
Abstract
Parathyroid carcinoma is a rare malignancy; and it is rarer to find one located in an ectopic location. Ectopic parathyroid glands are a reported cause of failed primary surgery for hyperparathyroidism. We report here a 73-year-old male who previously had parathyroidectomy for primary hyperparathyroidism but then had recurrence of his symptoms with a diagnosis of a mediastinal parathyroid carcinoma on further evaluation. This presentation of complicated mediastinal parathyroid carcinoma posed significant diagnostic and management challenges due to comorbid stage IV chronic kidney disease (CKD). Secondly, due to the same comorbid condition, a more aggressive calcimimetic regimen could not be undertaken due to the risk of renal dysfunction with potential progression to dialysis status. Thirdly, he was a high-risk surgical candidate due to significant cardiovascular risks. Ideally, open surgical intervention would be recommended but due to the associated risks, he was managed with robotic-assisted thoracoscopic surgery. He subsequently developed hypocalcemia which normalized with supplemental calcium at follow-up.
Keywords
Introduction
Parathyroid carcinoma (PC) is extremely rare, with a reported prevalence of 0.005% of all tumors. It accounts for 1%–5% of all cases of primary hyperparathyroidism. 1 Ectopic parathyroid glands localized to the mediastinum are even rarer and have similar pathophysiologic presentation as parathyroid adenomas (PA), making diagnosis arduous. PCs commonly occur in adults in their fifth decade, regardless of gender. Favorable prognosis significantly correlates with young age, female sex, recent diagnosis, and absence of distant metastases. 2 Despite advancements in diagnostic modalities, diagnosis can be elusive, and distinguishing benign from malignant parathyroid diseases can be challenging (Figure 1). 3

A graphical abstract of this case report.
Case description
