
Abstract
Immune checkpoint inhibitors, such as anti-cytotoxic T-lymphocyte–associated antigen-4 and anti-programmed death-1, are a type of cancer immunotherapy approved for late-stage malignancy treatment. However, such therapies often induce immune-related adverse events. During anti-programmed death-1 blockade therapy, the most commonly reported adverse effects are skin toxicities, such as psoriasis—a chronic immune-mediated inflammatory disorder affecting the skin. We present the clinical characteristics of flared psoriasis in one patient under anti-programmed death-1 therapy who was diagnosed with T2N2M0/IIIB squamous lung carcinoma with a history of psoriasis for the past 5 years, exacerbated after the first cycle of nivolumab. After the third cycle, the extensive skin plaques necessitated treatment cessation. Following the discontinuation of anti-programmed death-1 treatment, skin lesions were treated locally. Possibly, anti-programmed death-1 immunotherapy can trigger immune-mediated diseases, such as psoriasis. Physicians should be alert to immune-related adverse events. Continuation or permanent cessation of treatment depends on the severity and reversibility of immune-related adverse events.
Introduction
Psoriasis is a common, chronic, immune-mediated, inflammatory disorder affecting the skin, nails and joints in both children and adults. The skin disorder is estimated to affect 2.0%–3.5% of the global population. 1 It affects both genders and has a bimodal peak of onset. Onset can peak at 20–30 years and 50–60 years of age. The disease is generally thought to be agenetic and triggered by environmental factors—such as trauma, infections, medicines, metabolic/hormonal factors, stress, sun exposure, alcohol use and smoking—and leads to immunological response, psoriasis vulgaris or chronic plaque psoriasis being the most common types. 2 Other types include guttatepsoriasis, erythrodermic psoriasis and pustular psoriasis. Depending on the affected body part, psoriasis is further categorized in scalp psoriasis, flexular/inverse psoriasis, nail psoriasis, palmoplantar psoriasis, psoriasis of mucus membranes/genitals and psoriatic arthritis. 2 It is also associated with a plethora of extracutaneous comorbidities such as Crohn’s disease, diabetes mellitus type II, obesity, metabolic syndrome, depression and other inflammatory manifestations of the eyes. 2 Psoriatic skin lesions are characterized by well-defined erythematousscaly plaques, and tend to have a chronic relapsing and remitting course. 1 Severity ranges from a few scattered plaques to involvement of almost the entire body surface. 1 Many severity scores have been suggested, to assess the severity of psoriasis, such as the Psoriasis Area and Severity Index (PASI), Dermatology Life Quality Index (DLQI), Body Surface Area (BSA) and Physician Global Assesment (PGA) index (Table 1). 2 Treatment of psoriasis is individualized depending on the affected body area, severity of disease and other patient specific features and may be local, systemic treatment or phototherapy. 2
Management strategies by skin toxicity grade.

BSA: body surface area.
Immunotherapy is a type of targeted therapy against cancer, 3 which boosts the body’s immune response against cancerous cells. There are several types of immunotherapy, including monoclonal antibodies (mAbs), non-specific immunotherapies, oncolytic virus therapy, T-cell therapy and cancer vaccines. 4 During the past 20 years, breakthroughs in our understanding of the regulation of T-cell immune response against pathogens or abnormal (cancerous) cells paved the way for development of mAbs that modulate T-cell activity by inhibiting “brake” receptors on the lymphocytic surface. These receptors are now designated as immune checkpoints, such as programmed death-1 (PD-1)/programmed death ligand-1 (PD-L1) and cytotoxic T-lymphocyte–associated antigen-4 (CTLA-4). 4 Checkpoint inhibitors such as nivolumab or pembrolizumab prevent the binding between T-cell inhibitory receptor PD-1 and its ligands (PD-L1, PD-L2) on the surface of tumor cells, thereby preventing T-cell anergy and unlocking the full activity of the T-cell against the tumor. It has been shown that these immune checkpoint inhibitors (ICOs) can provide durable, long-term survival benefits in patients with a variety of metastatic solid tumors with a manageable toxicity profile, distinct from that of cytotoxic chemotherapy. Generally, adverse effects (AEs) may occur early or late during therapy (within 1 week–3 months after treatment initiation), but the first onset of AEs has been reported as late as 1 year from completion of therapy. These side-effects are generally autoimmune, as a result of excessive T-cell activation and injury of normal tissues. Action should be taken to diagnose early immune-related adverse events (IrAEs), prevent further aggravation and initiate immediate steroid-based therapy. In all but the mildest cases, immunotherapy should be discontinued immediately, and immunosuppressive or immune modulating drugs initiated promptly. 5
Case presentation
A 71-year-old woman with a 40-pack-year smoking history was referred to the emergency department with fever. Her medical history included psoriasis for the past 5 years, psoriatic arthritis for the past 3 years, coronary artery disease and chronic obstructive pulmonary disease. No further symptoms were reported. The patient underwent chest X-ray which detected a mass opacity in the right lung. Further investigations with a chest computed tomography (CT) showed a subpleural mass at the peripheral part of the right middle lobe with lobular margins and irregular enhancement with a maximum diameter of 4.0 cm (Figure 1).

