
Abstract
Objective
To identify the factors influencing early recurrence in patients with hepatocellular carcinoma (HCC) after curative resection.
Methods
Clinical data for 99 patients with HCC undergoing curative resection were analyzed. The clinicopathological factors influencing early recurrence were analyzed by Cox regression.
Results
Twenty-five of 99 patients (25.3%) suffered from early recurrence. There were significant differences between patients with and without recurrence in terms of tumor diameter, tumor capsular integrity, and preoperative alpha fetoprotein level. Cox regression analysis revealed that a tumor diameter >2.6 cm and preoperatively increased total bilirubin (TBL) level were risk factors for postoperative recurrence, while tumor capsular integrity had a protective effect on postoperative recurrence. After adjusting for preoperative TBL level and tumor capsular integrity, the risk of HCC recurrence was markedly increased in line with increasing tumor diameter in a non-linear manner.
Conclusion
Tumor diameter >2.6 cm and preoperatively increased TBL level are associated with a higher risk of early recurrence after curative resection in patients with HCC, while tumor capsular integrity is associated with a lower risk of early recurrence.
Keywords
Introduction
Cancer is the leading cause of death worldwide after cardiovascular diseases, with liver cancer ranked the fourth most common cause of cancer-related deaths.1,2 In 2015, 854,000 cases of liver cancer and 810,000 deaths were estimated worldwide, 2 with an incidence and mortality of 446.1 and 422.1 per 100,000 in China. 3 Liver cancer derived from liver cells or intrahepatic biliary epithelial cells is classified into hepatocellular carcinoma (HCC), cholangiocellular carcinoma, and mixed carcinoma, 4 of which HCC accounts for the majority of cases.5,6
The development and progression of HCC are closely associated with chronic liver diseases, especially liver cirrhosis, 7 and approximately 80% to 90% of cases of HCC develop in the context of liver cirrhosis.8,9 There are currently various treatment modalities for HCC, including surgical resection, percutaneous ablation, transcatheter arterial chemoembolization, and liver transplantation, of which surgical resection is considered the optimal modality for early-stage HCC.10,11 However, the recurrence rate of HCC after resection has been reported to be up to 70%, and it is frequently difficult to distinguish between new lesions appearing within 2 years and primary tumor recurrence, sometimes as metachronous HCC.3,12,13 Numerous studies have demonstrated that early recurrence is associated with a poor prognosis in patients with HCC after curative resection. Compared with late recurrence, the prognosis of patients with early recurrence is worse regardless of the cut-off value for recurrence time.14–16 There is thus a need to identify the risk factors for postoperative recurrence to improve the prognosis of patients with HCC undergoing curative resection.
In the present study, we retrospectively analyzed the clinical data for patients with HCC who underwent curative resection and investigated the factors affecting early recurrence, with the aim of identifying factors predicting early recurrence of HCC and thus allowing timely interventions to improve the prognosis.
Materials and methods
Patients
The clinical data for patients with HCC who underwent curative resection at Taizhou Hospital of Zhejiang Province between 1 January 2012 and 31 August 2018 were analyzed. All the patients participated voluntarily in the study and provided informed consent. The study was approved by the Institutional Review Board of Taizhou Hospital of Zhejiang Province (approval No.: K20181004).
The inclusion criteria were as follows: presence of HCC based on preoperative computed tomography (CT) or magnetic resonance imaging (MRI); initially confirmed as HCC by postoperative pathological diagnosis; and Child–Pugh grade A–B. Exclusion criteria were: patients undergoing second surgery or preoperative radiotherapy and chemotherapy; other organ metastases, e.g. lung and brain; and incomplete clinical data.
Clinicopathological data
The following clinicopathological data were collected through the hospital’s case management system: age, sex, tumor diameter, number and capsular integrity, Child–Pugh score, Edmondson classification, preoperative alpha fetoprotein (AFP) level, alanine aminotransferase and total bilirubin (TBL), presence or absence of liver cirrhosis, microvascular invasion, anatomical resection, ascites, hepatitis B surface antigen, intraoperative transfusion, and relevant blood indicators.
