
Abstract
This case report describes a woman in her 70s who presented with a 3-month history of hip pain and inability to walk. Upon admission, she was diagnosed with the extremely rare condition of complete femoral head disappearance. A comprehensive examination was conducted to determine the cause and devise an effective treatment strategy, taking the patient’s medical history into account. Through interdisciplinary discussions, occult infection and other potential causes were ruled out. The femoral head disappearance was ultimately determined to be due to wear, ischemia, and absorption following a fracture. After informing the patient of the diagnosis and treatment plan, total hip arthroplasty was proposed. This case highlights the rarity and severity of femoral head disappearance in patients with femoral neck fractures, emphasizing the effectiveness of total hip arthroplasty and appropriate joint prostheses in managing such cases. This case has significant implications for clinical diagnosis, treatment, and complication prevention. The report also discusses the causes of acquired femoral head disappearance, relevant diagnostic assessments, and alternative treatment options.
Keywords
Introduction
Disappearance of the femoral head is a relatively rare and complex condition within the skeletal system, often associated with comminuted fractures and severe osteoporosis. 1 Various other factors such as rheumatic diseases, neoplastic conditions, arthritis, osteonecrosis, disturbances in bone metabolism, and osteolytic diseases may also lead to disappearance of the femoral head.2–4 Following a fracture, complete or partial disappearance of the femoral head and neck can severely impact the patient’s quality of life and the stability of the bone and joint system if timely and effective treatment is not administered. A literature search revealed no published cases similar to this one.
We herein describe a patient with femoral head disappearance, the cause of which was identified through detailed examination and ultimately treated with total hip arthroplasty. This case highlights the rarity and severity of femoral head disappearance as a complication of femoral neck fractures. It also underscores the ineffectiveness of conservative treatment for such fractures. In this report, we provide a detailed overview of the patient’s medical history, physical examination, diagnostic findings, and treatment process. In addition, we explore potential causes of femoral head disappearance, including factors related to fractures and other possible etiologies.
The treatment process emphasizes the importance of thorough examination and multidisciplinary consultation in establishing a precise diagnosis. The immediate effectiveness of total hip arthroplasty in restoring the patient’s mobility is demonstrated, with a satisfactory short-term postoperative assessment. 5 By delving into the complexities of this case, our aim is to offer the medical community a more comprehensive understanding and provide experience and references for the diagnosis and treatment of similar cases in the future.
Case presentation
The reporting of this study conforms to the CARE guidelines. 6
This study received approval for publication, and the patient’s verbal consent for treatment was obtained. We have de-identified the details to the extent that the patient’s identity cannot be ascertained in any way.
The patient was a woman in her 70s. According to her medical history, she had normal limb function, could live independently, and could perform regular work before the onset of symptoms. Upon admission, she complained of left hip pain persisting for 3 months with no history of trauma. Physical examination revealed unequal limb lengths, with the left lower limb shortened by 3 cm and severe restriction of movement in the left hip joint. However, the left knee joint, left ankle joint, and movement and sensation in the toes of the left foot were normal. The right lower limb showed normal joint function and sensation in the toes. Both hands and fingers exhibited normal movement and sensation with no deformities. Other limb joints, aside from the left hip joint, did not exhibit morning stiffness, swelling, or pain. For the past 2 months, the patient had been wheelchair-bound and unable to stand or walk.
The patient’s psychological attitude was characterized by a tendency to procrastinate seeking medical attention. She had not undergone any systematic treatment. There was no family history of hip pain, rheumatic diseases, diabetes, or vascular diseases. The patient was not on any chronic medications, was engaged in regular activities such as strolling in the park with family, had a normal diet, and had no other specific lifestyle habits.
After admission, the patient received clinical care to prevent complications such as aspiration pneumonia and pressure sores due to prolonged bed rest. The preliminary diagnosis was femoral neck fracture. Routine biochemical examinations, including blood analysis, urinalysis, and liver and kidney function tests; vital signs, such as blood pressure and heart rate; and immune status for diseases such as HIV, syphilis, and hepatitis, were all within normal ranges (Table 1). However, because of the lack of follow-up imaging in the previous 3 months, the patient underwent a repeat X-ray examination (Figure 1(b)), revealing complete disappearance of the femoral head.
