
Abstract
Objective
To compare the clinical outcomes of primary metal-on-metal total hip replacement (MoM-TR) converted to uncemented total hip replacement (UTR) or cemented total hip replacement (CTR) in patients with femoral neck fractures (AO/OTA: 31B/C).
Methods
Patient data of 234 UTR or CTR revisions after primary MoM-TR failure from March 2007 to January 2018 were retrospectively identified. Clinical outcomes, including the Harris hip score (HHS) and key orthopaedic complications, were collected at 3, 6, and 12 months following conversion and every 12 months thereafter.
Results
The mean follow-up was 84.12 (67–100) months for UTR and 84.23 (66–101) months for CTR. At the last follow-up, the HHS was better in the CTR- than UTR-treated patients. Noteworthy dissimilarities were correspondingly detected in the key orthopaedic complication rates (16.1% for CTR vs. 47.4% for UTR). Statistically significant differences in specific orthopaedic complications were also detected in the re-revision rate (10.3% for UTR vs. 2.5% for CTR), prosthesis loosening rate (16.3% for UTR vs. 5.9% for CTR), and periprosthetic fracture rate (12.0% for UTR vs. 4.2% for CTR).
Conclusion
In the setting of revision of failed primary MoM-TR, CTR may demonstrate advantages over UTR in improving functional outcomes and reducing key orthopaedic complications.
Introduction
Because of elevated revision rates, the employment of metal-on-metal total hip replacement (MoM-TR) has gradually decreased in recent years.1–4 Prosthesis revision triggered by the use of MoM bearings remains a concerning problem.5–7 Bone mass loss may be due to massive osteolysis initiated by adverse reaction to metal debris, which potentially leads to failed MoM-TR and the need for conversion. 8 This increasing rate of failed MoM-TR has inevitably led to an escalation in the performance of uncemented total hip replacement (UTR) or cemented total hip replacement (CTR).8–10 Many authors have reported key orthopaedic complications after converting MoM-TR to UTR or CTR; however, a consensus has not been reached, mainly because of the limited follow-up time among these studies.3,5,7,10–12
The midterm clinical outcomes of converting original MoM-TR to UTR or CTR remain unclear. 11 Therefore, we performed a retrospective review to evaluate the outcomes of primary MoM-TR conversion to UTR or CTR in patients with femoral neck fractures (FNFs) (AO/OTA: 31B/C).
Materials and methods
Patients
This study was approved by the Investigational Review Board (IRB) of The First Affiliated Hospital, Sun Yat-sen University (IRB19-3232), and the requirement for informed consent was waived by the IRB because of the retrospective nature of the study. In total, 326 patients (326 revisions) who had undergone UTR or CTR after the first MoM-TR from March 2007 to January 2018 were retrospectively identified from our institutional database. All patients had FNFs (AO/OTA: 31B/C) and underwent primary MoM-TR (Zimmer Biomet, Warsaw, IN, USA) with subsequent conversion to UTR (CORAIL; DePuy Synthes, Raynham, MA, USA and REFLECTION uncemented; Smith & Nephew, London, UK) or CTR (Exeter; Stryker, Kalamazoo, MI, USA and Elite; Stryker). Each revision was performed by three high-volume surgeons (W.Y., X.Z., and Y.X.) as previously described. 13 The indication for revision was primarily based on the presence of continuous symptomatic hip or progressive symptoms regardless of normal imaging findings or whole blood metal concentrations. The major exclusion criteria were cachexy, absence of baseline information (such as injury mechanism or Harris hip score (HHS) prior to surgery), dyskinesia or akinesis, cancer, serious medical or infectious disease, multiple lesions, allergy to anaesthetics, and psychosomatic disorders.
Clinical outcomes, including the HHS and key orthopaedic complications (re-revision, prosthesis loosening, periprosthetic fracture, and dislocation), were collected in accordance with a standard protocol at each follow-up point (3, 6, and 12 months following conversion and every 12 months thereafter).
Statistical analysis
The definition of revision in this study was removal of the entire prosthesis. The definition of loosening was based on prior descriptions.8,14 Comparison of continuous variables was performed using Student’s t-test for normally distributed variables and the Mann–Whitney U test for non-normally distributed variables. Comparison of categorical variables was performed using the chi-square test or Fisher’s exact test. Each statistical analysis was executed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). A p value of ≤0.05 was considered statistically significant.
Results
In total, 234 patients (234 revisions) who underwent primary MoM-TR conversion to UTR or CTR met the inclusion criteria and were identified for study eligibility (UTR, n = 116; CTR, n = 118). The study flow chart is shown in Figure 1. A detailed summary of the patients’ characteristics is shown in Table 1. The median interval from primary MoM-TR to failure was 4.3 (1.2–6.5) years for UTR and 4.4 (1.1–6.4) years for CTR. At the time of analysis, the median follow-up was 84.12 (67–100) months for UTR and 84.23 (66–101) months for CTR.

