
Abstract
Objective
To investigate management and implementation of the “awakening and breathing trials, choice of drugs, delirium management, and early exercise/mobility” (ABCDE) bundle in the pediatric intensive care unit (PICU) in southwestern China
Methods
A self-designed questionnaire for determining implementation of the ABCDE bundle was distributed to healthcare professionals in the PICU. Multiple linear regression was used to analyze results.
Results
A total of 270 questionnaires were collected. There was no significant difference in the awareness of the ABCDE bundle rate among Sichuan, Guizhou, and Yunnan workers. Only dynamic adjustment of drug dose accounted for more than half (55.5%) of “frequent implementation” and “general implementation”, followed by implementation of sedation assessment, pain assessment, and spontaneous breathing trials (46.4%, 39.3%, and 35.6%, respectively). A total of 80.4% of healthcare professionals never performed screening of delirium. Multivariate analysis showed that the healthcare professionals’ scores of ABCDE bundle behavior significantly differed regarding awareness of the ABCDE bundle, years of work at the hospital, the region of hospitals, and occupational category.
Conclusion
Implementation of the ABCDE bundle in the PICU in southwestern China is not sufficient. Existing problems need to be identified and a standardized sedation and analgesia management model needs to be established.
Keywords
Introduction
Children who are admitted to the pediatric intensive care unit (PICU) are in a high-stress environment. Common causes of stress include the following: 1 1) stress caused by trauma, infection, and other diseases, and frequent invasive procedures; 2) being separated from parents; appearance of many strange faces and instruments; noise and long lights disturbing the biological clock; 3) worry about the disease and prognosis and fear of death; and 4) various intubations and being bedridden. Interestingly, children undergoing mechanical ventilation (MV) may develop patient–ventilator dyssynchrony. This leads to difficulty in ventilation and delayed weaning, thereby affecting the clinical efficacy and also worsening the conditions. Therefore, sedation and analgesia are recommended as treatment for children undergoing MV.1–4 However, improper sedation and management of analgesia can result in harm and poor prognosis for children.5,6
Improper use of sedative and analgesic drugs is a cause of delirium. The incidence of delirium in the PICU ranges between 5% and 53%,7–9 and delirium during a hospital stay significantly increases the duration of MV, the length of hospital stay, and the cost of hospitalization.10,11 Another study suggested that anesthetics and sedatives adversely affect neurological function of pediatric patients. 12 Because of damage and an unfavorable prognosis caused by improper analgesia and sedation for children with MV, appropriate strategies and interventions need to be adopted to maintain moderate analgesia and sedation and reduce the incidence of adverse consequences.
Pandharipande et al. 13 first proposed the evidence-based “awakening and breathing trials, choice of drugs, delirium management, and early exercise/mobility” (ABCDE) bundle. The specific contents of this bundle include daily awakening, breathing coordination, choices of sedative or analgesic drugs, management of delirium, and early exercise. A recent prospective cohort study showed that the ABCDE bundle effectively reduced the MV time, the length of hospital stay, and the hospitalization cost. 14 Currently, this strategy has been safely implemented in a large number of adult intensive care units (ICUs) worldwide with satisfactory results. 15 However, at present, there is no guideline for the children’s ABCDE bundle. The ABCDE bundle requires teamwork and can be led by an experienced physician or nurse. The team usually includes physicians, nurses, respiratory therapists, rehabilitation therapists, and even psychiatrists.
Management and implementation of the ABCDE bundle in the PICU in China has not been reported. Therefore, the present survey aimed to determine the current status of implementation of the ABCDE bundle in the PICU of Class A tertiary hospitals in the southwestern provincial capitals of China to provide effective evidence for establishing a scientific sedation and analgesia management model in children.
Material and methods
Participants
The convenient sampling method was used to select 6 of 12 Class A tertiary hospitals with a PICU in the southwestern provincial capitals of China (Chengdu in Sichuan Province, Guiyang in Guizhou Province, and Kunming in Yunnan Province) from March to April 2019. An online survey of PICU healthcare professionals was performed from June to July 2019. Inclusion criteria were as follows: 1) practicing certificates of certified physicians and nurses; and 2) PICU healthcare professionals working in the hospital. Exclusion criteria were interns and residents who received standardized training and trainee physicians in the departments. The survey was reviewed by the West China Second University Hospital of Sichuan University Ethics Committee (2014SZ0004-9). Written informed consent was obtained from the participants before the study. Participation was voluntary, and anonymity and confidentiality were assured.