Biochemical examination results, vital signs, intraoperative rapid leukocyte examination results, and pathological findings of the patient. All results reported were normal.

Intraoperative frozen section diagnosis (hip joint tissue): No white blood cells observed in rapid leukocyte examination, and 0–1 neutrophils observed per high-power field.
WBC, white blood cell count; RBC, red blood cell count; HGB, hemoglobin; HCT, hematocrit; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; PLT, platelet count; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; GLU, glucose; K, blood potassium; Na, blood sodium; Cl, blood chloride; Cr, creatinine; UA, uric acid; HR, heart rate; BP, blood pressure; TBIL, total bilirubin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamyl transferase; ALP, alkaline phosphatase; TBA, total bile acids; TP, total protein; ALB, albumin; IP, inorganic phosphorus; HAVAB, anti-HAV IgM (electrochemiluminescence); HBsAg, hepatitis B surface antigen (chemiluminescence); HBsAb, anti-hepatitis B surface antibody (chemiluminescence); HBeAg, hepatitis B e antigen (chemiluminescence); HBeAb, anti-hepatitis B e antibody (chemiluminescence); HBcAb, anti-hepatitis B core antibody (chemiluminescence); HCVAb, anti-hepatitis C virus antibody (chemiluminescence); HEV-IgG, anti-hepatitis E virus IgG antibody (chemiluminescence); HEV-IgM, anti-hepatitis E virus IgM antibody (chemiluminescence); anti-TP, anti-Treponema pallidum antibody (chemiluminescence); HIV Ag/Ab, HIV antigen/antibody combined test (chemiluminescence).
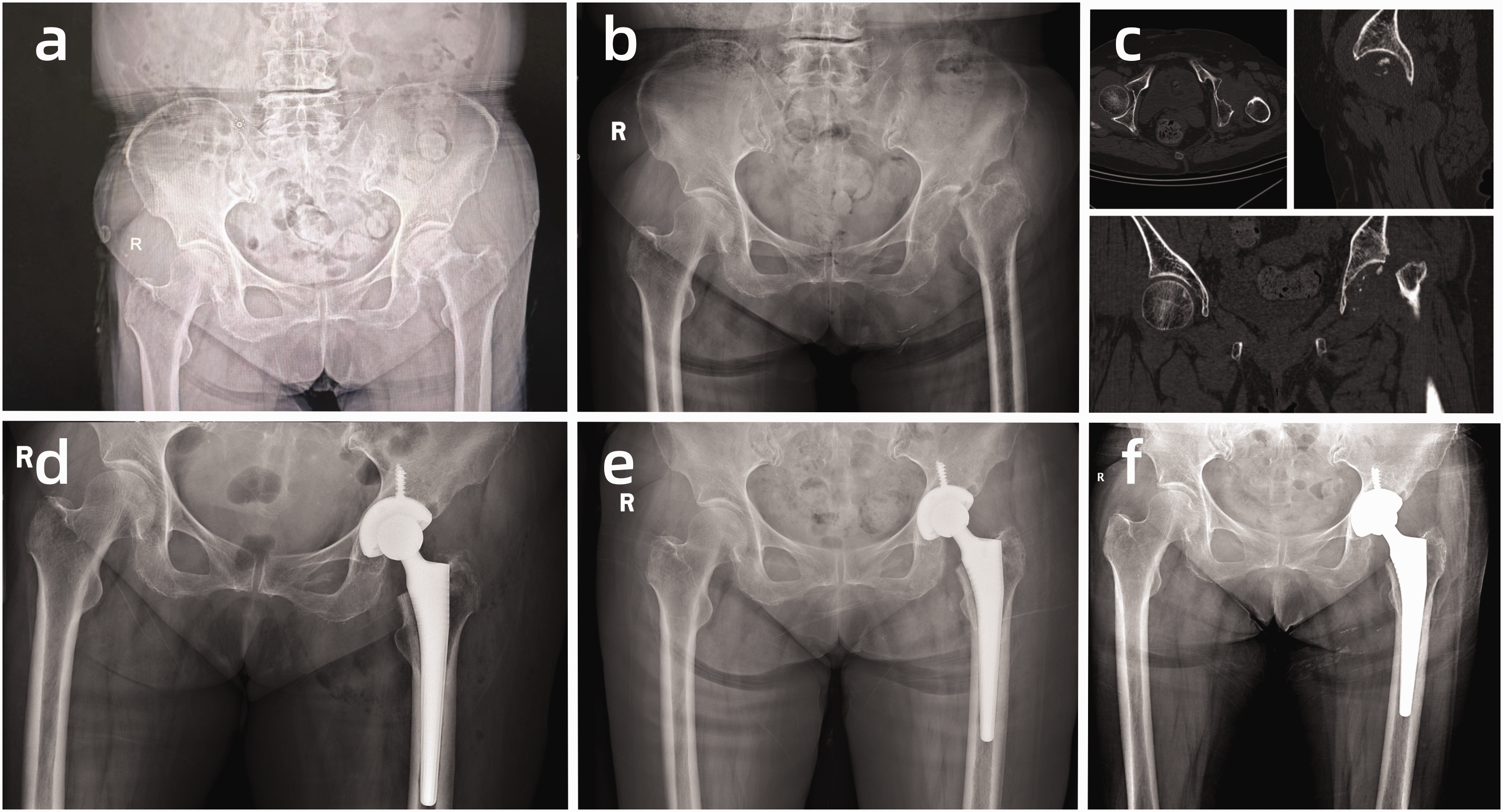
Patient’s preoperative and postoperative radiological data. (a) X-ray taken 3 months previously, when the patient first experienced hip pain. (b) X-ray at the time of admission, showing complete disappearance of the femoral head. (c) Preoperative computed tomography scan, revealing minimal residual bone. (d) X-ray image on postoperative day 1. (e) X-ray image 1 month postoperatively and (f) X-ray image 3 months postoperatively.
Detailed inquiry into the patient’s medical history revealed that she had begun experiencing hip pain 3 months previously and sought treatment in the pain management department. An X-ray examination at that time indicated a femoral neck fracture. Following consultation and information disclosure, the patient and her family opted for conservative treatment. She was discharged for self-rest and did not adhere to medical advice regarding care and exercise during the recovery period. Topical and oral analgesic medications were used, and although the patient engaged in walking and standing post-discharge, severe limitations in limb mobility and an inability to stand developed over the following 2 months, with persistent and inadequately relieved pain.
