
Abstract
Objective
This study was performed to compare the clinical outcomes and performance of the collum femoris-preserving (CFP) stem (Waldemar Link GmbH & Co., Hamburg, Germany) and the Tri-Lock stem (DePuy Orthopaedics, Warsaw, IN, USA) in terms of femoral offset (FO) and leg length reconstruction.
Methods
Clinical and radiographic data of patients who underwent total hip arthroplasty with either a CFP stem or Tri-Lock stem from January 2016 to March 2017 were compared (65 and 57 patients, respectively). The Harris hip score and Western Ontario and McMaster Universities Osteoarthritis Index were recorded. The FO, femoral vertical offset, and neck–shaft angle were measured at the last follow-up. The occurrence of dislocation and periprosthetic fracture during the follow-up period was recorded.
Results
The CFP stem induced significantly more FO than did the Tri-Lock stem on the operated side than contralateral side (3.63 ± 4.28 vs. 0.83 ± 5.46 mm). Significantly fewer patients had a >5-mm decrease in FO on the unaffected side in the CFP stem group (n = 1) than Tri-Lock stem group (n = 10).
Conclusion
Both stems similarly improved hip function and reconstructed the leg length, but the CFP stem was superior to the Tri-Lock stem in reconstructing FO.
Keywords
Introduction
Increasing numbers of young, active patients are undergoing total hip arthroplasty (THA) because of its high success rate and good clinical results. Physicians are striving to improve surgical outcomes and prosthesis longevity while making future revision surgeries simpler.1,2 In the last few years, the use of short-stem cementless bone-sparing hip prostheses has gradually increased worldwide. 3 In general, short cementless bone-sparing stems are especially suitable for young, active patients. Pipino introduced the collum femoris-preserving (CFP) stem in the 1980s and evaluated it in several studies. 4 The CFP stem is a curved short stem that requires osteotomy under the femoral head for total hip replacement. 5 The CFP stem preserves the trabecular system of the metaphyseal cancellous bone, allowing a more even distribution of the physiological load along the diaphysis, and the blood supply to the preserved femoral neck can increase bone ingrowth. 6
In THA, restoration of the femoral offset (FO) and leg length of the hip joint is important to ensure good joint stability and extension of the prosthesis life span. 7 A previous study showed that the CFP stem effectively restores FO and optimizes biomechanical properties. 8 However, another study comparing the CFP stem with the ribbed stem demonstrated that the CFP stem was more likely to cause an increase in the leg length and the occurrence of periprosthetic fractures. 9 Klein et al. 10 showed that both the CFP stem and the Corail stem (DePuy Orthopaedics, Warsaw, IN, USA) had similar hip function scores, but they did not evaluate the FO or leg length. Thus, whether femoral neck-preserving hip prostheses perform better than traditional neck implants that require resection remains unclear. Most studies to date have compared CFP stems with conventional long stems; however, no published studies have compared CFP stems with straight short stems.
Therefore, this study was performed to compare the clinical outcomes and performance of the CFP curved short stem (Waldemar Link GmbH & Co., Hamburg, Germany) and the Tri-Lock straight short stem (DePuy Orthopaedics) in terms of FO and leg length reconstruction. Several studies have shown good clinical results with Tri-Lock stems.11,12
Methods
Patients
In this retrospective cohort study, we reviewed patients who had undergone THA from January 2016 to March 2017. The inclusion criteria were no history of other unilateral hip replacement procedures, the presence of femoral head necrosis or hip osteoarthritis, and treatment of one side by hip arthroplasty with a healthy hip on the other side. The exclusion criteria were severe structural destruction of the affected hip joint that could not be measured radiographically, lack of timely follow-up or missing data, and other femoral abnormalities, osteoporosis, or hyperthyroidism. The patients included in the study underwent THA using either a cementless CFP short stem (Waldemar Link GmbH & Co.) with a titanium-coated press-fit metal cup (Waldemar Link GmbH & Co.) or using a cementless Tri-Lock short stem (DePuy Orthopaedics) with a titanium-coated press-fit metal cup (DePuy Orthopaedics). Both stems were short stems with the same indications for treatment; the main difference was that the CFP stem allowed preservation of the femoral neck and the patient could choose which prosthesis to use. The local review board approved this study. Because this was a retrospective study and all patient information was deidentified before analysis, informed consent was not required. All hip replacement surgeries were performed by a single senior surgeon.
