
Abstract
Objective
The relationship between the surgical approach used for hemiarthroplasty and periprosthetic bone mineral density (BMD) is not well understood. We have previously described a decrease in BMD 1 year postoperatively. Here, we assessed the medium-term changes in periprosthetic BMD.
Methods
We performed a follow-up study of patients with femoral neck fracture (FNF) who underwent uncemented hemiarthoplasty using a direct lateral or anterolateral approach. Dual-energy X-ray absorptiometry (DXA) was used to evaluate the changes in BMD in 23 patients over 5 years.
Results
A mean 6% loss of total BMD occurred over 1 year, but between 1 and 5 years, BMD was restored to the baseline value. The mean total BMD in the anterolateral group had decreased by 2% after 3 months and 3% after 12 months, and increased by 2% after 5 years, vs. decreases of 7%, 8%, and 3% for the direct lateral group. Between 1 and 5 years, BMD increased in Gruen zones 2, 3, 4, 5, and 6 in both groups. There was a significantly larger increase in zone 4 in the lateral group (4%) than the anterolateral group.
Conclusion
The surgical approach affects periprosthetic BMD in patients with FNF. Furthermore, BMD is restored to the baseline value 5 years postoperatively.
Keywords
Introduction
A reduction in bone mineral density (BMD) is a common sequela of hip arthroplasty. 1 Several factors are responsible for this reduction, and periprosthetic bone loss may lead to implant loosening and late periprosthetic fracture.2–4 Previous studies have shown that the material that the stem is made of, the fixation method, and the design of the stem influence the change in periprosthetic BMD.5,6 Body mass index (BMI) and the daily activity level also appear to affect BMD around the femoral stem, 7 and some previous studies have shown an alteration in bone resorption according to the surgical approach used during the implantation of the prosthesis.8,9 The increase in knowledge regarding prosthesis design and fixation has led to longer survival of the implants used for total hip arthroplasty (THA). In particular, the use of triple-tapered polished cemented stems, 10 cemented stems in osteoporotic bone, 11 uncemented collared stems, 12 and highly cross-linked polyethylene bearings 13 have contributed to the prolongation of THA implant survival. However, the relationship between the surgical approach and periprosthetic BMD is less well understood. There have been some studies of this relationship with respect to THA,8,9 but the results have been inconsistent, demonstrating both the ongoing loss 14 and restoration of BMD 15 over the medium-to-long term. The surgical approach used may affect BMD through altered gait and loading of periprosthetic bone. These factors, together with the age-related reduction in BMD may cause a postoperative loss of periprosthetic bone density and a resulting increase in the risk of periprosthetic fracture. The incidence of periprosthetic fracture is increasing, and it is now the leading reason for revision surgery in some countries.16,17
Although the surgical approach used has been shown to affect BMD following THA, there is little knowledge regarding its influence in patients undergoing hemiarthroplasty for the treatment of femoral neck fracture (FNF). In a previous study, we compared the bone density of patients who underwent two different surgical approaches to uncemented HA and found a reduction in their total periprosthetic BMD during the following 12 months. Furthermore, the mean change in total BMD over this period was less marked in those who underwent THA using an anterolateral approach. 18 Here, we report a further study of the patients in this randomized controlled trial (the “original study”) that focused on the change in periprosthetic BMD over the medium term.
Patients and methods
Study design and sample
Original study
This was a randomized controlled trial that compared the outcomes of inserting an uncemented femoral stem using the direct lateral or modified anterolateral approach in patients with acute dislocated femoral neck fracture. 18 A subgroup analysis of periprosthetic BMD, measured using DXA, was pre-specified in the study protocol. In this study, we hypothesized that the anterolateral approach would be associated with less bone loss around the femoral stem than the direct lateral approach. Based on an a priori sample size calculation, we acquired data for 51 patients between February 2014 and March 2016 for this subgroup analysis. The mean age of the patients was 83 (70 to 90) years and they principally had American Society of Anesthesiologists (ASA) grade II or III (Table 1). They were followed for up to 12 months using DXA and clinical scores (the Harris Hip Score, Hip disability and Osteoarthritis Outcome Score, and European Quality of Life Five Dimensions questionnaire score). Thirteen patients were excluded during the original study: seven who died, five who declined to participate, and one who sustained a periprosthetic fracture. Details regarding the original study design and sample have previously been published. 18
Baseline characteristics of the included patients, categorized according to surgical approach.