The preliminary consideration was that this situation might be related to osteoporosis, with the fracture causing fragmentation of the femoral head and neck and leading to disappearance of the femoral head through subsequent activity and absorption. However, the X-ray taken 3 months previously (Figure 1(a)) showed a relatively stable fracture and intact femoral head. This discrepancy from the initial assumption and the uniqueness of femoral head disappearance in this patient necessitated further investigation.
Further investigation involved a computed tomography scan (Figure 1(c)), confirming the disappearance of the femoral head and ruling out other fractures and femoral head migration. Bone density measurements revealed osteoporosis (Figure 2(a)). Brucellosis was excluded (the patient being an urban resident with no history of contact or consumption of contaminated food), and blood tumor markers were negative (Table 2). Rheumatoid and rheumatic factor results were within normal limits (Table 2). After comprehensive analysis by a multidisciplinary team, the ultimate cause of femoral head disappearance was determined to be a femoral neck fracture. Rapid ischemia, osteonecrosis, wear, and dissolution contributed to the absorption, leading to disappearance of the femoral head. The recommended treatment plan was total hip arthroplasty. The patient’s compromised bone quality led to the consideration of selecting a domestically produced cementless fixed hip joint prosthesis provided by AK Medical Equipment (Beijing, China). The acetabular cup prosthesis was constructed with a three-dimensionally printed bone trabecular layer, offering high initial stability and rapid bone integration. The femoral head and acetabular liner were made of ceramic and polyethylene, respectively, resulting in lower wear rates and extended longevity of the prosthesis.

Patient’s bone density and pathological examination data. (a) Results of the patient’s bone density examination, indicating severe osteoporosis in both femoral necks and (b) postoperative pathological findings of the patient’s hip joint tissues and surrounding tissues (screenshots only because of limitations in exporting images within our hospital), revealing thinning of the bone cortex, fracture of trabeculae, and localized formation of necrotic bone.
Patient’s biochemical examination data, including tumor markers and rheumatoid and rheumatic tests.

The results showed normal tumor markers (−) and normal rheumatoid and rheumatic biochemical test results.