A 73-year-old man had primary hyperparathyroidism diagnosed the previous year and underwent subtotal parathyroidectomy with reimplantation to the right arm, and he currently has stage IV chronic kidney disease with secondary hyperparathyroidism. He presented to the emergency department with complaints of nervousness, fatigue, and generalized weakness of 2 weeks duration. At baseline, he was independent with activities of daily living but had started having difficulty carrying out his activities of daily living due to weakness. He also had polyuria, polydipsia, and bone pain. Review of systems was otherwise unremarkable. Patient was receiving cinacalcet. At presentation, he was awake and alert, his vital signs were stable with a pulse of 66 beats per minute and blood pressure of 143/68 mmHg, and he had a right forearm arteriovenous fistula with thrill and a strength of 3/5 in all extremities.
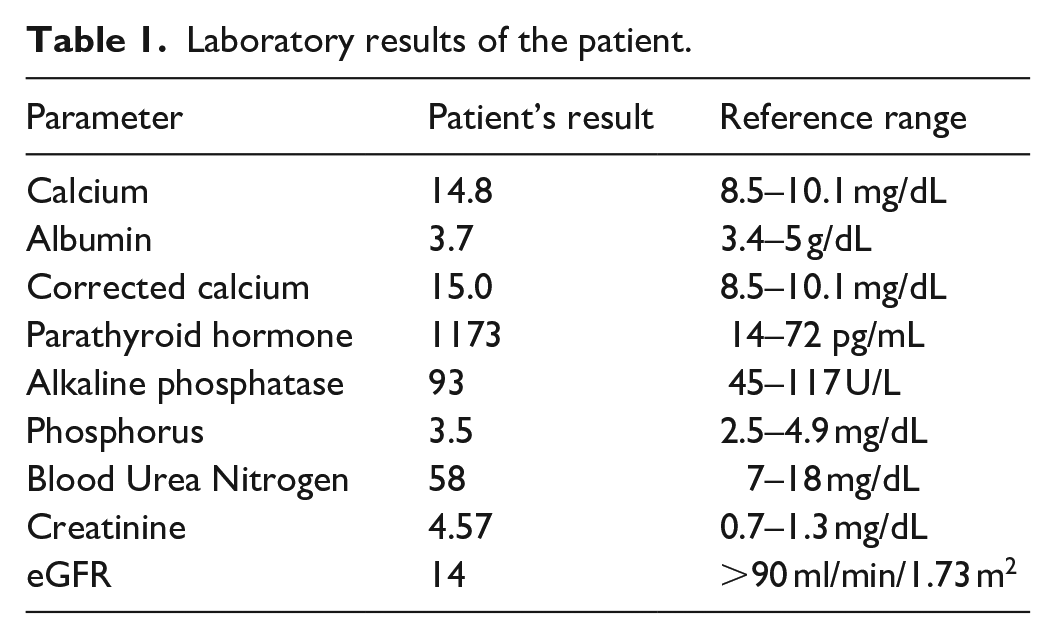
Initial work-up revealed normocytic anemia, elevated urea/creatinine, hyponatremia, severe hypercalcemia, normal 25-Hydroxy-Vitamin D, and elevated Parathyroid Hormone (Table 1). He was admitted to the medical unit for management of hypercalcemic crisis thought to be due to primary hyperparathyroidism. Given that he underwent total parathyroidectomy with gland reimplantation, this was suspected to be the source. An ultrasound imaging obtained did not reveal viable glandular tissue. On further evaluation, neck/thyroid ultrasound revealed no suspicious nodules or parathyroid abnormalities. Nuclear medicine/sestamibi parathyroid scan revealed an uptake in the mediastinum indicative of parathyroid activity, possibly an adenoma. For preoperative planning, a non-contrast chest Computed Tomography was obtained (due to risk of nephrotoxicity), revealing 4.1 × 1.9 cm soft tissue density in the anterior aspect of superior mediastinum (Figures 2–4).
Laboratory results of the patient.
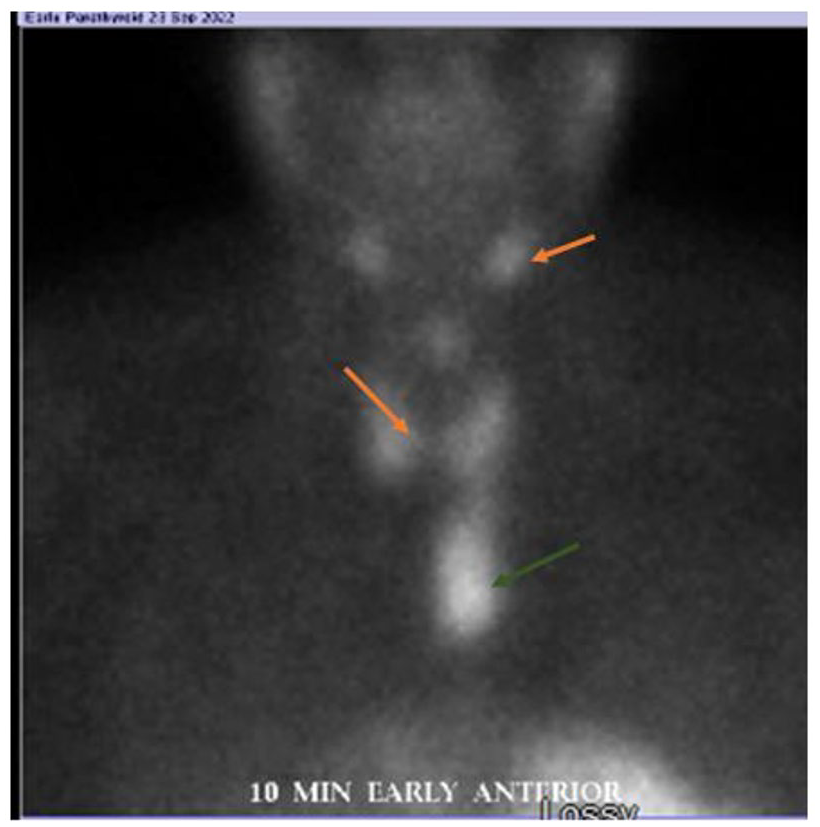
Parathyroid scan showing increased uptake in the mediastinum.

