
Abstract
Synovitis is a type of aseptic inflammation that occurs within joints or surrounding tendons. No previous reports have described a hypertrophic synovium eroding the tendon sheath and manifesting as synovitis within the flexor tendon. We herein report a case involving a 10-year-old girl who presented to our hospital with a 1-month history of a swollen mass and progressive inability to completely flex her left index finger. The active flexion angle of the proximal interphalangeal joint was limited to 85°. A longitudinal incision of the flexor digitorum profundus tendon was surgically performed. The synovium inside and outside the flexor digitorum profundus tendon was completely removed. After the surgical excision, normal tendon gliding returned without recurrence by the 1-year follow-up. The active flexion angle of the proximal interphalangeal joint improved to 100°. To the best of our knowledge, this is the first case of synovitis affecting the flexor tendon and leading to limited flexion of a finger. The manifestation of a double ring sign on magnetic resonance imaging is quite characteristic. Early diagnosis and monitoring of the hyperproliferation and invasiveness of the synovial tissue are required. Surgical excision can be a simple and effective tool when necessary.
Keywords
Introduction
The synovium is mainly generated around joints or surrounding tendons, not within tendons. Synovitis commonly affects finger joints and usually manifests as mild synovial effusion and/or hypertrophy. Generally, synovitis does not result in moderate to severe symptoms.1,2 According to its etiology, synovitis can be divided into degenerative or post-traumatic diseases and inflammatory rheumatic diseases. 3 Synovitis may extensively involve the peritendinous tissues, and long-term inflammation may lead to tendon damage. However, it is uncommon for synovial tissue to invade the tendon sheath and enter a tendon. We herein report a case involving a 10-year-old girl with a mass in her left index finger due to synovitis within the flexor tendon.
Case report
A 10-year-old girl presented to our hospital with a 1-month history of a progressively swelling mass and limited flexion of her left index finger. She had no apparent trauma history. A swollen and painless immovable mass was observed in the proximal interphalangeal (PIP) joint of the affected finger, without skin ulcers or redness (Figure 1). A physical examination revealed that the active flexion of the PIP joint angle had decreased to 85°, while her flexor strength was normal. The patient’s other joints and fingers were not affected. Her parents denied a history of tuberculosis, rheumatoid arthritis, or any other inflammatory diseases. Laboratory studies showed that the white blood cell count, high-sensitivity C-reactive protein level, erythrocyte sedimentation rate, and tumor marker levels were all within normal limits. The rheumatoid factor, anti-cyclic citrullinated peptide antibody, anti-streptococcal hemolysin O, and tuberculous (tuberculosis antibody and T-SPOT.TB) test results were all negative. Radiographs showed swelling of the soft tissue without bone involvement in the PIP joint (Figure 2). A chest radiograph was normal without hilar lymphadenopathy or tuberculomas. Ultrasound showed good continuity of the flexor digitorum profundus (FDP) tendon, with hyperechoic lesions both inside and outside it. The lesion moved with the tendon. Magnetic resonance imaging (MRI) demonstrated a well-defined lesion isointense to muscle on T1 sequences and hyperintense to muscle on T2 sequences, and strong homogeneous enhancement was observed after injection of contrast medium during coronal plane sequencing. The enhanced-signal lesion surrounded and partly infiltrated the FDP tendon, manifesting as a double ring sign on transverse plane sequencing (Figure 3).

Physical examination showed a swollen, painless immovable mass (arrow) in the proximal interphalangeal joint of the left index finger, without skin ulcers or redness.

Lateral radiograph of the left index finger showed soft tissue swelling on the palmar side without bone involvement.