During the surgery, it was discovered that the femoral head had completely dissolved. Intraoperative rapid pathological examination and rapid leukocyte examination showed no white blood cells (Table 1). Primary septic hip arthritis was ruled out. Postoperatively, residual tissues were obtained for pathological examination (Figure 2(b)), and joint replacement surgery was successfully performed. The postoperative rehabilitation plan included physical therapy and functional exercises. Considering the patient’s tendency to procrastinate seeking medical attention, we provided her with a specialized rehabilitation program and guidance postoperatively. Following anesthesia recovery, the patient was instructed in active and passive movements of the foot, ankle, knee, and hip joints to exercise muscle strength and promote blood circulation. On the first day postoperatively, after the first follow-up examination (Figure 1(d)), the patient began standing and gradually walking, with the standing and walking time increasing gradually each day. Because of the use of a posterior approach for the surgical incision, precautions were taken to prevent excessive flexion, adduction, and internal rotation of the affected limb to prevent postoperative joint dislocation.
At 1 month (Figure 1(e)) and 3 months (Figure 1(f)) postoperatively, follow-up X-rays showed normal walking function, well-positioned hip joint prostheses, and no signs of loosening. The pelvic and femoral bone quality was good, with no lesions. The bone cortex showed good continuity, normal trabecular patterns, and no abnormalities.
This case highlights the practical value of thorough examination, multidisciplinary analysis, accurate diagnosis, and total hip arthroplasty in patients with femoral head disappearance. The patient experienced rapid recovery of walking function postoperatively, leading to high satisfaction. Verbal informed consent for the publication of relevant data and research findings was obtained from the patient.
Discussion
Cases of femoral neck fractures combined with complete disappearance of the femoral head are extremely rare. The potential mechanisms and pathophysiology of femoral head disappearance may involve several factors. For example, interruption of the blood supply may lead to hypoxia and nutrient deficiency, causing cell death and bone tissue necrosis. 7 Difficulty in revascularization and imbalances in bone remodeling may lead to failure of the bone reconstruction and repair processes. 8 This can lead to collapse of the trabecular bone structure and, subsequently, collapse of the femoral head. 9 Specific reasons for the complete disappearance of the femoral head after a femoral neck fracture may include ischemic necrosis, chronic joint lesions, osteoporosis, and related complications. The fracture disrupts the blood supply to the femoral head, and without proper treatment, the fracture ends may fail to heal or heal in a deformed manner. This can lead to chronic joint inflammation, causing wear and tear on the bone joint surface, ultimately resulting in bone dissolution and absorption. 10 For patients with femoral neck fractures, surgical treatment is usually recommended to provide stability and promote healing. 11 This case demonstrates the significant efficacy of total hip arthroplasty in managing femoral neck fractures combined with femoral head disappearance, offering the possibility of rapid recovery and high patient satisfaction. Based on the patient’s condition and relevant research, the application of a non-cemented hip joint prosthesis and a three-dimensionally printed bone trabecular layer acetabular prosthesis is recommended. This approach offers high initial stability, facilitates rapid bone integration, and supports early postoperative mobilization while prolonging the longevity of the prosthesis. 12
Among the possible causes and scenarios leading to femoral head disappearance, femoral head disappearance may occur after femoral neck fractures. 13 Conditions such as osteoarthritis, infectious arthritis, and rheumatoid arthritis can lead to the destruction of bone and joint structures, with severe cases resulting in femoral head disappearance. Ischemic and medication-induced necrosis can lead to femoral head necrosis, and in severe cases, the femoral head may collapse or even disappear.2,4,14 Brucella bacteria can invade the skeletal system, causing inflammatory reactions in joints, bone marrow, and surrounding tissues. 15 Syphilis-induced extensive bone defects can lead to disappearance of the femoral head and neck. 16 Multiple myeloma can cause bone damage. 17 Spinal stenosis may damage the vasculature supplying the femoral head, triggering necrosis and bone loss. 18 Bone and other metastatic tumors can erode bone, causing changes and disappearance of bone structure. 19 Some bone metabolic and osteolytic diseases, such as Paget’s disease, may result in abnormal growth and morphological changes in the femoral head. 20 Gorham’s disease involves progressive and irreversible dissolution of bone tissue, leading to skeletal loss.21,22 Finally, certain rare genetic bone disorders, such as skeletal dysplasia or hereditary osteonecrosis, may cause abnormal morphology and disappearance of the femoral head. 23
Compared with previous studies on similar conditions, this case is notable for the rapid progression of femoral head disappearance, underscoring the importance of standardized diagnosis and treatment as well as the complexity of the diagnostic process. We employed comprehensive and systematic examination methods and personalized treatment plans rather than relying solely on a single examination technique. In addition, given the patient’s tendency to delay seeking medical attention, we placed special emphasis on educating the patient about the severity of the disease, the postoperative rehabilitation plan, and the importance of patient education. We provided specialized rehabilitation guidance and follow-up plans to ensure effective postoperative recovery.