Figures are numbers (percentages) unless stated otherwise. *HHS, Harris hip score estimated prior to fall. *Dorr classification. ASA, American Society of Anesthesiologists: BMI, body mass index; SD, standard deviation.
Current study
A 5-year follow-up study of the original cohort 18 was performed between February and April 2019. Ambulatory patients, who did or did not require walking aids, were between 70 and 90 years of age, and had experienced a dislocated FNF were assessed for inclusion. Those with dementia, pathologic fracture, retained hardware, and/or sepsis or local infection were excluded.
Surgery
Three consultant orthopedic surgeons who were familiar with the two approaches operated on the patients within 48 hours of their sustaining the fracture. After randomization to either the anterolateral (AL, supine position) or the direct lateral (DL, lateral decubitus position) approach, the patients had a collared Corail stem implanted (DePuy Orthopedics Inc., Warsaw, IN, USA). Spinal anesthesia was used during the procedure, and the patients received a standardized analgesic protocol and 2 g cefalotin preoperatively, followed by three 2-g doses over the next 24 hours. Low-dose heparin (enoxaparin) was prescribed for 10 days. The patients were mobile following the surgery, and there were no restrictions on weight bearing.
DXA
Technicians in the Osteoporosis unit performed the DXA measurements within 3 days of surgery. The femoral BMD for both hips was measured using a Lunar Prodigy (GE Healthcare, Chicago, IL, USA), and the findings obtained were defined as the baseline data. The measurements were repeated after 3 months, 12 months, and 5 years. To assess the standard rotation of the hip, a triangle was placed between the feet. Analysis of the DXA scans focused on seven regions of interest (ROIs), based on the Gruen zones. 19 The sizes of the seven ROIs were defined using the scanner software and adjusted according to the size of the implant. The Gruen zones were defined as follows. Zones 1 and 7 were from tip of the stem shoulder to the tip of the lesser trochanter, and zone 4 was from the tip of the stem to 20 mm distally. The midpoint between zones 1 and 4 defined the border between zones 2 and 3 laterally, and the midpoint between zones 7 and 4 defined the border between zones 5 and 6 medially. Baseline scans were performed twice and the patients were moved between each scan to estimate the precision of the measurements, expressed as the coefficient of variation (CV%). 20 The precision was recalculated at the 5-year follow-up examination, and the values obtained were comparable. Orthopedic Hip software for the GE Lunar Prodigy (GE Healthcare) was used to analyze the periprosthetic BMD in the seven Gruen zones.
Statistics
The power calculation performed prior to enrollment in the original study was based on those used in previous studies regarding bone remodeling around the femoral stem.1,6 This analysis showed that 34 patients (17 in each treatment arm) would be sufficient to detect a clinically important difference in BMD of 10% (SD 10) between the groups (80% power, two-tailed alpha of 0.05). Fifty-one patients were included, to allow for loss to follow-up.
The change in BMD (g/cm2) was calculated and the results are expressed as a percentage change with 95% confidence interval (CI) for the 3-month, 1-year, and 5-year postoperative data for all the ROIs. The mean postoperative BMDs were used as the baseline values. Standard descriptive statistics were used to assess the data for their distribution (histograms, Q-Q plots, and the Shapiro–Wilk test), and the groups were compared using Student’s t-test. The paired-samples t-test was used to compare the change in BMD between baseline and the follow-up examinations. The results were also assessed using linear mixed models for repeated measurements. We did not perform adjustments for multiple testing. P ≤ 0.05 was considered to represent statistical significance. IBM SPSS Statistics v.21 for Windows (IBM Corp., Armonk, NY, USA) was used for the statistical analysis.
