
Abstract
Objective
This study was performed to determine the risk factors associated with intensive care unit delirium (ICUD) in patients undergoing invasive mechanical ventilation (IMV) secondary to acute exacerbation of chronic obstructive pulmonary disease (COPD).
Methods
Data involving 620 patients undergoing IMV secondary to acute exacerbation of COPD from 2009 to 2019 at the First Hospital of Hebei Medical University were retrospectively analysed. The primary endpoint was the risk factors associated with developing ICUD. Univariable and multivariable logistic regression analyses were used to identify these risk factors.
Results
Of 620 patients, 93 (15.0%) developed ICUD. In the multivariable analysis, risk factors that were significantly associated with ICUD were increased age, male sex, alcoholism with active abstinence, current smoking, stage 3 acute kidney injury (AKI), and an American Society of Anesthesiologists (ASA) physical status of III.
Conclusion
This study showed that increasing age, male sex, alcoholism with active abstinence, current smoking, stage 3 AKI, and an ASA physical status of III might be associated with a risk of developing ICUD. Even if these risk factors are unaltered, they provide a target population for quality improvement initiatives.
Keywords
Introduction
Intensive care unit delirium (ICUD) is a particularly common complication among hospitalized elderly patients. The cumulative incidence is reportedly >75% when combined with stupor and coma following high-risk procedures (e.g., invasive mechanical ventilation [IMV]).1,2 ICUD is associated with decreased preoperative cognitive reserve. 3 Brain atrophy is not markedly associated with the high incidence of ICUD in elderly patients without dementia. 4 Although delirium is an acute, multifaceted neuropsychiatric phenomenon characterized by universal impairments in attention and cognition,5,6 it has been implicated in perpetual cognitive impairment and dementia. 7 The pathogenesis of delirium and the mechanisms associated with these incapacitating consequences are still unknown. 8 During critical illness, delirium is caused by various insults that may be interrelated and yet separately contribute to perpetual cognitive impairment.8,9
Although delirium has been widely reported in the literature,9,10 risk factors associated with delirium remain incompletely described, incompletely assessed, or improperly treated. 11 IMV-related delirium is an acknowledged complication in the ICU because although many patients undergo IMV, almost no evidence exists on this issue. 12 The duration of delirium can help predict the risk of long-term cognitive impairment; however, few studies have been performed to evaluate the risk factors associated with delirium in patients undergoing IMV following acute exacerbation of chronic obstructive pulmonary disease (COPD).13–15
Data assessing the risk factors associated with ICUD in patients undergoing IMV following acute exacerbation of COPD are lacking. Given the paucity of data, this retrospective cohort study was performed to assess the risk factors associated with ICUD in this population.
Materials and methods
Study population
This study was approved by the nine-member Medical Ethics Committee of the First Hospital of Hebei Medical University in December 2019. Because the current analysis only used data that appeared in the medical record, the requirement for informed consent was waived by our Ethics Review Board. From 1 March 2009 to 31 March 2019, consecutive patients who underwent IMV following acute exacerbation of COPD at our institution (the First Hospital of Hebei Medical University, a tertiary care centre) were retrospectively analysed. The inclusion criteria were IMV following acute exacerbation of COPD and the ability to follow instructions while receiving an in-person delirium assessment. The main exclusion criteria were a lack of clinical data, previous diagnosis of delirium prior to IMV, severe dementia that could not be evaluated, complete global aphasia making the patient unable to follow commands, schizophrenia, a Mini Mental State Examination score of <15, Parkinson’s disease, severe hearing impairment, neuroleptic malignant syndrome, severe brain injury, drug abuse, and pregnancy.
All IMV procedures were performed by three ICU physicians (H.T., Q.M., and M.W.). The relevant data points were identified based on the patient’s electronic medical record. Data retrieval was performed by at least two reviewers. Demographic and clinical data were recorded for all patients, including the medical history, physical examination findings, and imaging and laboratory data. For each patient, appropriate pre-IMV and post-IMV data were assessed during the study period. Medical comorbidities were recorded using the Charlson comorbidity index (CCI), the score of which ranges from 0 to 33, with higher scores indicating more comorbidities. 16 Delirium was defined as an acute state of confusion and disorientation with changes in arousal and attention. 1 Symptoms of ICUD were defined as previously reported. 17 Delirium monitoring was performed using the Confusion Assessment Method for the ICU (CAM-ICU). 18 The researchers were trained to apply the CAM-ICU, and its application was part of the daily nursing protocol. To ensure the validity of these data, all study data were audited by two of the co-authors (H.T. and M.W.).
Statistical analysis
Categorical and continuous variables were compared using the chi-square test and the Wilcoxon rank-sum test, respectively. The associations between risk factors and the development of delirium were assessed using univariable and multivariable logistic regression models. All regression model results are described as an odds ratio (OR) with an associated 95% confidence interval (CI). All statistical analyses were conducted using SPSS 24.0 software (IBM Corp., Armonk, NY, USA). A two-sided p value of <0.05 was considered statistically significant.