Follow-up
After surgery, the patients were followed-up by outpatient reexamination and telephone up to 31 August 2019. The follow-up was conducted every month for the first 3 months after surgery, then every 3 months to 1 year and every 6 months thereafter. Reexaminations included liver function, AFP, upper abdominal CT or MRI examination, chest CT examination, and hepatobiliary B-mode ultrasound. The time to tumor recurrence was evaluated based on the presence of masses detected by CT and MRI.
Statistical analysis
The data were analyzed using R software version 3.6.1 (www.r-project.org). Data with normal and non-normal distributions were presented as mean ± standard deviation and analyzed by t-tests and as median and quartiles (Q1, Q3) and analyzed by Mann–Whitney U rank-sum tests. Numerical data were compared by χ2 or Fisher’s exact tests and presented as n (%). Factors affecting factors for early recurrence were analyzed by Cox regression analysis, and variables entered into multivariate analysis were chosen based on the minimum Akaike information criterion. Postoperative recurrence curves were created by the Kaplan–Meier method and compared between groups using log-rank tests. After adjusting for confounding factors with statistical significance in multivariate Cox regression analysis, the dose-response relationship between tumor size and recurrence risk was analyzed according to a three-node restrictive cuboidal model of Cox regression, with three nodes located at the 25, 50, and 75 percentiles of tumor size. P < 0.05 was considered statistically significant.
Results
Patient characteristics
A total of 856 patients with HCC underwent surgery and were discharged from hospital between 1 January 2012 and 31 August 2018, among whom 300 cases received curative resection. After excluding 101 patients with incomplete follow-up information, 67 undergoing second surgery or preoperative radiotherapy and chemotherapy, and 33 with other organ metastases, 99 eligible patients were finally included in the study. Twenty-five patients experienced recurrence within 2 years after surgery, and 74 did not, and the early recurrence rate was therefore 25.3%. The patient characteristics are shown in Table 1. There were significant differences between the recurrence and non-recurrence groups in terms of tumor diameter, tumor capsular integrity, and preoperative AFP (all P < 0.05).
Baseline characteristics of patients.

Values presented as mean ± standard deviation or median (quartile [Q1, Q3]).*Data analyzed by Fisher’s exact test.AFP, alpha fetoprotein; ALT, alanine aminotransferase; TBL, total bilirubin; HBsAG, hepatitis B surface antigen.
Univariate analysis of risk factors for early recurrence
Univariate Cox regression analysis identified tumor diameter >2.6 cm as a risk factor for postoperative recurrence in patients with HCC [hazard ratio (HR): 3.25, 95% confidence interval (CI): 1.21–8.77, P = 0.019], while tumor capsular integrity was a protective factor for postoperative recurrence (HR: 0.28, 95%CI: 0.110.70, P = 0.007) (Table 2).
Cox regression analysis of factors influencing HCC recurrence.

AFP, alpha fetoprotein; ALT, alanine aminotransferase; TBL, total bilirubin; HBsAG, hepatitis B surface antigen.
Multivariate analysis of risk factors for early recurrence
Multivariate Cox regression analysis identified tumor diameter >2.6 cm (HR: 4.77, 95%CI: 1.65–13.73, P = 0.003) and preoperatively increased TBL level (HR: 1.06, 95%CI: 1.01–1.12, P = 0.016) as risk factors for postoperative recurrence of HCC, while tumor capsular integrity (HR: 0.24, 95%CI: 0.09–0.66, P = 0.005) was a protective factor (Table 2). The recurrence risk increased by 6% for every 1 µmol/L increase in preoperative TBL.