Ethics and registration
The study was approved by the Regional Committee for Medical and Health Research Ethics, South East Norway, on 15 Nov 2013 (approval number 2013/1853/REK) and registered at ClinicalTrials.gov (ClinicalTrials.gov identifier NCT03753100). The reporting of this study conforms to the CONSORT statements 21 and it was performed according to the 1975 Declaration of Helsinki. All of the patients provided their written informed consent.
Results
Of the 38 patients who had been assessed after 12 months, 9 had died and 6 declined to participate, for age- or health-related reasons, leaving 23 patients (17 women and 6 men, with a mean age of 84 (70 to 90) years) who were eligible for follow-up study (Figure 1). At the time of inclusion, four patients were on anti-osteoporosis treatment. A review of the medical records revealed that 10 patients were on anti-osteoporosis treatment with a bisphosphonate (4 patients in the DL group and 6 patients in the AL group) on the date of the final follow-up appointment.
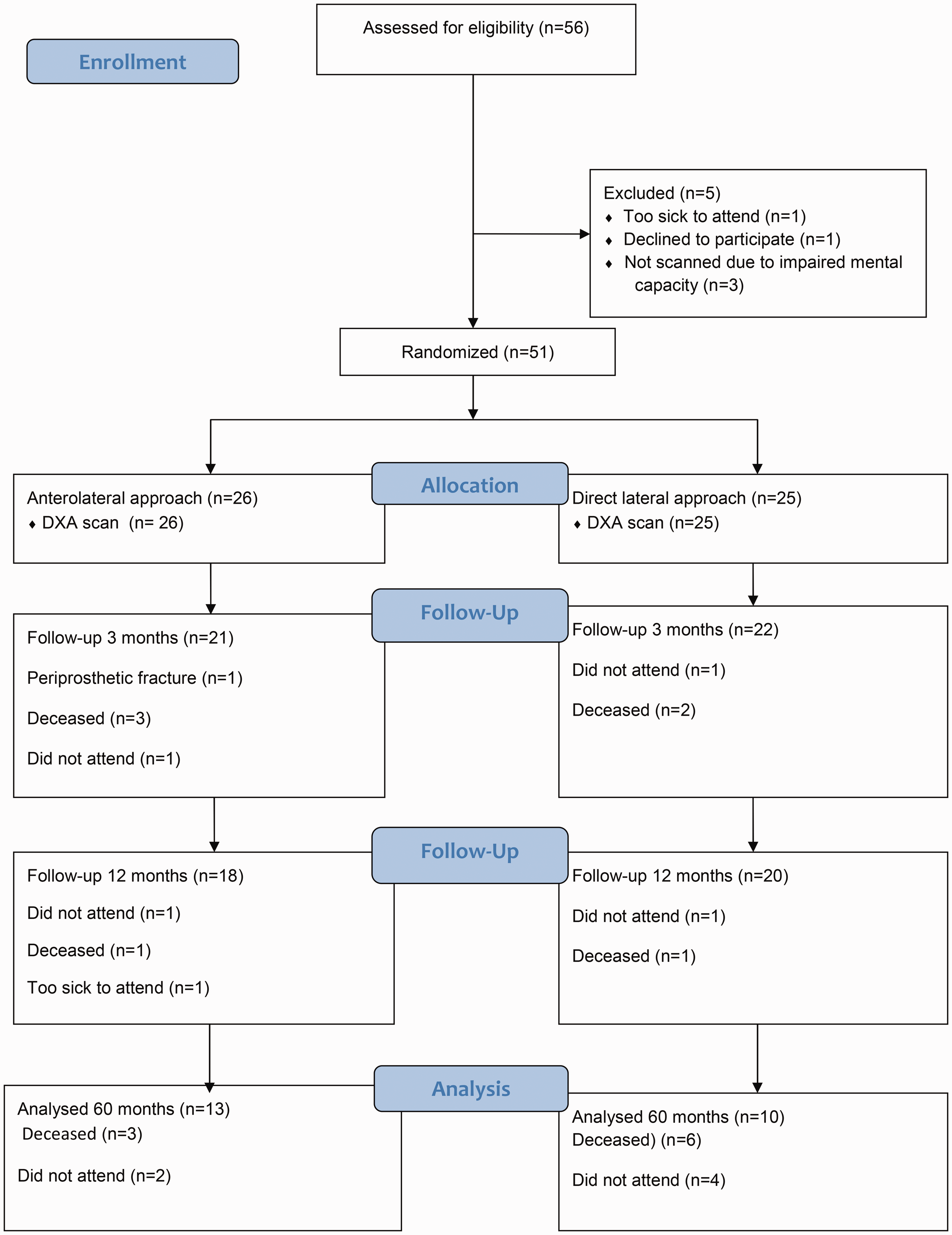
Flow chart describing the allocation of the patients.
