.85–1.5 mmol/L), alkaline phosphatase (ALP) concentration of 261 IU/L (reference range, 45–125 IU/L), 25-OH vitamin D concentration of 46 ng/mL (reference range, 20–70 ng/mL), and serum glucose concentration of 5.42 mmol/L (reference range, 3.8–6.1 mmol/L). Diagnoses of spontaneous rupture of the right quadriceps and secondary hyperparathyroidism were made. Surgical repair was performed through a 9-cm longitudinal midline incision. A complete rupture above the patella was observed with no residual tendon tissue attached to the smooth surface of the patella (Figure 1(c)). The rupture extended to the quadriceps muscle, which had an insufficient blood supply, and the color of the tissue stump was dark brown with signs of calcification and chronic inflammatory infiltration. Ultrasonic examination of right knee 10 days postoperatively showed that the repaired tendon was continuous with the superior pole of the patella (Figure 1(d)). Pathological examination of the tendon tissue was performed (Figure 2). Postoperatively, the patient’s right knee was immobilized for 6 weeks, followed by physiotherapy. Eight weeks after surgery, the patient gradually resumed full weight bearing and then normal walking.
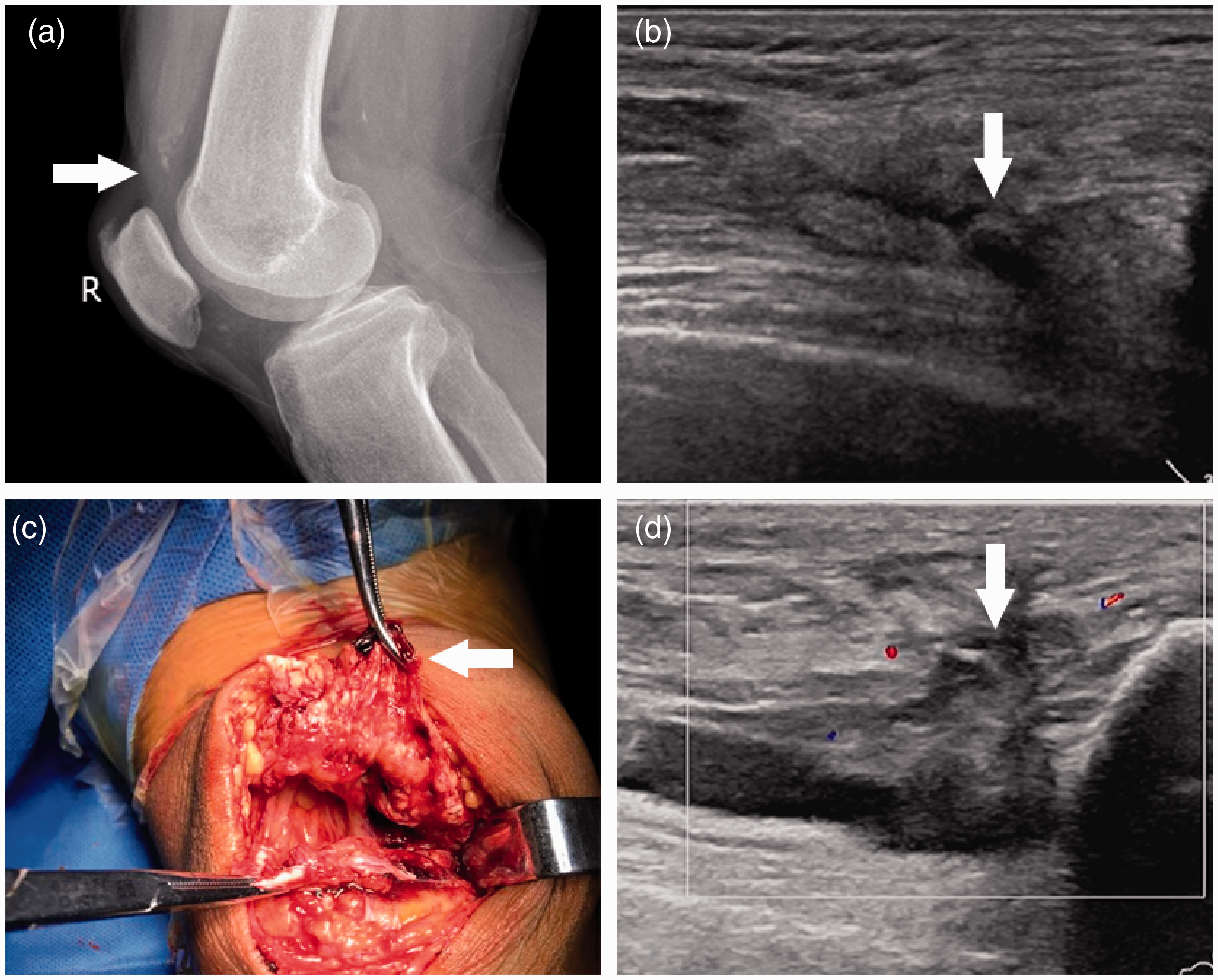
(a) Radiographs of the right knee showed downward displacement of the right patella with calcified deposits in the quadriceps tendon (white arrow). (b) Ultrasound examination showed the rupture of the quadriceps tendon as indicated by the arrows. (c) Intraoperatively, complete rupture between the quadriceps tendon and patella was identified; the color of the tissue stump was dark brown and it had a poor blood supply (white arrow). (d) Ultrasound examination showed that the repaired tendon was continuous with the superior pole of the patella (white arrow).

Pathological examination of the ruptured quadriceps tendon. Hematoxylin–eosin staining showed (a) vascular proliferation (star), calcification (triangle), a bone fragment (arrow) (×100), and (b) inflammatory cell infiltration (arrow) (×200).
Discussion
Secondary hyperparathyroidism in patients with chronic kidney disease reportedly plays a major role in the pathogenesis of spontaneous tendon rupture. 4 However, the pathologic characteristics of the ruptured tendon have not been investigated. The present report describes the first pathological examination of a ruptured quadriceps tendon. Hematoxylin–eosin staining revealed signs of vascular proliferation, calcification, bone fragments, and inflammatory cell infiltration. The calcification observed was consistent with the results of the imaging and intraoperative exploration. The patient described herein had high serum calcium, phosphorus, PTH, and ALP concentrations, which are common complications in patients with chronic kidney disease undergoing long-term dialysis. 