Flow diagram demonstrating methods to evaluate the outcomes of UTR versus CTR following initial MoM-TR in patients with FNFs (AO/OTA: 31B/C).
Baseline data.

Data are presented as n, n (%), mean ± standard deviation, or median (range).
UTR, uncemented total hip replacement; CTR, cemented total hip replacement; BMI, body mass index; BMD, bone mineral density; FNFs, femoral neck fractures; MoM-TR, metal-on-metal total hip replacement; ASA, American Society of Anesthesiologists; HHS, Harris hip score.
Functional outcomes
At the final follow-up, the mean HHS was 79.18 ± 11.12 and 84.32 ± 10.35 in the UTR and CTR group, respectively. The HHS showed no difference between the two groups at either 3 or 6 months following revision. From 1 year following revision to the last follow-up, the HHS was better in the CTR than UTR group (p < 0.05) (Table 2).
Functional outcomes.

Data are presented as mean ± standard deviation.
*Statistically significant.
UTR, uncemented total hip replacement; CTR, cemented total hip replacement; HHS, Harris hip score.
Radiological outcomes
Fifty-five (47.4%) key orthopaedic complications were verified in the UTR group versus 19 (16.1%) in the CTR group. Of the 55 complications in the UTR group, there were 12 (10.3%) cases of re-revision, 19 (16.3%) cases of prosthesis loosening, and 14 (12.0%) cases of periprosthetic fractures. Of the 19 complications in the CTR group, there were 3 (2.5%) cases of re-revision, 7 (5.9%) cases of prosthesis loosening, and 5 (4.2%) cases of periprosthetic fractures (Table 3). The re-revision rate significantly differed at the last follow-up (10.3% for UTR vs. 2.5% for CTR, p = 0.015). No significant difference was observed in the rate of dislocation between the two groups. The median interval between revisions was 3 (1.4–3.5) years for UTR and 3 (1.2–3.6) years for CTR.
Midterm radiological outcomes.
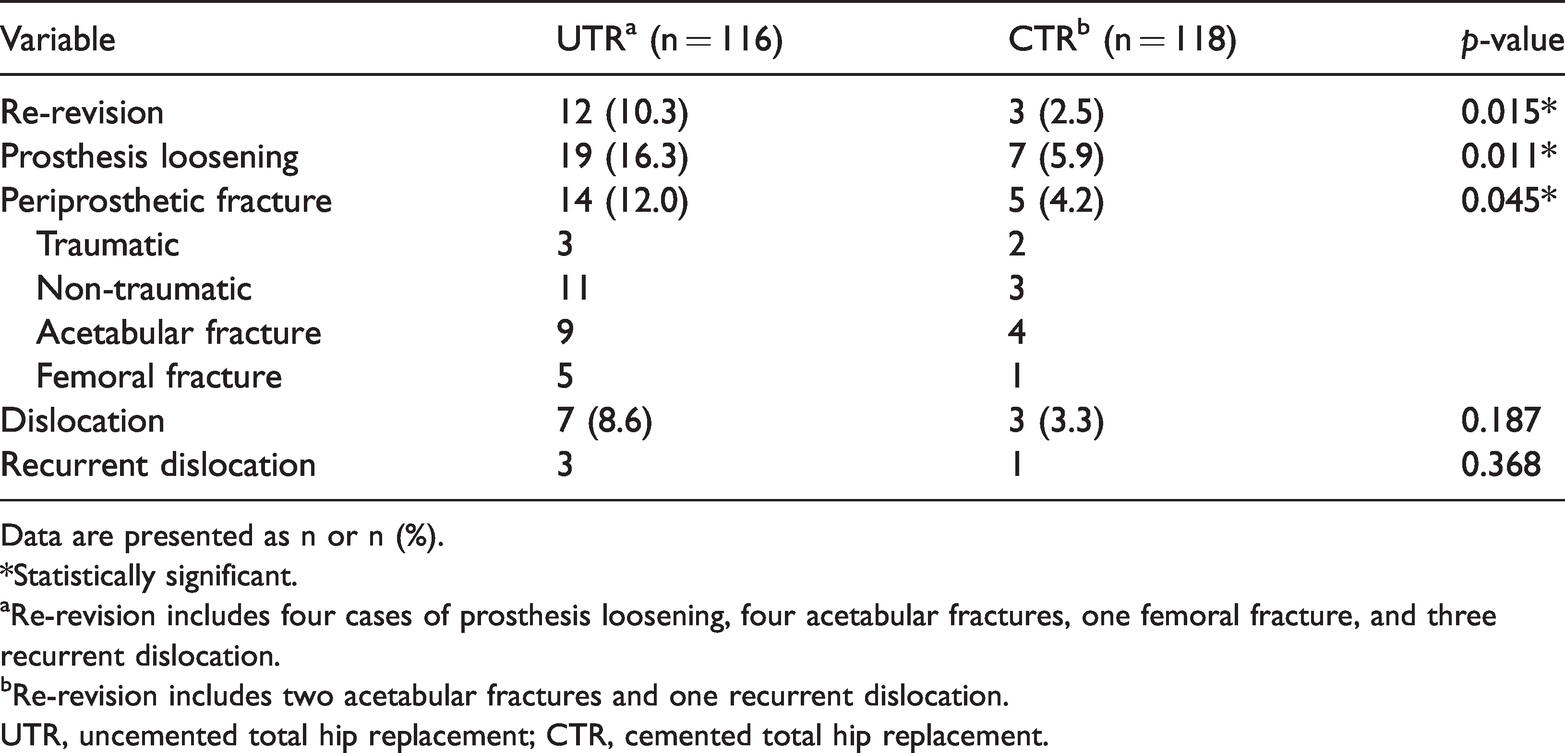
Data are presented as n or n (%).