Results
In total, 620 eligible patients who underwent IMV following acute exacerbation of COPD were included in the final analysis. The patients’ mean age ± standard deviation was 62.3 ± 11.4 years, and the population comprised 437 men (70.5%) and 183 women (29.5%). The mean CCI (age-adjusted) was 6.0 ± 3.7. At the time of IMV, 173 patients (27.9%) smoked tobacco and 124 (20.0%) had alcoholism with active abstinence. The most common reason for IMV surgery was respiratory failure, which occurred in 214 patients (34.5%). The patients’ baseline data are shown in Table 1.
Demographic and clinical characteristics at the time of IMV.

Data are presented as mean ± standard deviation, n, or n (%).
IMV, invasive mechanical ventilation; BMI, body mass index; BMD, bone mineral density; CCI, Charlson comorbidity index; OCD, obsessive-compulsive disorder; AKI, acute kidney injury; APACHE II, Acute Physiology and Chronic Health Evaluation II; ASA, American Society of Anesthesiologists.
aScores range from 0 to 33, with higher scores indicating more comorbidities.
ICUD occurred in 93 patients (15.0%). The univariable and multivariable analyses showed numerous noteworthy risk factors for developing ICUD, as shown in Table 2. All variance inflation factors were <10. The univariable analysis showed that the CCI (OR, 1.37; 95% CI, 1.01–1.62), duration of IMV (OR, 1.79; 95% CI, 1.15–3.48), surgical admission (OR, 0.73; 95% CI, 0.14–0.88), stage 1 acute kidney injury (AKI) (OR, 1.66; 95% CI, 1.12–2.01), stage 2 AKI (OR, 0.47; 95% CI, 0.23–0.68), and an American Society of Anesthesiologists (ASA) physical status of II (OR, 2.44; 95% CI, 1.26–5.36) were noteworthy risk factors. However, the multivariable analysis showed that these risk factors had no statistical significance. Alcoholism with active abstinence (OR, 0.56; 95% CI, 0.23–0.72), stage 3 AKI (OR, 1.62; 95% CI, 1.01–3.75), and an ASA physical status of III (OR, 1.21; 95% CI, 1.42–4.48) were identified as noteworthy risk factors in the univariable analysis, and these factors remained significant in the multivariable analysis (p < 0.05). The absence of alcohol dependence at the time of IMV was identified as a protective risk factor in the univariable and multivariable analyses (OR, 0.78; 95% CI, 0.36–0.95).
Univariable and multivariable risk factors associated with ICUD.
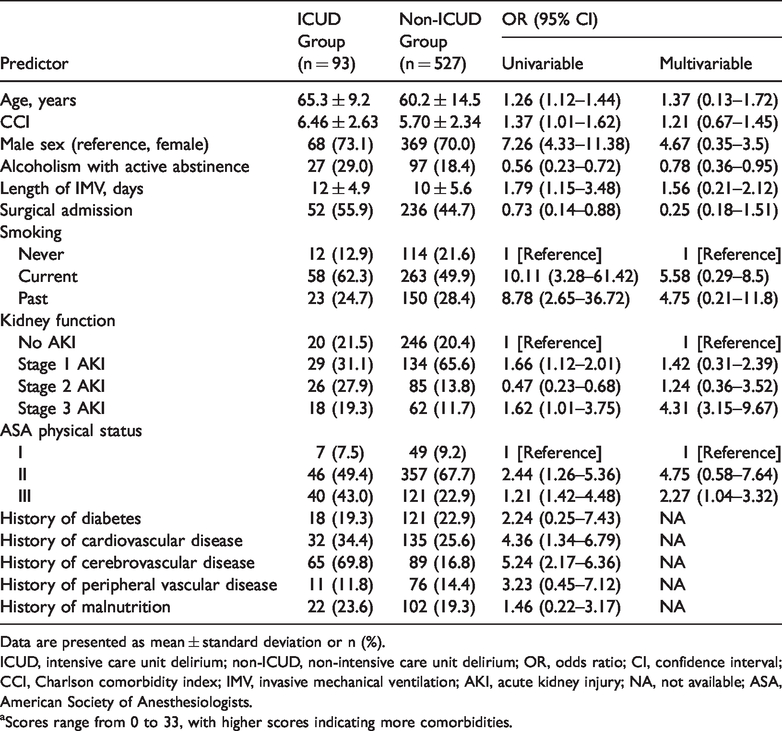
Data are presented as mean ± standard deviation or n (%).
ICUD, intensive care unit delirium; non-ICUD, non-intensive care unit delirium; OR, odds ratio; CI, confidence interval; CCI, Charlson comorbidity index; IMV, invasive mechanical ventilation; AKI, acute kidney injury; NA, not available; ASA, American Society of Anesthesiologists.
aScores range from 0 to 33, with higher scores indicating more comorbidities.