Assessment and measurement of the ABCDE bundle
We collected baseline information on sex, age, occupation, professional ranks and titles, education level, years of working in the hospital (<1, 1–2, 3–5, 6–10, and ≥11 years), years of working in the PICU (<1, 1–2, 3–5, 6–10, and ≥11 years), and regions of the hospital.
Implementation of the ABCDE bundle was based on the relevant literature worldwide and the Experts’ Consensus on Sedation and Analgesia for Children in Pediatric Intensive Care Unit of China (2018) 1 . We used a self-designed questionnaire that included nine items, such as daily awakening, also known as spontaneous awakening trials (SATs), spontaneous breathing trials (SBTs), drug selection and adjustment, assessment of the risk of delirium, and early exercise. The Likert grade 4 scoring standard was used (never implemented=1, occasionally implemented [implemented in <25% of children]=2, frequent implementation [25%–75% of children]=3, and general implementation [>75% of children]=4). Selection of participants was made on the basis of experience of the subjects within 3 months. The sum of the scores was calculated to assess implementation of the ABCDE bundle; the total score was 36 points and a higher score indicated better compliance with the ABCDE bundle. This questionnaire was evaluated and reviewed by five experts of critical care medicine at the Department of Critical Care Medicine, West China Second University Hospital of Sichuan University. Additionally, the content validity index was 0.781. Twenty-five nurses and five physicians were randomly selected from the Department of Critical Care Medicine, West China Second University Hospital of Sichuan University to conduct a pre-survey and calculate the Cronbach’s alpha as 0.723. Other assessments included analgesia, commonly used pain assessment scales, commonly used sedatives and analgesics, delirium management status, and non-drug interventions.
Quality control
The questionnaire was initially developed on the basis of a literature review. The Delphi method was used two times on the five experts of critical care medicine to determine the final questionnaire. A pre-survey was conducted to improve the contents of the questionnaire on the basis of existing problems. In the implementation stage, the personnel in charge of the project went to the site to conduct unified training for respondents in each hospital, and the inclusion, exclusion, and the questionnaire filling out criteria were determined. Participants logged in to the https://jinshuju.net questionnaire survey site and filled out the online questionnaire. The questionnaire used an online anonymous survey mode to ensure that the data were objective and true. The integrity and logic of the collected questionnaire were checked. Questionnaires with no logical loopholes or distinct regularity were considered valid, and those with >20% missing options were invalid.
Statistical analysis
Statistical analysis was performed using IBM SPSS 19.0 software (IBM Corp., Armonk, NY, USA). Measurement data with a normal distribution are shown as mean ± standard deviation. Between-group comparisons were made by the t-test and comparisons among more than two groups were made by the least significant difference test t-test. Data that did not conform to a normal distribution are shown as median (95% confidence intervals), and comparison between groups was performed by a non-parametric test. Count data are described by the number of cases (percentage), and comparison between groups was made by the chi-square test. P values <0.05 (two-sided) were considered statistically significant. The multiple linear regression model (stepwise method) was used to analyze factors that affected the score of ABCDE bundle behavior of the healthcare professionals. The total score of ABCDE bundle behavior was used as the dependent variable. Statistically significant variables in bivariate analysis were used as independent variables to construct the regression equation. Factors with P<0.05 in bivariate analysis were used for further analysis in multiple linear regression, and unordered multicategory variables were entered into the multiple linear regression model as dummy variables.
Results
Baseline data
A total of 270 (90%) questionnaires were collected from 300 eligible healthcare professionals. The cohort consisted of 31 (11.5%) men and 239 (88.5%) women, and the mean age was 30.23±7.58 years. Of the 60 (22.2%) physicians and 210 (77.8%) nurses, 164 (60.7%) were assistant doctor/nurse aides (junior professional title), 75 (27.8%) were doctors in charge/nurses in charge (middle-rank professional title), and 31 (11.5%) were Associate Professors of medicine/Associate Professors of nursing or Professors of medicine/Professors of nursing (senior professional title). The cohort consisted of 72 (26.7%) participants with junior college education or below, 177 (65.5%) with a university degree, and 21 (7.8%) with graduate degree or above. Furthermore, 117 (43.3%) participants were in Sichuan, 76 (28.1%) in Guizhou, and 77 (28.5%) in Yunnan.