Clinical evaluation
All patients agreed to enter the arthroplasty registry and were followed up clinically and radiographically on an annual basis. At each follow-up visit, the patients underwent measurement of the Harris hip score (HHS) and Western Ontario and McMaster University Osteoarthritis Index (WOMAC) score.
Imaging evaluation
All patients underwent standardized preoperative and postoperative follow-up anteroposterior pelvic radiographs. The distance between the patient and the X-ray tube was 90 cm. The anteroposterior radiograph was taken with the patients in a standing posture with double support and the foot spacing equal to the shoulder width while performing a slightly inward (15°) bilateral tiptoe stance. At the last follow-up, radiographic measurements were performed using standardized anatomical landmarks. FO was measured as the vertical distance between the center of rotation of the femoral head and the long axis of the femur (Figure 1). 13 The leg length discrepancy and femoral vertical offset (FVO) were both measured as the vertical distance between the inter-teardrop line and the medial-most visible point on the lesser trochanter (Figure 1), and FVO was used to represent the leg length condition.14,15 The neck–shaft angle (NSA) was measured as the angle between the long axis of the femoral shaft and the medial and inferior aspects of the axis of the femoral neck (Figure 1). The difference between the two groups before and after surgery was calculated as follows: after surgery − before surgery. The difference between the two groups after surgery and on the contralateral side was calculated as follows: after surgery − contralateral side. The difference between the two groups after FO and on the contralateral side was divided into three subgroups: <−5 mm, −5 to 5 mm, and >5 mm. The difference between the two groups after FVO and on the healthy side was divided into two subgroups: −10 to 10 mm and >10 mm (no patient <−10 mm). All measurements were performed by two senior operators, neither of whom was the surgical operator.
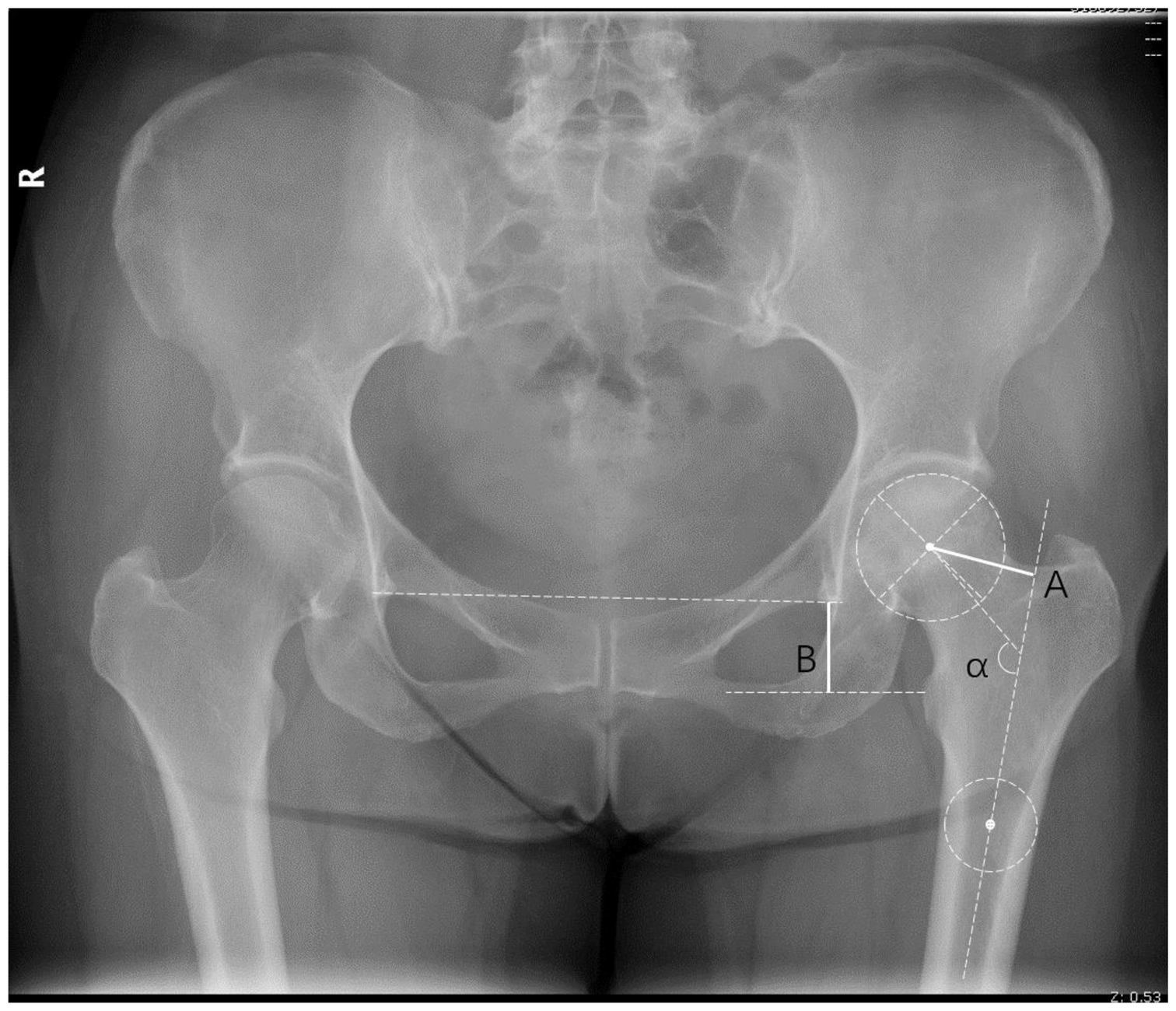
Imaging measurements based on anatomical landmarks. Femoral offset (solid line A) is the vertical distance between the center of rotation of the femoral head and the long axis of the femur. Femoral vertical offset (solid line B) is the vertical distance between the inter-teardrop line and the most medial visible point on the lesser trochanter. The neck–shaft angle (α) is the angle between the long axis of the femoral shaft and the medial and inferior aspect of the axis of the femoral neck.
The clinical outcomes observed in this study were the HHS and WOMAC score before surgery, 1 year after surgery, 2 years after surgery, and at the last follow-up visit in both groups; operation time; blood loss; and occurrence of dislocation and periprosthetic fracture during follow-up. The radiographic outcomes were the FO, FVO, and NSA preoperatively and at the last follow-up.