Parathyroid scan showing persistent increased oblong uptake in the mediastinum even in the late phase.

Non-contrast chest CT showing a 4.1 × 1.9 cm soft tissue density in the anterior aspect of the superior mediastinum.
He was managed with cautious intravenous volume expansion with isotonic fluids to avoid volume overload in the setting of Chronic Kidney Disease, calcitonin for 48-h, Cinacalcet, and low-dose pamidronate (30 mg given over 4 h) given CrCl < 30. He underwent left chest robotic partial thymectomy with mobilization of the anterior mediastinal mass. However, there was no significant decrease in PTH or ionized calcium levels intraoperatively. Therefore, a redo neck exploration with completion total parathyroidectomy was done, consistent with the sestamibi scan which showed enhancement at the base of the neck, above the innominate vein. PTH levels dropped from over 500 preoperatively to 250 intraoperatively. A 5.3 × 2.7 × 2.0 cm and 0.19 × 0.8 × 0.5 cm nodular tan masses were excised. Intraoperative frozen section was positive for tumor, so reimplantation was not done. Histopathology revealed the masses were positive for chromogranin, GATA3, and PTH but negative for synaptophysin, TTF-1, and thyroglobulin on immunohistochemistry. Ki-67 proliferation index was 10%. There was broad fibrous bands and vascular invasion, confirming the diagnosis of PC (Figures 5 and 6). Unfortunately, pathology could not comment on margins. Post-surgery hypocalcemia was treated with calcium carbonate, Vitamin D, and calcitriol with normalization of calcium levels. He was discharged on hospital day 23, 10 days post-surgery due to challenges with insurance approval for post-acute placement. The patient was seen 1 month post-hospitalization with normalization of serum calcium while on calcium carbonate and resolution of symptoms.

Pathology of resected mass showing lymphovascular invasion.

Pathology of resected mass showing irregular fibrous bands.
Discussion
Genetics and environmental factors contribute to the development of PC. 4 Disease incidence and prevalence are typically expressed as the percentage of primary hyperparathyroidism cases given the rarity of its occurrence. 3 (1) In the United States, the incidence is reported at <1% based on large case series from the National Cancer Data Base and reports from Japanese cohorts are as high as 5%. 5 Several genetic associations have been proposed, including the MEN1 and 2A syndromes, however, most evidence supports its association with hereditary hyperparathyroidism-jaw tumor syndrome.6,7 An ectopic parathyroid gland is not uncommon due to the embryonic development of the parathyroid gland from the third pharyngeal pouch; however, ectopic locations do not confer a higher risk of malignancy.3,8
Diagnosis of PC can be challenging in that it shares clinical, radiological, and histological characteristics with PA. Despite these similarities certain indicators may suggest the possibility of parathyroid cancer. Most parathyroid cancers are functional tumors, in which patients usually experience signs and symptoms of hypercalcemia presenting with fatigue, malaise, weakness, weight loss, and anorexia at the time of initial clinical evaluation. The humoral symptoms often manifest prior to the clinical effects of local tumor invasion. Clinical features that suggest a diagnosis of PC include age less than 50 years; markedly elevated PTH and calcium levels (usually >14mgdL), severe bone pain and lesions, and recurrent laryngeal nerve palsy from tumor invasion. 9 Most complications involve the skeletal and renal systems, although pancreatitis and hypercalcemic crisis may occur. 9 The Schulte 3 + 3 rule was initially developed for cervical PC, but it has been applied to mediastinal PC with 100% specificity and positive predictive value in ruling out malignancy. 10 In a large cohort of individuals with primary hyperparathyroidism, lesions below 3 cm and with calcium-corrected blood levels below 3.0 mM had an essentially zero risk of cancer; lesions that met both criteria had a malignancy risk of 5%–10%. 10