BMD measurements
The precision of the DXA measurements of BMD (CV) has previously been reported (Table 2), and ranged from 1.2% in zone 4 to 5.5% in zone 6. 18 The precision was reassessed for this follow-up study, and was found to be similar. The two groups had similar BMDs for both the injured and non-injured hip immediately postoperatively. (Tables 3 and 4).
Precision of the dual x-ray absorptiometry measurements in the regions of interest (Gruen zones 1–7).

CV%, coefficient of variation.
Percentage changes in bone mineral density for the entire periprosthetic region and each Gruen zone from baseline in the anterolateral group.

Data are mean (interquartile range). ap < 0.05 vs. baseline (paired t-test). bexcluded, owing to heterotopic ossification.
Mean percentage changes in bone mineral density for the entire periprosthetic region and each Gruen zone from baseline in the direct lateral group.
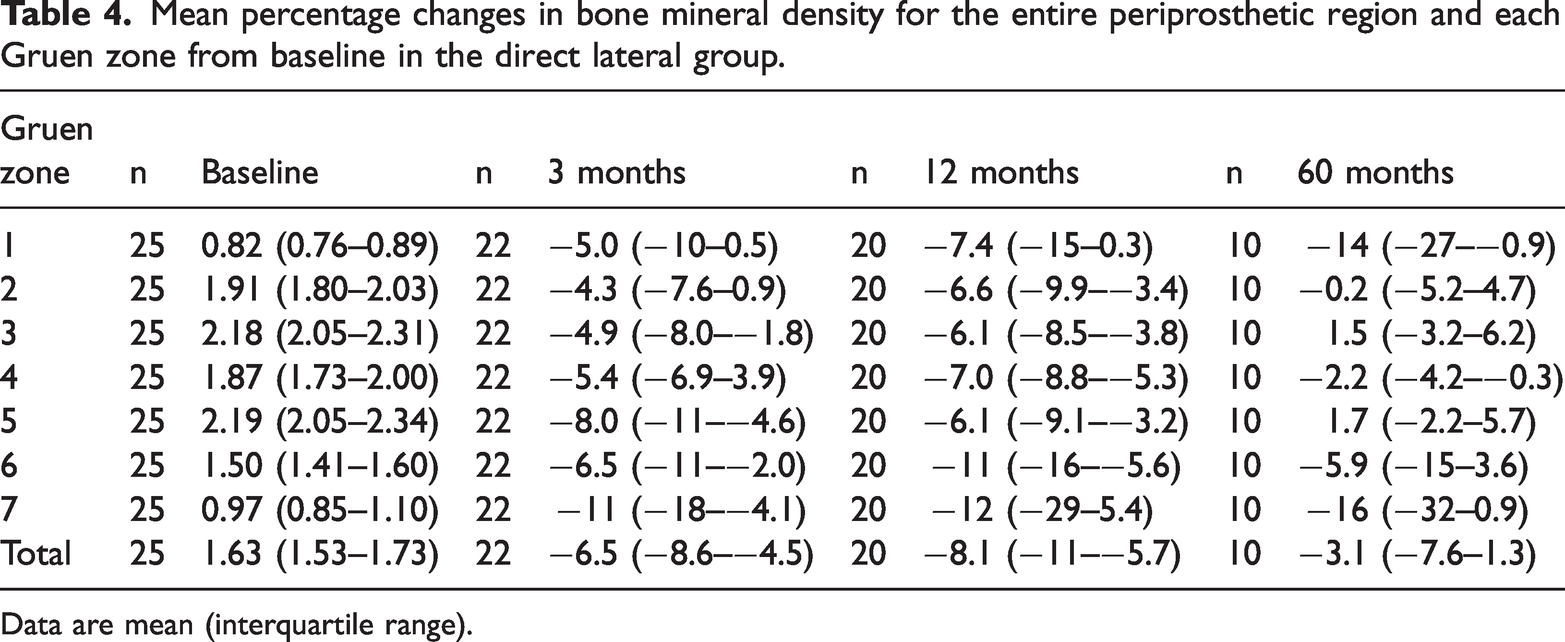
Data are mean (interquartile range).
