
Abstract
Simultaneous bilateral quadriceps tendon rupture is a rare injury that represents < 5% of all quadriceps tendon ruptures. It is generally associated with chronic metabolic disorders and is seen in patients with uraemia undergoing maintenance haemodialysis. The present case was a 46-year-old man who presented with pain and the inability to extend his knees following a minor accident. A physical examination combined with X-radiography and magnetic resonance imaging investigations resulted in a diagnosis of bilateral quadriceps tendon rupture. He had a history of uraemia and had received regular haemodialysis for 7 years. He had high levels of serum parathyroid hormone and he was diagnosed with secondary hyperparathyroidism. Following surgical repair of both quadriceps tendons, in addition to management of the secondary hyperparathyroidism, the patient regained full active mobility of both knee joints and was able to participate in normal activities of daily living.
Introduction
Cases of simultaneous bilateral quadriceps rupture in patients with chronic renal failure have been described in the literature.1–4 Although the exact mechanism remains unclear, most investigators agree that secondary hyperparathyroidism due to repeated dialysis treatment plays a major role in the pathogenesis of tendon rupture.2–4 Early treatment of ruptured tendons results in better outcomes than delayed treatment.5–8 This current report presents a case of bilateral spontaneous rupture of the quadriceps tendon in a patient with secondary hyperparathyroidism, undergoing long-term haemodialysis.
Case report
Approval for the publication of this case report was obtained from the Ethics Committee, First Affiliated Hospital of Soochow University, Suzhou, Jiangsu Province, China. Written informed consent was obtained from the patient.
A 46-year-old man presented to the Department of Orthopaedic Surgery, First Affiliated Hospital of Soochow University in May 2010, with pain and the inability to extend his knees. The injury had occurred when he applied the brakes suddenly while riding an electric bicycle at a very slow speed. The patient had been undergoing haemodialysis at the First Affiliated Hospital of Soochow University for the previous 7 years, due to uraemia.
A physical examination revealed substantially swollen thighs in the region of the injury on both legs and palpable soft tissue depression above the patellae, which was exaggerated with active contraction of the quadriceps muscles. Moreover, the patellae could be moved freely over a wider range than normal and the deep surface of each patella was easily felt (Figure 1). The remainder of his physical examination was normal.
Physical examination of a 46-year-old man who presented with pain and the inability to extend his knees following a minor accident. He had substantially swollen thighs in the region of the injury. Palpable soft tissue depression above each patella was observed, which was exaggerated with active contraction of the quadriceps muscles. Both patellae could be moved freely over a wider range than normal and the deep surface of each patella was easily felt.
An X-radiography examination of his knees demonstrated downward displacement of the patellae, with calcified deposits in the quadriceps tendon (Figure 2). Both patellae were tilted forwards with no evidence of fracture. Magnetic resonance imaging (MRI) showed that the continuity of the quadriceps tendons was avulsed from the superior pole of the patellae (Figure 3). The serum parathyroid hormone (PTH) level was 984 pg/ml (normal range 15.0–65.0 pg/ml). A diagnosis of bilateral quadriceps tendon rupture and secondary hyperparathyroidism was made.