Status of clinical implementation of the ABCDE bundle for healthcare professionals
The mean score of the healthcare professionals was 19.74±5.47 points. Only dynamic adjustment of drug dose accounted for more than half (55.5%) of “frequent implementation” and “general implementation,” followed by implementation of sedation assessment, pain assessment, and SBTs (46.4%, 39.3%, and 35.6%, respectively). A total of 80.4% of the healthcare professionals never performed assessment of the risk of delirium (Table 1).
Status of clinical implementation of the awakening and breathing trials, choice of drugs, delirium management, and early exercise/mobility bundle for healthcare professionals (n = 270).

SATs, spontaneous awakening trials; SBTs, spontaneous breathing trials.
The overall awareness rate of the ABCDE bundle was 53.7%. The awareness rate of the ABCDE bundle was 56.4% in Sichuan, 47.4% in Guizhou, and 55.8% in Yunnan, with no significant difference among the three regions (P=0.425). The most common sedation assessment scale was Ramsay and that for pain assessment was the Faces Pain Scale. The most commonly used sedative and analgesic was midazolam and sufentanil, respectively. The most commonly used delirium assessment scale was the Pediatric Confusion Assessment Method for the ICU, the most common intervention drug for delirium was haloperidol, and reducing noise and light was a common non-drug intervention (Table 2).
Common consciousness, pain, and delirium assessment scales and the distribution of drugs.

SAS, Riker sedation-anxiety score; RASS, Richmond agitation and sedation score; BIS, bispectral index; NRS: numerical rating scale; VRS, verbal rating scale; VAS, visual analog scale; FPS, faces pain scale; FLACC, face, legs, activity, crying, consolability; CRIES, crying, requires O2 saturation, increased vital signs, expression, sleeplessness; CHEOPS, cry, facial, child verbal, torso, touch, legs; pCAM-ICU, Pediatric Confusion Assessment Method for the ICU; CAPD, Cornell Assessment of Pediatric Delirium; PAED, pediatric anesthesia emergence delirium; ICDSC, intensive care delirium screening checklist.
Analysis of factors affecting ABCDE bundle behavior
Bivariate analysis of factors affecting ABCDE bundle behavior
Bivariate analysis showed significant differences in the scores of ABCDE bundle behavior for sex, occupation category, professional ranks and titles, working years in the hospital, working years in the PICU, regions of the hospital, and understanding of the ABCDE bundle (all P<0.05) (Table 3).
Bivariate analysis of scores of ABCDE bundle behavior for healthcare professionals (n = 270).
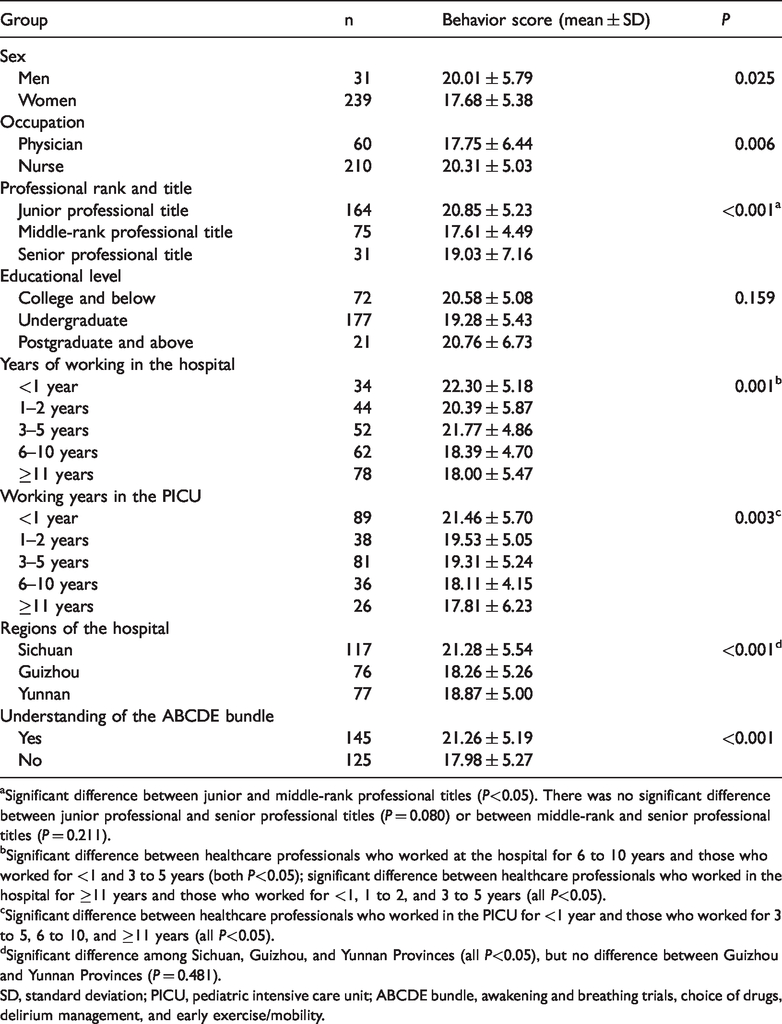
aSignificant difference between junior and middle-rank professional titles (P<0.05). There was no significant difference between junior professional and senior professional titles (P = 0.080) or between middle-rank and senior professional titles (P = 0.211).