7 Elevated serum PTH and ALP levels lead to subtendinous bone resorption at the sites of insertion through increased bone turnover. In addition, the high PTH acts as a toxin that contributes to tendon degeneration and chronic inflammation, diminishing the blood supply of the tendon and leading to thrombosis of the microcirculation. The blood supply to the tendon is the most important factor in the pathogenesis of major tendon rupture. 8 The malnutrition of the tendon causes secondary microvascular hyperplasia as well as increased brittleness and reduced elasticity of the tendon. Moreover, the high calcium phosphate product results in dystrophic calcification of the tendon, which further weakens the osseotendinous junction between the quadriceps tendon and patella. Thus, the tendon sustains minor avulsion fractures of the bone cortex at the tendon insertion site and eventually ruptures after microtrauma. Therefore, for patients with secondary hyperparathyroidism undergoing hemodialysis, strict systematic treatment measures for hyperparathyroidism are needed to prevent further spontaneous tendon rupture.
Some scholars have noted that total parathyroidectomy (with or without autotransplantation of part of the parathyroid gland in recalcitrant cases), early use of vitamin D analogs, phosphate binders, and calcimimetics are recommended to prevent future tendon rupture. 9
Conclusions
The present report reveals the pathological mechanisms involved in spontaneous rupture of the quadriceps tendon in patients with chronic renal disease. Although the widespread use of dialysis improves the quality of life and extends the life expectancy for patients with chronic kidney disease, the subsequent incidence of quadriceps tendon rupture is non-negligible. For patients undergoing long-term hemodialysis, strict and systematic management of mineral and bone disorders is required to prevent rupture or re-rupture of the quadriceps tendon. Injury prevention during daily activities is also important for patients undergoing hemodialysis.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
This study was approved by the medical ethics committee of Fujian Provincial 2nd People’s Hospital. Written informed consent was obtained from the patient for the publication of this case report.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.