Lateral X-radiography examination (both knees) in a 46-year-old man who presented with pain and the inability to extend his knees following a minor accident. Downward displacement of both patellae is shown, with calcified deposits in the quadriceps tendons (arrows). Both patellae were tilted forwards with no evidence of fracture. Lateral T2-weighted magnetic resonance images of the knees of a 46-year-old man who presented with pain and the inability to extend his knees following a minor accident. Images showed that the continuity of the quadriceps tendons was avulsed from the superior pole of the patellae (arrows).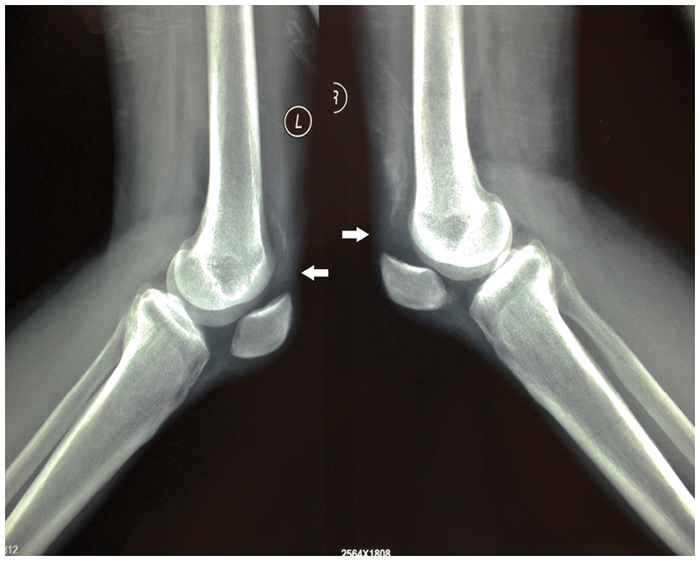

The patient underwent an operation on 11 May 2010. In the operating room, he was placed in the supine position and a tourniquet was inflated to 300 mmHg. Each leg underwent the same surgical procedure. A longitudinal incision was made ∼7 cm overlying the quadriceps tendon and proximal patella of each knee. Sharp dissection exposed the ruptured quadriceps tendon. Complete rupture above the patella was observed, the rupture extended to the quadriceps muscle and the colour of the tissue stump was dark brown; it had a poor blood supply and there were signs of chronic inflammatory infiltration. No residual tendon tissue was attached to the smooth surface of the patella (Figure 4).
Surgery was undertaken on both knees of a 46-year-old man who presented with pain and the inability to extend his knees following a minor accident. Complete rupture of the quadriceps tendon above the patella was observed following dissection of each knee. The rupture extended to the quadriceps muscle and the colour of the tissue stump was dark brown; it had a poor blood supply and there was evidence of chronic inflammatory infiltration. No residual tendon tissue was attached to the smooth surface of the patella.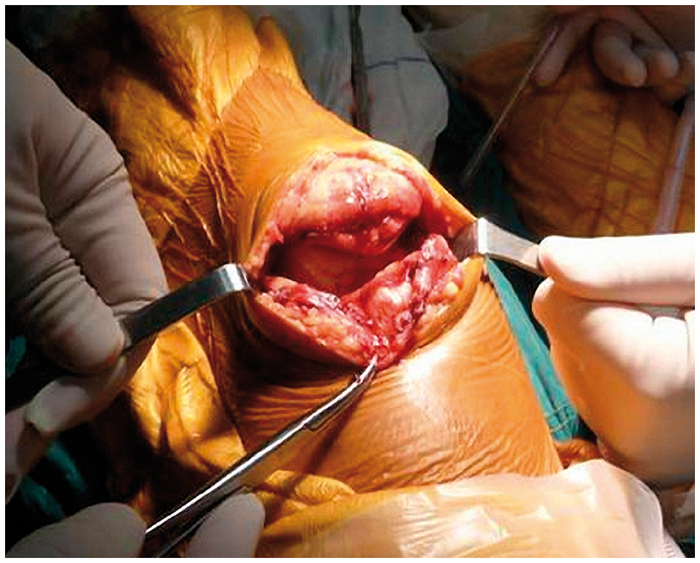
After removing part of the inactivate quadriceps tendon, the upper pole of the patella was roughened using a spherical burr. Two anchors were implanted into the patella after drilling, and two pairs of heavy, nonabsorbable sutures were placed through the quadriceps tendon, using the same technique used for Bunnel’s suture. The knee could be flexed up to 120° intraoperatively without causing tension to the sutured tendon. During this procedure, a wire was placed around the patella and quadriceps tendon to reduce tension.
Following a 4-week immobilization period for the extended knees, continuous passive movement was applied and assistive physiotherapy was used, to exercise the extensor mechanism and improve the range of movement using < 60° of flexion. At 8 weeks after surgery, the patient presented with joint activity of 0–130°. At the 12-month follow-up visit, the patient had regained full active mobility of both knee joints and was able to participate in normal activities of daily living (Figure 5).