Procedure
The preoperative plan was to use an X-ray template to measure the size of the implant used and select the appropriate cutting position. All surgeries were performed by the same group of surgeons via a posterolateral approach. Briefly, after hip dislocation, a subcapital osteotomy was performed with the CFP stem (the Tri-Lock stem osteotomy was performed at the base of the femoral neck). The acetabulum was exposed, and an acetabular component was implanted. The CFP stem or Tri-Lock stem was implanted after reaming of the diaphysis using a reamer. Finally, a ceramic femoral head was used, and the joint was reduced. The patient was allowed to attempt full weight bearing on the second postoperative day. The mean shell size was 49.87 ± 2.44 mm (range, 44–56 mm) with no difference between the groups. Either ceramic liners or highly cross-linked polyethylene liners were used. Ceramic heads were used in all patients.
Statistical methods
Continuous variables are reported as mean ± standard deviation and categorical variables as count and percentage. Categorical variables were compared between the two groups using the chi-square test or Fisher’s exact test, as appropriate. Continuous variables were compared using Student’s
Results
General information
In total, 356 patients were initially reviewed, and 122 patients were finally included (65 in the CFP stem group and 57 in the Tri-Lock stem group). Ceramic liners were used in 47 patients in the CFP group and 43 patients in the Tri-Lock group, and highly cross-linked polyethylene liners were used in 18 patients in the CFP group and 14 patients in the Tri-Lock group; all patients had ceramic heads. All patients were followed up for >2 years. The mean age of the patients in the CFP and Tri-Lock groups was 51.59 ± 13.02 and 52.89 ± 15.37 years, respectively (range, 20–80 years), with no difference between the groups. The mean follow-up time was 31.30 ± 4.05 months (range, 24–42 months), with no difference between the groups. Sixty-six patients were male and 56 were female, with no difference between the groups. The body mass index, operative time, and blood loss volume were similar between the two groups, with no significant difference. Table 1 shows that all patients underwent preoperative, postoperative, and final follow-up radiographic examinations. None had complications of prosthesis loosening, periprosthetic infection, or periprosthetic fracture during follow-up. None underwent revision THA. One patient in each group developed hip dislocation, with no difference between the groups. No patients in either group sustained a periprosthetic fracture during surgery. Figures 2 and 3 show two representative patients with a CFP stem and Tri-Lock stem, respectively.
General information.