The mean age in the ICUD group was significantly higher than that in the non- ICUD group (65.3 ± 9.2 vs. 60.2 ± 14.5 years, respectively; p < 0.05), and most of the patients who developed ICUD were male (68 [73.1%]). Smoking was associated with a higher rate of developing ICUD, with a higher risk among current smokers (58 of 93 patients [62.3%]) than non-smokers (12 of 93 patients [12.9%]). A history of cardiac and cerebrovascular disease was identified as a significant risk factor in the univariable analysis (p < 0.05).
Discussion
This retrospective study characterized the large-sample outcomes of patients undergoing IMV secondary to acute exacerbation of COPD and provided compelling evidence that increasing age, male sex, alcoholism with active abstinence, current smoking, stage 3 AKI,19,20 and an ASA physical status of III tend to be noteworthy risk factors for the development of ICUD.
Although there are many models for the stratification of patients at risk of developing ICUD, a definite model for clinical implementation is lacking.1,21 A review of risk-stratification models conducted by Newman et al. 22 showed that significant between-model heterogeneity was present and that difficulties in implementation could be a barrier to broader application of these models. This situation is mostly attributed to the unclear definition of individual risk factors for the development of ICUD.23,24 Moreover, substantial heterogeneity has been seen in the baseline data of previous studies2,3 with irrelevant risk factors that were identified using a multivariable logistic regression model. Since Marcantonio 1 established a predictive model of ICUD, an age of ≥70 years has been regarded as a risk factor for ICUD. Booka et al. 25 assessed an age of ≥70 years as the only variable resulting in the development of ICUD in their multivariable analysis. Hasegawa et al. 26 demonstrated that patients aged ≥75 years had an increased risk of developing ICUD (OR, 6.83; 95% CI, 2.47–18.90). When Wang et al. 27 stratified patients by age, they found that the rate of ICUD following IMV surgery increased with each decade of life (R = 0.97). Our findings are in accordance with most of these published studies. We identified increasing age as an important risk factor for developing ICUD, with each year of increased age elevating the risk multiplicatively by a factor of 1.01 (95% CI, 1.00–1.21).
Few studies have evaluated risk factors associated with delirium in patients undergoing IMV surgery following acute exacerbation of COPD.28,29 Findings from previous reports have shown that alcohol and tobacco abuse is associated with the development of ICUD.12,29 In accordance with these reports, the current results showed a higher rate of ICUD in alcohol-dependent patients. Our study is distinctive by revealing that regardless of whether a patient had a history of alcohol dependence, abstinence around the time of IMV surgery appreciably decreased the risk of developing ICUD. Moreover, an increasing but still exceedingly limited body of literature has revealed a significant reduction in the rate of ICUD from 73% to 12%.10,17 One study showed a low rate of ICUD after IMV following acute exacerbation of COPD. 30 This may be partly attributed to the outcomes of non-alcohol-dependent subjects because of the potential for alcohol to worsen cerebrovascular risk.1,2 Similarly, a reduced rate of ICUD was noted in a study by Girard et al. 24 evaluating risk factors associated with delirium in patients. Combined with these reports, our study verifies that patients with alcohol dependence are at higher risk of developing ICUD. The specific reasons for developing ICUD are unclear.1,21 Risks of developing ICUD remain an extensive concern. 21 However, the available studies on the development of ICUD remain deficient. Wan et al. 31 performed a single-centre case-control study conducted in a 30-bed mixed ICU in the United Kingdom and demonstrated that stage 3 AKI was independently associated with hyperactive delirium (OR, 5.40; 95% CI, 2.33–12.51). Other independent risk factors were IMV (OR, 2.70; 95% CI, 1.40–5.21) and alcohol dependence (OR, 5.80; 95% CI, 1.90–17.72). However, in a study of the effect of haloperidol on survival, Van Den Boogaard et al. 32 conducted a randomized, double-blind, placebo-controlled investigator-driven study involving 1789 critically ill adults treated at 21 ICUs and found no difference regarding IMV.
Several limitations of the present study should be acknowledged. First, the retrospective nature and lack of detailed data to adjust for other risk factors make our results vulnerable to errors and could lead to weakened power to draw definitive conclusions. An attempt was made to avoid potential confounding variables; nevertheless, our analysis could be defective. We might not have captured all patients undergoing IMV following acute exacerbation of COPD from the database because of imprecise COPD codes. Nevertheless, we attempted to assess the most homogeneous and specific sample possible. A lack of imaging data is also a factor in the interpretation of our findings. Second, despite application of the same protocol, there may have been individual differences that were not documented. Third, we failed to assess additional risk factors related to the development of ICUD. Finally, this was a single-centre study and its generalizability may therefore be limited.
In conclusion, the results reported in this study support a growing body of evidence that increasing age, male sex, alcoholism with active abstinence, current smoking, stage 3 AKI, and an ASA physical status of III tend to be associated with a high risk of developing ICUD in patients with COPD. Understanding the risk factors and clinical aspects of ICUD may provide us with a better ICUD management strategy in these patients. Patients with COPD who have the above characteristics might be regarded as a high-risk category, and monitoring their cognition throughout their stay in the hospital might be key in the prevention and management of delirium.