The novelty of this case lies in the extremely rare occurrence of a femoral neck fracture accompanied by the complete disappearance of the femoral head. Very few reports to date have addressed this condition. This case used a novel prosthesis provided by AK Medical Corporation, which was suitable for the patient. Through comprehensive analysis by a multidisciplinary team, the cause of the femoral head disappearance was identified, and a personalized treatment plan was formulated. The detailed diagnostic and treatment process provided in this case fills a gap in the study of similar cases.
When the femoral head disappears, surgical treatment should not be pursued blindly. If patients have certain underlying conditions, especially infectious, metabolic, or osteolytic diseases, targeted treatment may not be feasible and could potentially result in surgical failure.
For patients with femoral head disappearance, a detailed medical history, physical examination, biochemical tests, and imaging assessments contribute to a comprehensive understanding of the etiology and guide personalized treatment. Specific treatment plans should be tailored based on the patient’s overall condition and underlying causes. Addressing femoral head disappearance involves several aspects, including tumor metastasis assessment and treatment planning (evaluate the severity of metastatic conditions and primary tumors to devise appropriate treatment plans), 24 joint replacement for mechanical wear or ischemic necrosis (consider joint replacement for cases involving mechanical wear or ischemic necrosis), control of infections caused by agents such as Brucella (actively manage infections and the underlying causes, particularly in cases of infectious arthritis induced by agents like Brucella), and assessment and surgical treatment for rare bone metabolic disorders and osteolytic lesions (accurately assess bone quality and the stage of osteolysis). Currently, there may not be definitive treatment plans for rare bone metabolic and osteolytic diseases, but surgical intervention remains feasible by evaluating bone quality and halting osteolysis.25,26 Total hip arthroplasty is a viable and effective treatment option for femoral head disappearance, but a thorough evaluation of the patient’s specific condition, physical fitness, and the value of surgical intervention is essential.
Conclusion
This case emphasizes that although the occurrence of complete femoral head disappearance in patients with femoral neck fractures is rare, it is extremely serious. Comprehensive examinations and multidisciplinary analyses are crucial in diagnosing complete femoral head disappearance. Personalized treatment plans and the application of innovative prostheses have significantly improved treatment outcomes. Patient education, rehabilitation guidance, and follow-up are essential for ensuring postoperative recovery. The successful management of this case provides valuable insights for the diagnosis and treatment of femoral head disappearance caused by various factors. Future research should include in-depth exploration of pathophysiological mechanisms, development of long-lasting prostheses, formulation of preventive strategies, and conduction of multicenter clinical studies.
Footnotes
Acknowledgement
The authors express their gratitude to the patient who made this work possible.
Author contributions
All authors listed have significantly contributed to the investigation, development, and writing of this article.
Conceptualization: Zhencun Cai.
Data curation: Hairui Liang, Lei Yang, Rongda Xu, Siyu Duan.
Formal analysis: Zhencun Cai, Beibei Chen.
Funding acquisition: Zhencun Cai.
Investigation: Lei Yang, Xueting Zhou, Hanfei Liu, Hang Wen.
Validation: He Zhang, Ming Sun.
Writing – original draft: Hairui Liang.
Writing – review & editing: Hairui Liang, Zhencun Cai, Beibei Chen.
All individuals are members of the surgical team.
Data availability statement
Data will be made available on request.
Declaration of conflicting interest
The authors declare that they have no conflicts of interest concerning this article.
Funding
This study was supported by the Natural Science Foundation of Liaoning Province (2024), the Liaoning Provincial Department of Education Fund Project (JYTMS20231396), and the Science and Technology Plan Project of Shenyang City (Grant no. 22-321-32-13).