CT initial presentation.
No additional abnormalities were observed on subsequent detailed metastatic work-up including abdominal and brain CT. A positron emission tomography–computed tomography (PET/CT) revealed high uptake of 18F-fluoro-2-deoxy-
CT after external beam radiotherapy.

CT demonstrating disease progression after chemotherapy.
Following a brief exposure to gemcitabine/carboplatin chemotherapy for two cycles and further disease progression, immunotherapy with nivolumab i.v. 3 mg/kg was commenced. Although nivolumab therapy induced psoriatic exanthema with a 2.4 PASI score in the previously asymptomatic patient, treatment was continued for another two cycles (one cycle per 15 days). Hence, the psoriatic exanthema was exacerbated with plaques in the extremities and the trunk with a 41.6 PASI score (Figure 4).

Eruption of psoriasis-skin rashes: (a) trunk, (b) abdomen, (c) thigh, (d) legs and (e) toes.
Due to the exacerbation of psoriatic lesions which coincided with the start of nivolumab treatment, the dermatologist advised an immediate discontinuation of the anti-PD-1 treatment and the local treatment of skin lesions with moisturizing cream (eucerin), mometasone cream, acitretin and psoralen photochemotherapy (PUVA) with p.o. methoxsalen leading to visible clinical improvement of the exanthema (Figure 5) and a 2.7 PASI score.
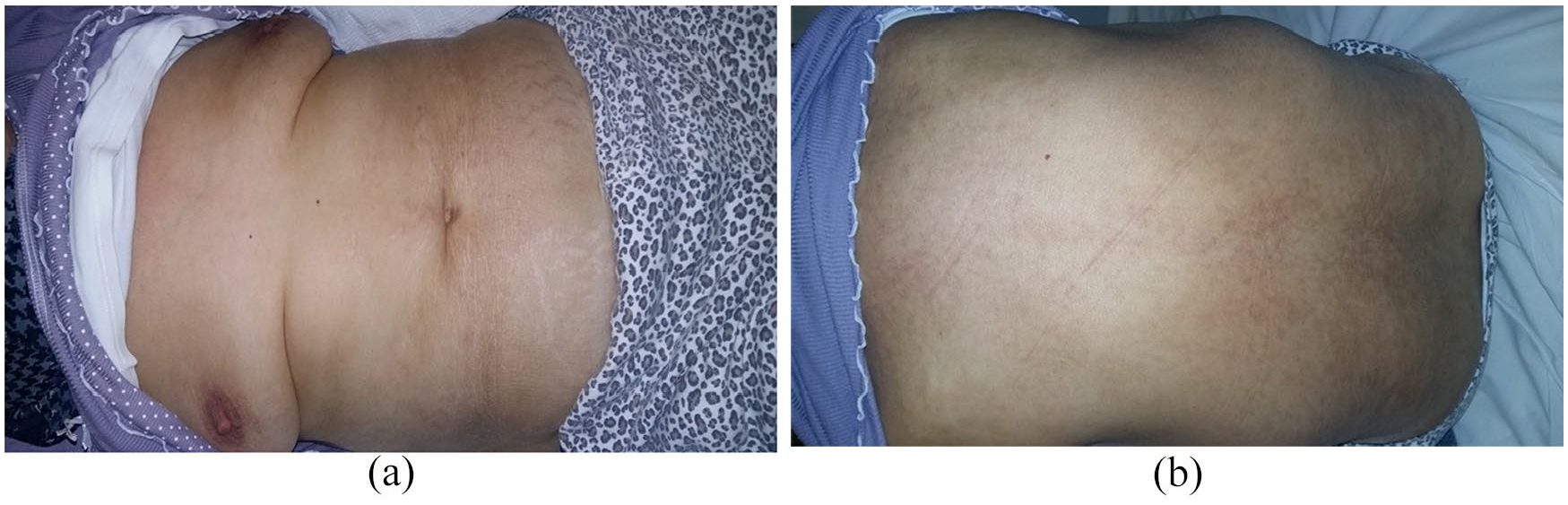
Recession of proriasis after treatment with steroids: (a) abdomen and (b) trunk.