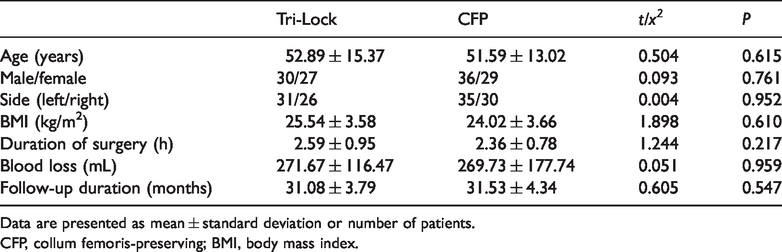
Data are presented as mean ± standard deviation or number of patients.
CFP, collum femoris-preserving; BMI, body mass index.
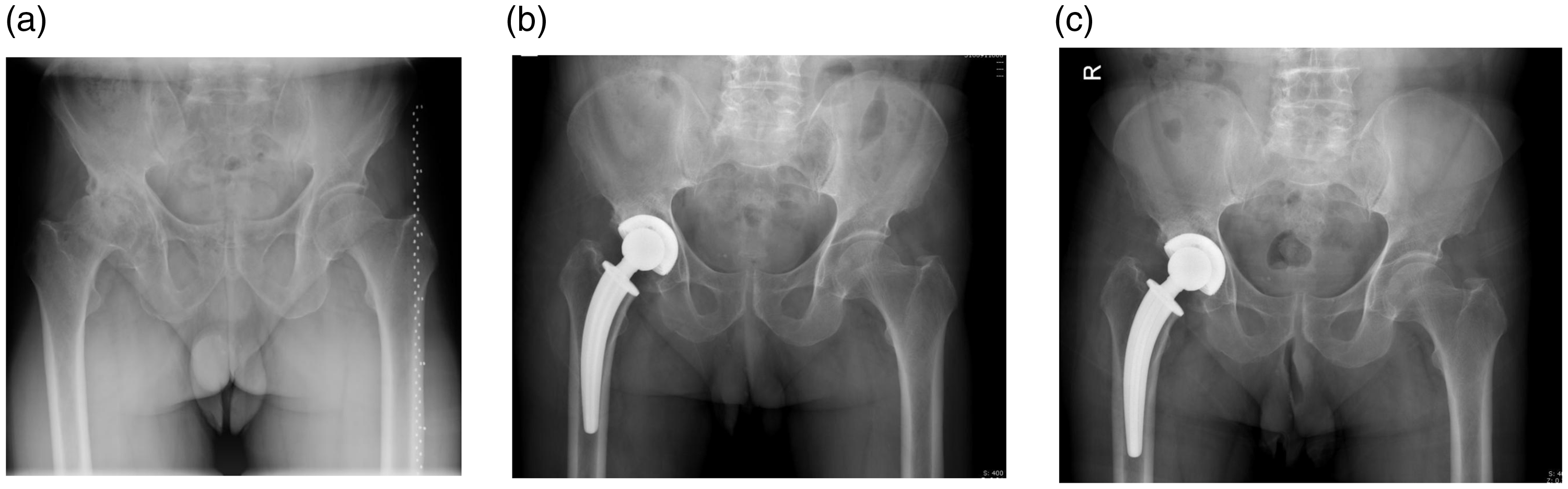
A patient with a collum femoris-preserving stem. (a) Preoperative radiograph. (b) Early postoperative period (3 months).(c) Last follow-up measurement (2 years).

A patient with a Tri-Lock stem. (a) Preoperative radiograph. (b) Early postoperative period (2 months). (c) Last follow-up measurement (1 year).
Intraobserver and interobserver reproducibility
Twenty patients were randomly sampled to test the intraobserver and interobserver reproducibility, and each measurement was independently made and repeated after 1 week. All intraclass correlation coefficients, which were used to evaluate reproducibility, were >0.9 in this study.
Imaging evaluation
In the Tri-Lock stem group, both FO and FVO were significantly greater after than before surgery (P < 0.01), but no significant difference in the NSA was found before and after surgery. The results were similar between the CFP and Tri-Lock stem groups, with a significant increase in the FO and FVO after surgery (P < 0.01) and no significant difference in the NSA, as shown in Tables 2 and 3, respectively.
Preoperative and postoperative imaging evaluation results of the Tri-Lock stem.

Data are presented as mean ± standard deviation.
FO, femoral offset; FVO, femoral vertical offset; NSA, neck–shaft angle.