bSignificant difference between healthcare professionals who worked at the hospital for 6 to 10 years and those who worked for <1 and 3 to 5 years (both P<0.05); significant difference between healthcare professionals who worked in the hospital for ≥11 years and those who worked for <1, 1 to 2, and 3 to 5 years (all P<0.05).
cSignificant difference between healthcare professionals who worked in the PICU for <1 year and those who worked for 3 to 5, 6 to 10, and ≥11 years (all P<0.05).
dSignificant difference among Sichuan, Guizhou, and Yunnan Provinces (all P<0.05), but no difference between Guizhou and Yunnan Provinces (P = 0.481).
SD, standard deviation; PICU, pediatric intensive care unit; ABCDE bundle, awakening and breathing trials, choice of drugs, delirium management, and early exercise/mobility.
Multivariate analysis of factors affecting ABCDE bundle behavior
The multiple regression equation included the following: the region of the hospital (Sichuan = [0, 0, 0], Guizhou = [0, 1, 0], Yunnan = [0, 0, 1); understanding of the ABCDE bundle (yes = 1, no = 2); working years in the hospital (<1 year = 1, 1–2 years = 2, 3–5 years = 3, 6–10 years = 4, and ≥11 years = 5); and occupational category (nurse = 0, physician = 1). Multivariate analysis showed that the healthcare professionals’ scores of ABCDE bundle behavior significantly differed in terms of awareness of the ABCDE bundle, years of work at the hospital, the region of hospitals, and occupational category (all P < 0.05, Table 4).
Factors associated with awakening and breathing trials, choice of drugs, delirium management, and early exercise/mobility bundle behavior using multivariable analysis.
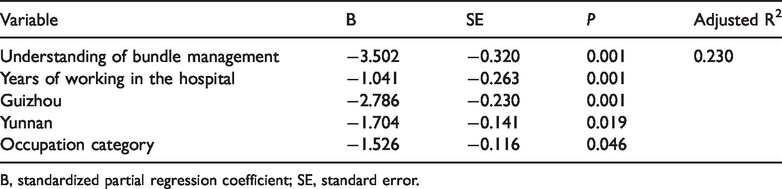
B, standardized partial regression coefficient; SE, standard error.
Discussion
Approximately half of the respondents in this study were not aware of the ABCDE bundle strategy, which is similar to data (58.4%) from a survey of nurses in Italy. 16 This finding indicates that the relevant knowledge reserve and update of healthcare professionals require improvement by training to strengthen the scientific management of sedation and analgesia. A recent survey of global adult ICUs showed that the proportion of implementing daily routine awakening and SBTs was 59% and 67%, respectively. 15 Additionally, 42% of the respondents reported that they would use SATs and SBTs simultaneously. The proportion of routine use of the pain assessment scale and sedation scale was 83% and 89%, respectively. In our study, in addition to dynamically adjusting the dose of drugs, the proportion of the remaining ABCDE bundle procedures in “frequent implementation” and “general implementation” was less than 50% and greatly lagged behind the international adult ICU level. This phenomenon could be attributed to the current severe shortage of medical resources of pediatric critical care medicine and healthcare professionals who are involved in the daily resuscitation of critical children and recovery of diseases and organ function. Therefore, implementing sedation and analgesia management clinically is difficult. The provincial capital is usually a regional gathering center of high-quality medical resources, which can largely reflect the medical level in the region. However, based on the survey of our study, implementation of the ABCDE bundle in the southwestern provincial capitals could be improved, which should attract attention from medical nursing colleges of pediatric critical care medicine. Moreover, allocation of human resources should be strengthened, and medical nursing procedures of the PICU should be scientifically implemented.