There was a significant difference in postoperative recurrence time between patients with tumor diameter >2.6 cm and ≤2.6 cm (P = 0.014) (Figure 1). After adjusting for confounding factors including preoperative TBL level and tumor capsular integrity, we produced a restrictive cuboidal model of tumor size and recurrence risk (Figure 2), which showed a significant nonlinear increase in HCC recurrence risk in line with increasing tumor size (P = 0.019).
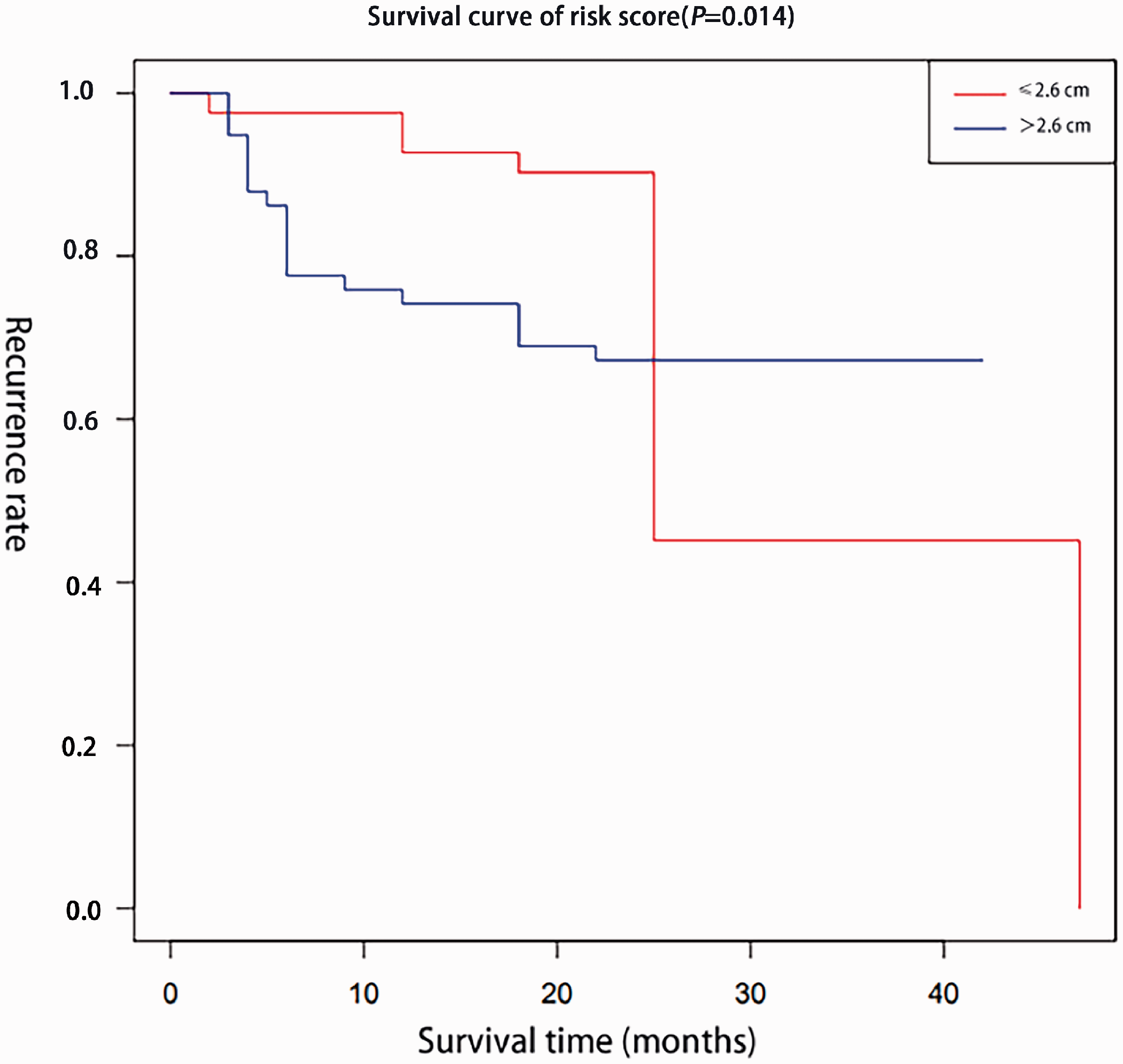
Postoperative recurrence curves for patients with hepatocellular carcinoma with tumor diameter >2.6 cm and those with tumor diameter ≤2.6 cm.