Following corrective surgery to the quadriceps tendons of both knee joints and rehabilitation therapy, a 46-year-old man who had presented with pain and the inability to extend his knees following a minor accident regained full active mobility of both knee joints, which was evident at a 12-month follow-up visit.
Discussion
Quadriceps tendon rupture is an uncommon injury, whereas patella fracture and patella tendon rupture are common causes of a disrupted extensor mechanism. 7 Simultaneous bilateral quadriceps tendon rupture is extremely rare and represents < 5% of all cases. 6 Quadriceps tendon rupture often occurs in older patients, especially men. 5 Weakening of the quadriceps tendon may predispose the patient to rupture, as can uraemia, rheumatoid arthritis, diabetes mellitus, nephritis, gout, autoimmune inflammatory diseases, tumours and the prolonged use of systemic steroid therapy. 1 Furthermore, cases of quadriceps rupture after total knee arthroplasty have been reported. 9
In 1949, Steiner and Palmer 1 reported the first case of simultaneous bilateral quadriceps tendon rupture in a patient with chronic renal failure. Other cases of simultaneous bilateral quadriceps rupture in patients with chronic renal failure have been reported subsequently.2–4 Although the exact mechanism of injury remains unknown, most investigators agree that secondary hyperparathyroidism due to repeated dialysis treatment plays a major role in the pathogenesis of tendon rupture.2,3 In this current case of a patient with uraemia, there was evidence during surgery that the quadriceps tendon was inflamed, and was therefore weak. In such situations, tendon rupture can be induced by minor or major trauma or it can even arise spontaneously.
In the present case, the key component of the diagnosis was the physical examination, which revealed that both patellae could be moved freely over a wider range than normal; in addition, the deep surface of each patellae could be easily felt. However, cases reported in the literature have shown that up to 50% of bilateral quadriceps tendon rupture may be misdiagnosed, 5 which might cause the affected patients to disengage from clinical treatment. It is important to consider the possibility of a quadriceps tendon rupture in any patient who presents with acute knee pain, an inability to extend the leg, or a palpable soft-tissue depression proximal to the superior pole of the patella, particularly if the patient has a history of chronic disease. MRI of both thighs may be helpful when the diagnosis remains unclear.
In the typical patient with an acute and complete quadriceps tendon rupture, surgical repair is recommended to restore function. Studies suggest that early (within 2 weeks) surgical treatment and subsequent functional exercise can lead to satisfactory results.5–8 The insertion of sutures through the quadriceps tendon (via drilled holes into the superior border of the patella) is the most common method used to repair quadriceps tendon rupture. 9 In addition to the growing popularity of suture anchor fixation in other types of orthopaedic surgery,10,11 a suture anchor is also being used for the treatment of quadriceps tendon rupture because it is a strong and effective technique. 9 During surgery for this current case, a suture anchor was used to fix the bone and tendon, with two anchors being implanted in the patella and two pairs of nonabsorbable sutures being placed through the quadriceps tendon. This approach was achieved using Bunnel’s suture technique with a wire wrapped around the patella and quadriceps tendon to reduce tension. Then the knee joints were immobilized in a cast for 4 weeks. Thereafter, the patient underwent physiotherapy to improve his range of movement.
Secondary hyperparathyroidism is frequently referred to as renal hyperparathyroidism. Estimates report that as many as 90% of patients with chronic renal failure develop hyperparathyroidism by the time haemodialysis is initiated. 12 The treatment of secondary hyperparathyroidism is predominantly medical, using newer calcimimetics, phosphate binders and vitamin D analogues. The surgical management of secondary and tertiary hyperparathyroidism is has a favourable good safety and efficacy profile. 12
In conclusion, bilateral quadriceps tendon ruptures are uncommon injuries that require early surgical treatment and subsequent functional exercise, in order to maximize functional outcomes for the patient. For patients with uraemia resulting in secondary hyperparathyroidism, the systematic treatment of secondary hyperparathyroidism is effective at correcting tendon mineralization and metabolic disturbances.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.