Preoperative and postoperative imaging evaluation results of the CFP stem.
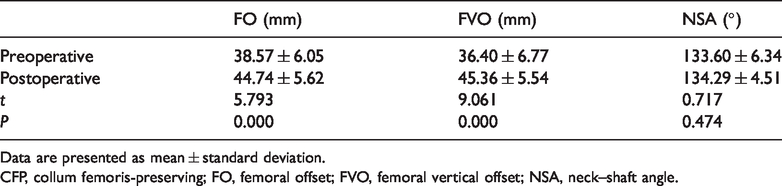
Data are presented as mean ± standard deviation.
CFP, collum femoris-preserving; FO, femoral offset; FVO, femoral vertical offset; NSA, neck–shaft angle.
Compared with the healthy side, FO increased by 0.83 ± 5.46 mm in the Tri-Lock stem group and by 3.63 ± 4.28 mm in the CFP stem group postoperatively, with a significant difference between the groups (P = 0.003). In both groups, the postoperative FVO was greater than that on the contralateral side; however, no significant difference was found between the groups, as shown in Table 4.
Difference in postoperative and contralateral imaging evaluation between the two groups.

Data are presented as mean ± standard deviation.
CFP, collum femoris-preserving; FO, femoral offset; FVO, femoral vertical offset.
No significant difference was found in the postoperative and contralateral FVO changes between CFP and the Tri-Lock stem groups. A <−5-mm change in FO occurred in 2 of 65 (3.1%) patients in the CFP stem group and in 10 of 57 (17.5%) patients in the Tri-Lock stem group, with a significant difference between the groups (P = 0.007) (Table 5).
Differences in FVO and FO changes between the two subgroups.
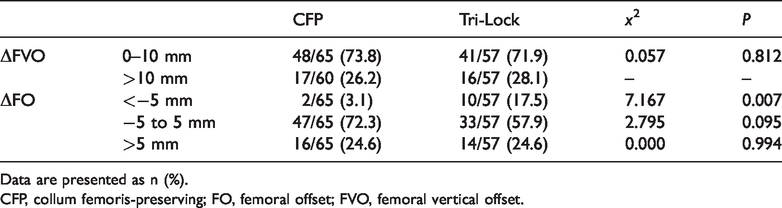
Data are presented as n (%).
CFP, collum femoris-preserving; FO, femoral offset; FVO, femoral vertical offset.
Clinical evaluation
The patients in both the CFP and Tri-Lock stem groups showed significant improvements in the preoperative HHS and WOMAC score (P < 0.05), whereas the difference between the two groups was not significant at the first, second, or final follow-up (Table 6).
Comparison of HHS and WOMAC score in the two groups.

Data are presented as mean ± standard deviation.
HHS, Harris hip score; WOMAC, Western Ontario and McMaster University Osteoarthritis Index; CFP, collum femoris-preserving.
Discussion
Both the CFP and Tri-Lock stems are short stems. The main difference between them is that the Tri-Lock stem requires resection of the femoral neck, whereas the CFP stem does not. In this study, we retrospectively compared the clinical and radiographic results of 65 patients treated with the CFP stem versus 57 patients treated with the Tri-Lock stem to investigate the relative benefits and applicability of the CFP and Tri-Lock stems in THA. All patients were followed up for >2 years. The CFP and Tri-Lock stems significantly improved the preoperative HHS and WOMAC score; however, the difference between the two stems was not significant at various time points of follow-up. This study showed no advantage of the CFP stem over the Tri-Lock stem in improving hip function.