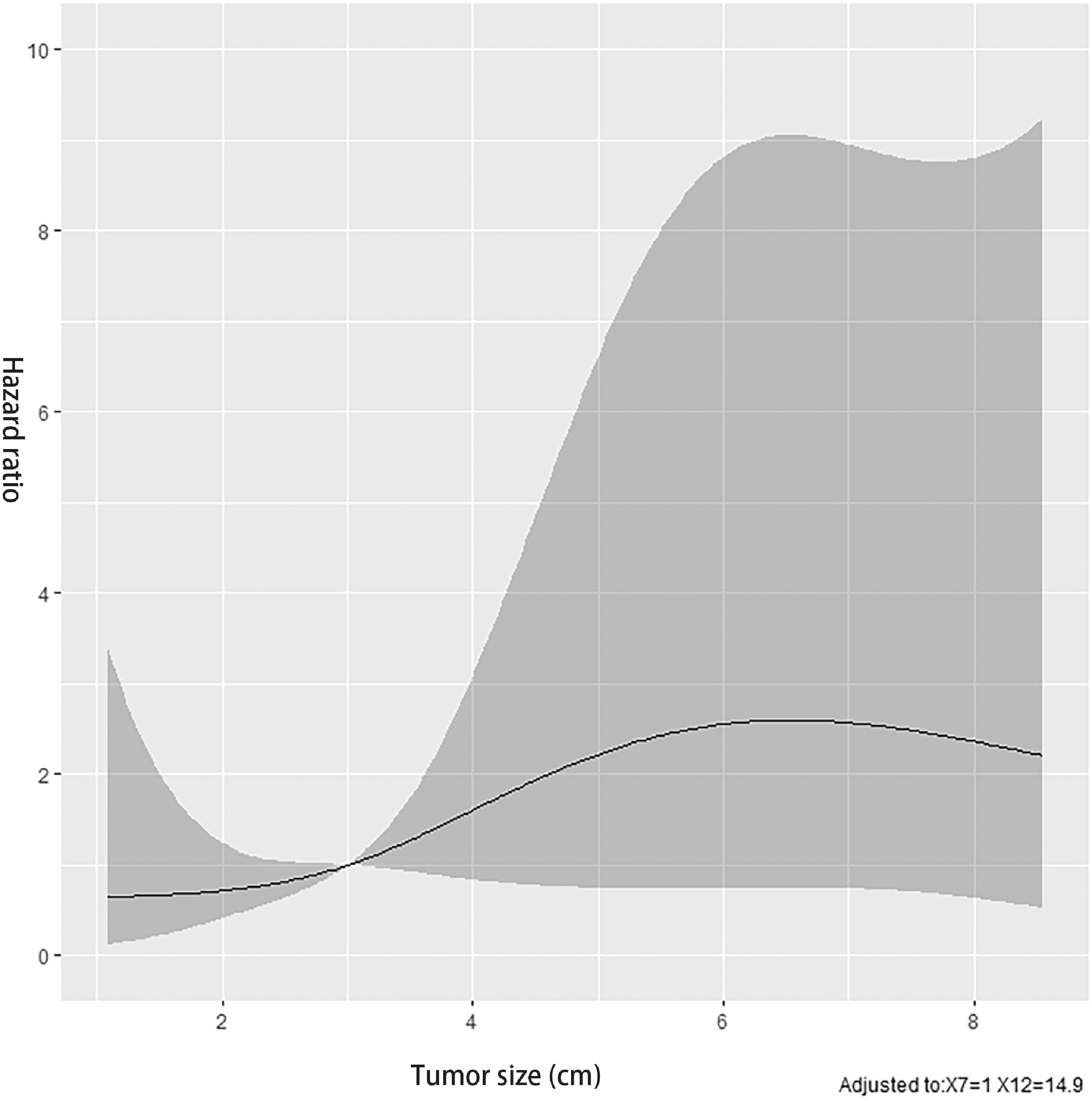
Dose-response relationship between tumor size and recurrence risk in patients with hepatocellular carcinoma.