Cervical ultrasound and 99 mTc-sestamibi scan are initial imaging of choice to localize the lesion.11,12 The role of fluorodeoxyglucose-positron emission tomography for diagnosis is limited, as lytic bone lesions exhibit a significant propensity for fluorodeoxyglucose uptake and may be erroneously identified as bone metastasis. 13 Sophisticated imaging techniques, including CT and MRI scans augmented with contrasts, represent a highly advantageous tool for precisely identifying the location of tumors, detecting tissue or lymph node infiltration, and assisting with preoperative planning. 14 Hybrid imaging combining MIBI scintigraphy with CT or MRI, like in this case, yields better results. 14 In patients with advanced chronic kidney disease (eGFR <30 mL/min/1.73), akin to the patient in this case, there is hesitation to pursue these imaging due to the risk of iodinated contrast induced kidney injury and nephrogenic systemic fibrosis associated with gadolinium exposure15,16 (Figure 6). However, sestamibi is reliable in making this diagnosis. In this case, nuclear sestamibi was able to delineate the mediastinal mass but was limited in providing information regarding the extent of tissue invasion. In cases where contrasted CT is absolutely required for preoperative evaluation, these patients should undergo prophylactic hydration with intravenous isotonic fluid. 17
Prompt management of hypercalcemic crisis necessitates intravenous normal saline infusion for volume expansion and the administration of loop diuretics to facilitate renal calcium excretion. Bone mass preservation is achieved with intravenous bisphosphonates. Cinacalcet, a calcimimetic, was studied in a case series of 29 patients with inoperable metastatic PC. Two-thirds of the patients had treatment response shown as average serum calcium reduction but no effect on PTH. It has not been shown to alter the course of parathyroid cancer but may alleviate clinical effects of hypercalcemia. 18 It is unclear if cinacalcet has benefit in individuals with renal disease and inoperable MPC. CKD patients require careful monitoring and modification of therapy in hypercalcemic crisis with bisphosphonates contraindicated in advanced renal dysfunction. En-bloc surgical resection with clear margins is the most effective treatment for MPC. 19 To achieve success, high-resolution imaging and preoperative planning are crucial to locating the parathyroid tumor accurately. 14 This case posed diagnostic and management difficulties due to coexisting stage IV chronic kidney disease. Additionally, CKD status precluded the implementation of a more intensive calcimimetic therapy, as it carried a risk of renal impairment and potential advancement to dialysis. Moreover, he was a poor surgical candidate due to age, frailty, and notable cardiovascular comorbid factors. Therefore, robotic-assisted thoracoscopic surgery was utilized to avoid risks associated with open surgical intervention. In addition, there have been reports of improved outcomes with robotic approach and our center commonly perform this procedure.20,21
It is not unlikely for patients treated for parathyroid adenoma to present with subsequent carcinoma. In fact, the ectopic glandular tissue may go undetected, during initial presentation leading to the unnecessary removal of the cervical parathyroid glands. 22 Individuals with prior parathyroid tumors should undergo routine surveillance follow up after initial management. In those with clinical findings suggestive of hyperparathyroidism in the absence of parathyroid mass on physical and radiological examination, ectopic parathyroid cancer must be considered, and appropriate localization imaging studies pursued. Multispecialty management involving endocrinologists, internists, and cardiothoracic surgeons is essential for optimal outcome.
Conclusion
This case highlights ectopic mediastinal PC in the setting of secondary hyperparathyroidism due to CKD IV in a patient with history of resected parathyroid adenoma. Persistent hypercalcemia despite appropriate treatment should prompt further evaluation for other etiologies including rare ectopic sites. Management requires medical optimization and surgical resection; clear margins on histology are essential to reduce the risk of recurrence.
Footnotes
Acknowledgements
We wish to acknowledge T. Eichelberger, MD for providing pathology interpretation and pictures.
Author contribution
C. E., G. E., and S. M. conceptualized the project; C. Ezeani, G. Echefu, and I. Stowe did the literature search and manuscript writing, data collection and manuscript elaboration. D. K. and S. M. are supervising attending and did interpretation and critical revision of the manuscript for intellectual content. S. M. is the article guarantor.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written Informed consent was obtained from the patient for publication of this case report.