THA is an economical and effective surgical method. 16 In addition to alleviating pain, improving function, and improving quality of life, THA aims to restore the hip anatomy and biomechanics by reconstructing the patient’s FO and leg length with appropriate implants.17,18 Inappropriate FO may lead to worse hip function and prosthesis instability, while leg length discrepancy after THA is a common factor leading to patient dissatisfaction, claudication, and gait disturbance.13,15,19 Reconstruction of the original FO increases the abductor function and hip range of motion and reduces polyethylene insert wear. 20 In this study, the postoperative FO in both groups was significantly greater than that before surgery (mean increase of 3.63 ± 4.28 mm in the CFP stem group and 0.83 ± 5.46 mm in the Tri-Lock stem group) compared with the unaffected side. The difference between the groups was significant, and the CFP stem increased FO to a greater degree than did the Tri-Lock stem. Liu et al. 21 reported that the retention rate of the femoral neck was positively correlated with FO. This was partly explained by the unique design of the curved CFP stem. 21 Bjørdal and Bjørgul 22 compared the HHS and Hip Osteoarthritis Outcome Score between patients with a normal and increased (>5-mm) FO and found no significant difference. Although the CFP stem might increase FO to a greater degree, it has no significant effect on hip function. Additionally, femoral neck resection is known to reduce the offset and increase the force required by the abductor muscles, resulting in elevated joint loads. A mild increase in FO may be an effective means to improve the abductor function and balance control of walking after hip surgery. 23 Cassidy et al. 24 compared the WOMAC functional scores 12 months after THA among patients with a >5-mm decrease in FO compared with the contralateral side (n = 31), patients with recovery of FO (n = 163), and patients with a >5-mm increase in FO (n = 55). They reported significantly worse outcomes in the group with decreased FO. 24 In the present study, significantly fewer patients in the CFP stem group (n = 1) than Tri-Lock stem group (n = 10) had a >5-mm reduction on the unaffected side; in this regard, the CFP stem was superior to the Tri-Lock stem in reconstructing FO.
Leg length discrepancy is a well-recognized complication of THA, and excessive lengthening is the most common type of leg length discrepancy after THA. 25 Generally, a leg length discrepancy of >1.5 cm causes low back pain and gait disturbance, leading to decreased satisfaction. 26 In this study, FVO was significantly greater postoperatively than preoperatively in both groups, with a mean increase of 3.44 ± 7.24 and 3.26 ± 8.66 mm, respectively, compared with the healthy side; however, there was no significant difference between the groups. The largest proportions of patients in the 0- to 10-mm subgroup were 73.3% and 71.7%. Both the CFP stem and the Tri-Lock stem performed well in reconstructing the leg length.
With the growing number of young and active patients, the principles of tissue-sparing surgery are being increasingly appreciated. The cornerstone of tissue-sparing surgery of the hip is preservation of the femoral neck. 27 Femoral neck preservation leads to several biomechanical and biological advantages, such as better biomechanical restoration of the hip, stabilization of the triplanar stem, and maintenance of the blood supply to the neck. 28 In 2006, Pipino and Keller 29 reported the clinical and radiographic outcomes in patients treated with femoral neck-sparing arthroplasty. They conducted a retrospective study of 943 implants with 2 different neck-sparing stems (Biodynamic and CFP) and observed excellent results and best survival in 97% of patients. 29 Formica et al. 27 retrospectively reviewed 176 patients (194 hips) with CFP stems with a minimum follow-up time of 10 years and observed 6 cases of aseptic loosening, 2 cases of infection, 1 case of implant revision for recurrent dislocation, and 1 case of stem revision after periprosthetic femoral fracture; the overall survival rate was 94.8%. Many studies have shown that the CFP stem both preserves the bone mass and has a good survival rate. In the present study, one patient in each group developed hip dislocation caused by a fall in the early postoperative period, without statistical significance. No patient in either group developed a distal lateral cortical cleavage fracture of the prosthesis during surgery, and no fracture events occurred during follow-up. The usual causes of fractures include inexperience, inadequate surgical reaming, excessive force during prosthesis installation, and selection of an oversized stem. 30 Li et al. 10 noted that the periprosthetic femoral fracture rate of 10.6% with the CFP stem was significantly higher than the 1.3% rate with the ribbed stem. According to the present study, adequate templating and preoperative preparation, selection of the appropriate size, adequate reaming, and proper force application by the installation process might prevent the occurrence of fractures.
Some biases might have influenced the results of this study. We did not control for anteversion or retroversion of the stem, which might have affected the offset. This study was retrospective in nature, involving the clinical characteristics of eligible patients at risk of selection bias. Potential selection bias might have limited the generalizability of the findings to the entire patient population. Prospective randomized studies are needed to confirm the present results. Finally, the follow-up period of this study was relatively short, and the long-term observation of the service life of the prosthesis with a small increase in FO was insufficient.
Conclusions
The CFP stem reconstructed the FO better than did the Tri-Lock stem, but no significant difference was found in reconstruction of the leg length. Both stems significantly improved the preoperative HHS and WOMAC score. However, the difference between the two stems was not significant. In addition, the CFP stem preserved more bone mass and theoretically provided a good bone condition for future hip prosthesis revision. Therefore, the CFP stem is an effective method for treating joint disease in young and middle-aged patients.