Discussion
Immunotherapy is a new type of targeted therapy aiming at bypassing tumor-induced T-cell anergy/apoptosis, thereby restoring the activity of cytotoxic CD8 + T-lymphocytes against malignant cells that can be recognized as abnormal by the host. Over recent years, it has been licensed for patients with many malignant diseases such as lung, bladder and head and neck cancer. However, immunotherapy may induce a state of immune hyper-reactivity through the relaxation of negative control loops tightly regulating T-helper and T-cytotoxic cells, thereby causing immune-related side-effects (IrAEs), including exacerbation of pre-existing autoimmune diseases. Psoriasis, having an autoimmune aspect, can be triggered during immunotherapy, either as a new case or as worsening of an already known disease. According to the literature, nine similar cases have been reported. In those cases, patients were forced to discontinue immunotherapy because of psoriasis onset (Table 2).
Published literature on immunotherapy-induced psoriasis.
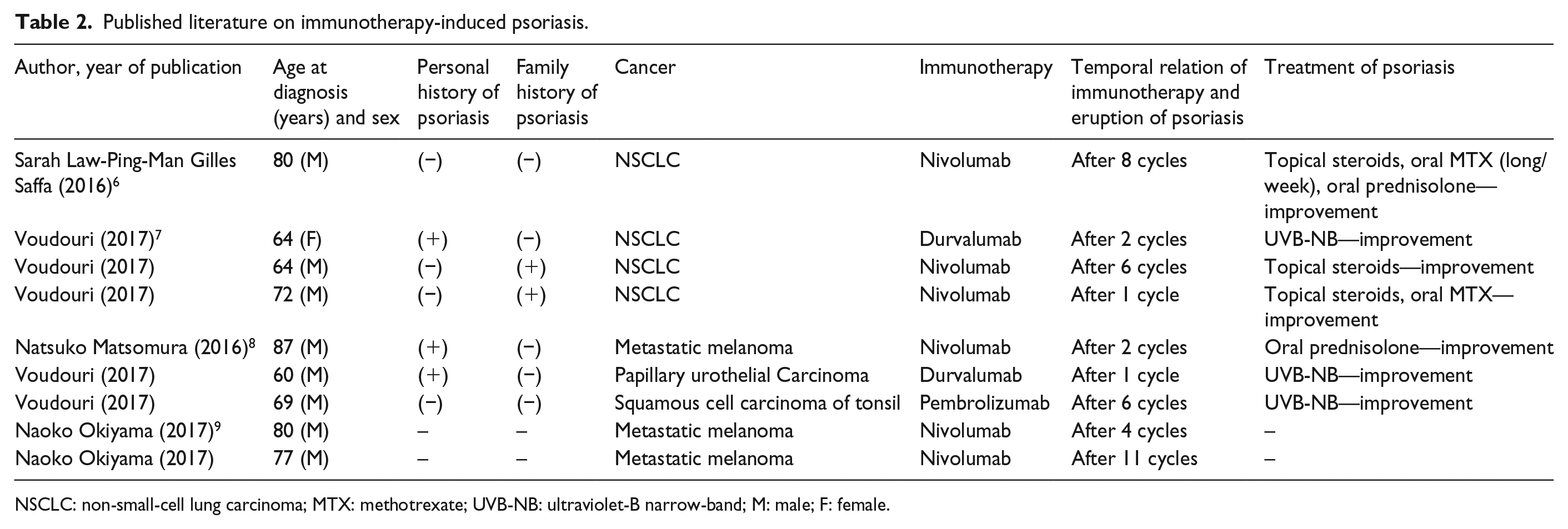
NSCLC: non-small-cell lung carcinoma; MTX: methotrexate; UVB-NB: ultraviolet-B narrow-band; M: male; F: female.
However, the possibility to re-institute immunotherapy, especially in those cases where cutaneous IrAEs are controlled using corticosteroids or immunosuppressive agents and in the presence of anti-tumor activity, should be explored with caution.
The reported skin adverse events include: (1) most common: erythema, maculopapular and pustulopapular rash; (2) rare: toxic epidermal necrolysis, Steven–Johnson syndrome and DRESS (drug rash with eosinophilia and systemic symptoms) and (3) vasculitis may also be present with purpuric rash.
Physicians who administer ICOs, especially in patients with a positive history of autoimmune disorders including psoriasis, should be aware of, and familiar with timely diagnosis and management of IrAEs. A careful pre-immunotherapy work-up on the extent and activity of psoriasis, particularly to exclude a bone involvement (psoriatic arthritis), should be sought. Moreover, it is obvious that in such cases, more guidance is needed to decide—in collaboration with the dermatologists—the most appropriate course of action on whether the anti-PD-1 treatment should be halted or not with the concurrent treatment of skin lesions, on the type of psoriasis treatment that should be commenced and so on. Depending on the reversibility of the complications, physicians could opt either to permanently discontinue immunotherapy or to reinstate it, provided control of cutaneous IrAEs is achieved and taking into consideration existing options for alternative antineoplastic therapies. 10
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient prior to publication.