Between baseline and 3 months post-surgery, the total BMD of the patients decreased by 4% (CI 2%–6%, p < 0.001). After 12 months, the total BMD had decreased by 6% (CI 3%–8%, p < 0.001) from baseline. However, after 5 years the total BMD had returned to the baseline value (0.0%, CI −4%–4%, p = 0.14).
The mean BMD of the AL group had decreased by 2% after 3 months and by 3% after 12 months, but had increased by 2% after 5 years (Table 3). The corresponding numbers in the direct lateral group were decreases of 7%, 8% and 3% (Table 4). There was a tendency toward an increase in total BMD between 1 and 5 years postoperatively in the two groups, but this did not reach statistical significance (Figure 2). Between 1 and 5 years postoperatively, BMD increased in Gruen zones 2, 3, 4, 5, and 6 in both groups, and there was a significantly larger increase in BMD in zone 4 in the DL group vs. the AL group (4%, CI 0.2%–7%, p = 0.038). In Gruen zones 1 and 7, BMD tended to decrease beyond 12 months in the AL group. In addition, in the AL group, BMD tended to decrease in zone 1 and increase in zone 7.

Percentage changes in total bone mineral density from baseline. Error bars represent 95% confidence intervals.
We also conducted independent sample t-tests with bootstrapped estimated p-values and CIs. These CIs were comparable to those listed in Tables 3 and 4.
Clinical results
After 5 years, the mean Harris Hip Scores of the two groups were similar (84 for the AL group and 83 for the DL group).
Discussion
The change in BMD that occurs around a femoral stem is an area of continuing interest because bone loss increases the risk of periprosthetic fracture. The incidence of periprosthetic fracture is increasing and it is now the principal reason for revision surgery. Surgery-induced bone remodeling is the result of changes in biomechanics and the trauma to the bone. 22 The etiology is multifactorial, and previous studies have shown that the fixation technique used, the design of the stem, the surface coating, and the surgical approach used affect periprosthetic bone density.5,8,23 Alterations in the transmission of forces to the surrounding bone results in adaptive remodeling and the resorption of bone, which is known as stress-shielding. Karachalios et al. have previously shown that stress-shielding is one of the most important factors influencing postoperative bone resorption following cementless hip arthroplasty. 24 However, the phenomenon of stress-shielding has not been extensively characterized in patients undergoing hemiarthroplasty because of femoral neck fracture.