*Statistically significant.
aRe-revision includes four cases of prosthesis loosening, four acetabular fractures, one femoral fracture, and three recurrent dislocation.
bRe-revision includes two acetabular fractures and one recurrent dislocation.
UTR, uncemented total hip replacement; CTR, cemented total hip replacement.
Discussion
Our analysis provides evidence that primary MoM-TR conversion to CTR may result in a better HHS and fewer key orthopaedic complications than conversion to UTR in patients with FNFs (AO/OTA: 31B/C). The present analysis of revision MoM-TR in an Asian population with a mean 7-year follow-up appears to be the largest-sample review to date.
The concentration of released metal ions triggered by MoM bearings is the basis for instigating biological effects, particularly immune effects.5,8 The presence of these ions mainly produces inflammatory factors by activating macrophages with simultaneous release of tumour necrosis factor, inducing osteolytic reactions and causing key orthopaedic complications.3,7,14 The concentration of cumulative ions poses a great obstacle to successful UTR or CTR.7–11 Patients exposed to higher levels of such metal ion environments have significantly reduced immune cell counts. 7 The metal ions released by the MoM bearings can form metal–protein complexes and delay cell regulatory responses, thereby triggering prosthesis-related hypersensitivity reactions.11–14 Eventually, the tissue surrounding the MoM bearing is attacked.7,14 This situation is difficult to avoid in patients undergoing MoM-TR. To overcome the challenges posed by MoM-TR, the transmission of mechanical forces on UTR may be forced to change.15–17 UTR exacerbates bone destruction and ultimately results in the need for conversion.17–19 Crawford et al. 8 performed 203 revisions following failed MoM-TR with a mean 4.2-year follow-up and showed that the massive soft tissue deformation around the endoprostheses triggered by MoM-TR is thorough and pervasive, and loosening is the instigator of frequent reoperations, predominantly in patients with a pseudotumor prior to revision. Lainiala et al. 15 evaluated 3013 cases of MoM-TR and reported that these patients will undergo reoperation within a short time. Grechenig et al. 16 implied that the low stability of the prosthesis induced by the destruction of bone tissue is the direct instigator of the frequent revision of MoM-TR.
CTR can increase the contact between the prosthesis–bone interface, which can achieve long-term stability of the prosthesis.4,20 It can also promote the growth of bone tissue into the prosthesis, which in turn improves the bonding strength between the prosthesis and the medullary cavity; moreover, it can preserve bone mass while avoiding the prosthesis loosening instigated by MoM-TR.12,14 The lower occurrence of the edge contact phenomenon in CTR can maintain the normal lubrication mechanism between the joints and reduce the amount of wear.11,17 With the development of biomaterials, research on CTR has received increasing attention from investigators.
The outcome of the revision is significantly constrained by the motivation for the revision.4,7 Revision after UTR or CTR is relatively rare, whether primary or secondary TR.11,15 Many reports have verified that the high tendency for the key orthopaedic complications is associated with UTR.16,19 A possible explanation for this circumstance might be the excessive stress concentration on the fracture blocks for UTR.20,21 However, CTR is associated with fewer key orthopaedic complications; this is primarily due to its ability to cope with the instability of the prosthesis initiated by MoM-TR with a strong riveting force, thus cutting off the instability of the prosthesis at its source.1,4,17
This study has a few limitations. First, retrospective analyses have inherent drawbacks. Nonetheless, our outcomes are principally quantitative data. Additionally, the presence of few noteworthy distinctions in patient characteristics may have largely circumvented the detrimental impact of the retrospective analysis on our results. Second, unexposed comorbidities may interfere with the results. Third, the fact that the patients were treated in different periods may have also influenced the results.
In conclusion, the results described in this analysis show that CTR may have more advantages in improving the HHS and reducing the key orthopaedic complications when compared with conversion with UTR. Hence, patients with FNFs (AO/OTA: 31B/C) who were initially managed using MoM-TR tend to be more suitable for conversion using CTR than UTR. Future studies are required to clarify whether our findings can be sustained over a longer follow-up period.