Discussion
HCC is generally thought to originate from chronic inflammation in the liver caused by several factors, including alcoholic/non-alcoholic fatty liver disease and hepatitis virus infection. Even after curative resection, patients remain at high risk of hepatocarcinogenesis. 17 Metachronous HCC, new postoperative lesions, and intrahepatic metastasis from primary HCC are relatively common following liver resection, and timely prediction of postoperative recurrence is thus important for improving patient prognosis. 18 In the present study, 25 out of 99 patients with HCC suffered from recurrence within 2 years after curative resection, with tumor diameter >2.6 cm and preoperatively increased TBL levels determined to be risk factors, and tumor capsular integrity identified as a protective factor.
Postoperative recurrence of HCC is considered to be closely associated with the biological properties of the HCC itself, such as tumor size, capsular integrity, differentiation degree, and presence or absence of vascular invasion,19,20 with larger tumor size confirmed as a key parameter affecting early recurrence. 21 Compared with patients with a tumor diameter ≤3.5 cm, patients with larger tumors (>3.5 cm) had a higher risk of postoperative recurrence. 22 However, the current results indicated that the risk of postoperative recurrence in HCC patients with a tumor diameter >2.6 cm was 4.77 times higher than that of those with a tumor diameter ≤2.6 cm, with a significant difference in postoperative recurrence time, suggesting that a tumor diameter of 2.6 cm might be a better cut-off point for predicting postoperative HCC recurrence. However, although the recurrence risk was obviously increased in line with increased tumor size, suggesting that a larger tumor size was associated with a higher recurrence risk of HCC, the relationship was non-linear, possibly because of the small sample size.
TBL is an indicator of liver function and can accurately reflect the injured condition of liver cells. HCC patients with impaired liver function or inadequate resection margins have been reported to be prone to recurrence. 23 Our results indicated that a preoperatively increased TBL level was an independent risk factor for postoperative recurrence in HCC patients, and that the recurrence risk increased by 6% for every 1 µmol/L increase in preoperative TBL. Moreover, tumor capsular integrity was identified as a protective factor for postoperative recurrence of HCC. The tumor capsule provides a powerful barrier preventing HCC cells from diffusion and metastasis, and thus protects against HCC infiltration; however, this function is lost in non-capsular HCC or in HCCs with broken capsules. 24 The current study demonstrated that non-capsular HCC was associated with a higher incidence of vascular invasion and poorer differentiation than tumors with capsules. HCCs with and without capsules thus showed lower and higher degrees of malignancy, respectively, with more malignant tumors tending to grow invasively, leading to vascular invasion. 25
The current study had some limitations. First, it was a single-center retrospective study involving a relatively small number of patients (99) compared with the long study duration (2012–2018), which may create a source of bias. Second, treatment-related factors, such as antiviral therapy, targeted therapy, and specific surgical methods, were not included in the analysis of recurrence factors. Further multicenter studies with large samples are therefore needed to verify these results.
Tumor diameter >2.6 cm and preoperatively increased TBL level are associated with a higher risk of early recurrence after curative resection in patients with HCC, while tumor capsular integrity is associated with a lower risk of early recurrence. After adjusting for preoperative TBL level and tumor capsular integrity, the recurrence risk of HCC increases significantly in line with increased tumor size, in a non-linear manner.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Taizhou Science and Technology Plan Project (No: 1701KY05).