Delirium significantly increases the MV time, length of hospital stay, and hospitalization costs, and is independently related to mortality.7,17,18 Delirium may also be manifested as post-traumatic stress disorder, depression, anxiety, and change in future cognitive function after discharge. 19 Although numerous studies have emphasized the need for screening and intervention of delirium in critical children, clinical implementation in the PICU has not yet been achieved. The proportion of never implementing delirium screening in the current study was 80.4%, which is much higher than that in a Chinese report on the adult ICU (36.6%). 20 Only 1.1% of healthcare professionals reported that they would conduct assessment of delirium frequently in our study. This finding is similar to that of a PICU survey of North America that showed that only 2% of healthcare professionals routinely conducted screening of delirium twice a day. 21 Because children are subject to changes in language and age, assessing their delirium is challenging. The current study showed that the Pediatric Confusion Assessment Method for the ICU was the most commonly used screening tool for delirium, but this scale is only applicable to children aged >5 years. 22 This is because younger children do not cooperate easily, thereby reducing compliance. In 2016, the European Society of Pediatric and Neonatal Intensive Care recommended use of the Cornell Assessment of pediatric delirium (CAPD) tool for assessing delirium in children (level of evidence A). 23 This scale is adaptive to children aged 0 to 21 years or those with developmental retardation 6 and a single assessment requires 2 minutes, which improves compliance of children. The Children’s Hospital of Chongqing in China 24 has completed Chinesization and cross-cultural adjustment of the CAPD scale. The Chinese version of the CAPD assesses the occurrence of delirium in children with strong feasibility and applicability as clinical observations. However, large-scale epidemiological data on delirium in children in China are still unavailable.
The present study showed that healthcare professionals with fewer working years and a junior professional title had higher compliance with the ABCDE bundle, which is inconsistent with survey findings by Lu et al. 20 Critical care medicine is a highly specialized and rapidly developing discipline that requires continuous learning to update and acquire new knowledge and skills. Studies have shown that a lack of knowledge and awareness is a major factor affecting employees’ ABCDE bundle behavior.25,26 Healthcare professionals with less working years and a junior professional title may receive more training and are more willing to accept new concepts during recruitment. Our study also showed that the nurses’ scores of ABCDE bundle behavior were higher than those of physicians. As a population who has frequent contact with children, nurses play multiple roles as leaders, organizers, and implementers in management of the ABCDE bundle. This is consistent with the ICU survey results of a study by Zhou et al. 27 However, some studies showed that, for each unit, the compliance of the ABCDE bundle was reduced by 53% as the workload increased. 28 This finding suggests that managers should pay attention to the nurses’ workload and rationally allocate human resources to improve compliance of the ABCDE bundle. Additionally, some studies have shown that tedious document writing, a heavy workload, and a lack of core leaders affect implementation of the ABCDE bundle. 29 Good teamwork eases implementation of the ABCDE bundle and increase the healthcare professionals’ confidence. 30 Nevertheless, further investigation is required regarding the factors affecting implementation of the ABCDE bundle in the PICU in China.
The present study has human limitations and restricted financial resources. We did not include all hospitals with a PICU in the southwest of China, and the sample representation may have been biased. Additionally, this was a cross-sectional study, which only analyzed the effects on general information of healthcare professionals. Furthermore, the adjusted R2 was not high enough, which meant that there was a 23% probability that the obtained multiple linear equation was valid. Actually, healthcare professionals’ awareness was highly related to their implementation of the ABCDE bundle, but we did not conduct an in-depth study of the related influencing factors. Therefore, the factors affecting implementation of the ABCDE bundle in the PICU require further investigation.
In conclusion, implementation of the ABCDE bundle in the PICU in southwestern provincial capitals of China still lags behind that of adult ICUs. Moreover, specific implementation of the ABCDE bundle in the PICU in management of delirium worldwide is not optimistic. Therefore, the relevant managers need to pay more attention to the ABCDE bundle and analyze the existing problems of managing sedation and analgesia in the PICU. Furthermore, by combining the characteristics and existing resources in this field, a scientific and standardized sedation and analgesia management model should be established to improve the quality of medical nursing and prognosis of children.
Footnotes
Acknowledgements
We thank five experts of pediatric critical care medicine (Lina Qiao, MD, DeYuan Li, MD, Zhongqiang Liu, MD, Yang Wang, and Haiyang Zhang) for their help in developing and implementing this questionnaire.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Sichuan Health and Family Planning Commission Popularization and Application Project (18PJ214).