Several previous studies have shown that there is a loss of periprosthetic bone following the implantation of uncemented stems for the treatment of THA, especially in Gruen zones 1 and 7. 23 Because these were studies of THA, the results are not directly applicable to femoral stems that are inserted because of FNF. In the original study, we showed a reduction in total BMD between baseline and 12 months. 18 The mean total periprosthetic BMD had decreased by 4% (CI 2%–6%) at 3 months and by 6% (CI 3%–8%) at 12 months. After 5 years, the reduction in mean total BMD had disappeared (change from baseline: 0%, CI −4% to 4%) and bone density had been restored around the femoral stem in Gruen zones 2, 3, 4, 5, and 6, whereas the bone density was lower in zones 1 and 7. In particular, the change in mean BMD was significant larger in Gruen zone 4 between 1 and 5 years when the DL approach was used (4%, CI 0.2%–7%). According to Wolff’s law, a rigid implant, through-stress shielding, transmits a load from the proximal part of the femur to the cortical bone of the diaphysis. 25 We found that there was a significant increase in BMD in Gruen zone 4, a tendency toward an increase in BMD in zones 2, 3, 5, and 6, and a tendency toward a decrease in BMD in zones 1 and 7. In zones 1 and 7, BMD tended to decrease beyond 12 months, to decrease in zone 1 and to increase in zone 7 in the AL group. Although it was not statistically significant, the trend toward a higher BMD in Gruen zone 7 associated with the AL approach vs. the DL approach could be related to the surgical approach used. The detachment of the gluteal muscles that is involved in the lateral approach, and possibly the alteration to endosteal perfusion in the greater trochanteric region (Gruen zone 7), might explain the differences in BMD associated with the two approaches. Perka et al. have published a comparison of the changes in periprosthetic BMD that occur in patients who undergo surgery using the DL or modified AL approach. In their retrospective study of patients who underwent THA, they found highly significant differences in Gruen zones 1, 2, 5 and 7 that favored the modified anterolateral approach. In addition, in a randomized controlled trial that compared the posterior approach and the DL approach in THA, Hjorth et al. found a significant difference in BMD loss that favored the posterior approach, further implying that the surgical approach used affects femoral BMD. 26
Uncemented stems have frequently been used in HA for the treatment of FNF, although the proportion of patients treated using these implants in Norway has fallen significantly. In 2013, uncemented stems were used in 30% of cases of HA, but only 3% in 2022. The principal reason for this change is the greater fracture risk associated with the use of uncemented stems in patients with FNF. Fernandez et al. showed a significant higher risk of periprosthetic fracture in a randomized controlled trial of patients who underwent surgery using an uncemented HA vs. a cemented HA. 27 McGraw et al. performed a retrospective follow-up study of 346 patients who had an uncemented HA implanted, found a significant higher risk of periprosthetic fracture vs. those who had a cemented HA implanted, and found that the mean timing of fracture was 2 years postoperatively. 28 Langslet et al. performed a 5-year follow-up study which showed that a significant higher risk of periprosthetic fracture was associated with uncemented HA. 4 In the original study, we found less periprosthetic bone loss following surgery using the AL approach to the hip than the DL approach after 12 months. However, after 5 years, the periprosthetic BMD had been restored to the baseline values in both groups.
The changes in BMD identified in this follow-up study, together with similar findings of previous medium- and long-term follow-up studies of the use of uncemented stems in THA, might at least in part explain the greater short-term risk of periprosthetic femoral fracture when uncemented stems are implanted. We found that there was greater bone loss in the DL group than in the AL group 3 months and 1 year following surgery, which indicates that the surgical approach to the hip joint affects the risk of periprosthetic BMD. However, the present results should be interpreted with caution, owing to the small sample size, which meant that we could not perform adjustments for multiple testing. Furthermore, only 23 patients were re-evaluated after 5 years, and the study protocol excluded patients with dementia. Therefore, changes in clinical practice that are based on the present results are not warranted. Larger studies are needed to clarify the relationship between the surgical approach used and the changes in BMD associated with HA for the treatment of FNF.
Footnotes
Acknowledgements
The investigators thank the patients and their families for their participation in the trial. We also thank the medical staff at the Department of Rheumatology, Sorlandet Hospital Kristiansand, Norway, for performing the DXA examinations.
Author contributions
SHU drafted the manuscript. All the authors contributed to the study design and the interpretation of the data and results, and reviewed and approved the final version of the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.