Magnetic resonance imaging revealed a well-defined lesion in the coronal plane. It was (a) isointense to muscle on T1 sequences and (b) hyperintense to muscle on T2 sequences. The lesion surrounded and partly infiltrated the flexor digitorum profundus tendon, forming a rare double ring sign on coronal sequences. (c) The enhanced-signal lesion on axial T2 weighted sequences. (d) Strong homogeneous enhancement of the double ring after injection of contrast material.
The mass was misdiagnosed as a tenosynovial giant cell tumor (TGCT) when she initially visited a doctor at a community hospital. MRI was performed when she presented to our department, revealing a lesion within the tendon, which was an uncharacteristic finding. Conservative treatments were attempted when she first presented to the hospital, but she developed a limitation of finger flexion within a short time. Her parents consented to surgical treatment. During the operation, a volar Brunner zig-zag incision was made, and the subcutaneous lesion was exposed. The A2, A3, and A4 pulleys were all intact. During the operation, the entire A3 pulley and distal two-thirds of the A2 pulley were removed, and the proximal part of A4 was slightly cut open. The FDP tendon was found to be expanded. Hypertrophic synovium surrounded the outside of the tendon (Figure 4(a)). The synovium invaded the tendon sheath, which could not be separated. After removal of the peritendinous tissue, the flexor tendon was confirmed to be intact. It was then dissected longitudinally. A large amount of synovial-like substance was found within the tendon (Figure 4(b)). This substance was completely cleared, and the tendon was then repaired with an uninterrupted suture (Figure 4(c)). The skin wound was closed. Pathologic examination revealed synovitis with synoviocytes and inflammatory cell infiltration, without hemosiderin deposition or multinucleate giant cells (Figure 5).
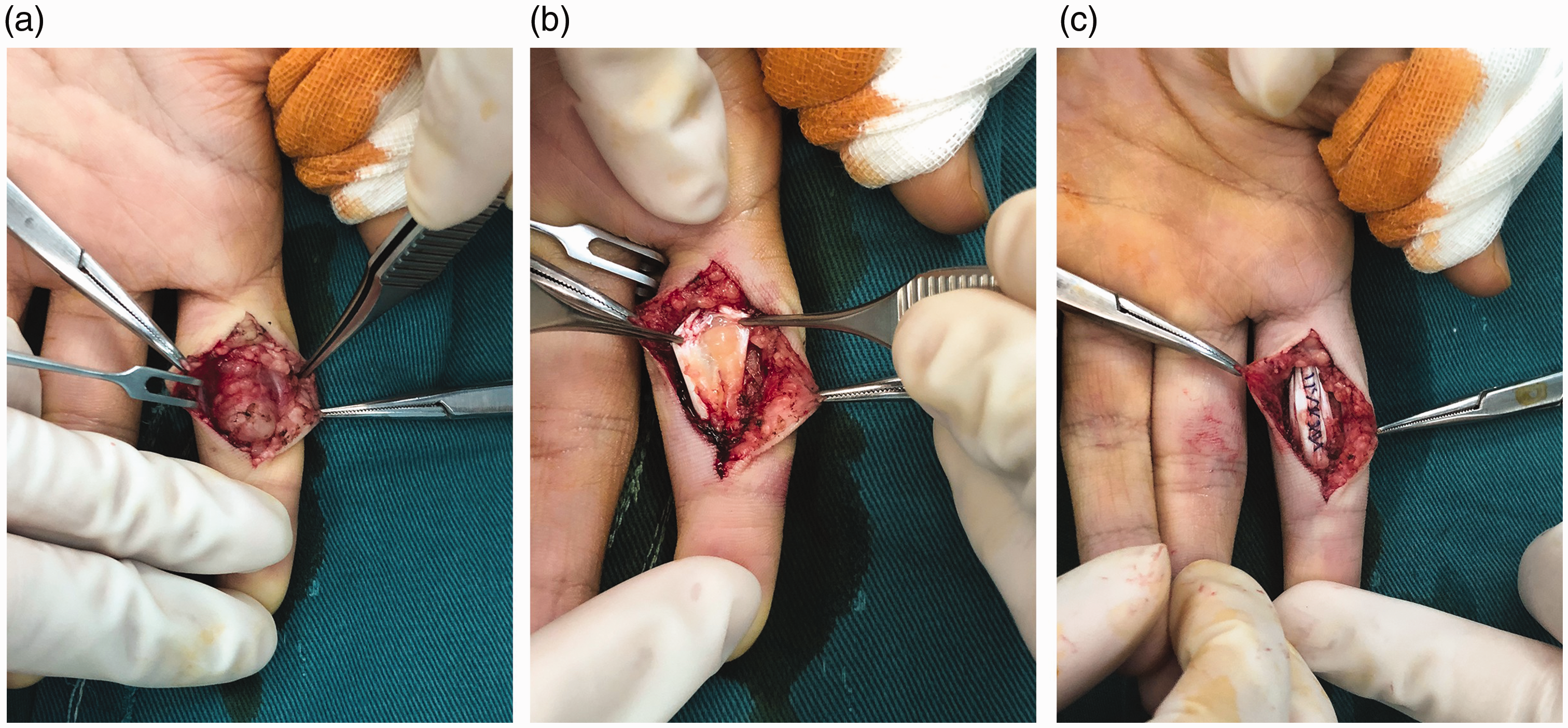
Intraoperative images. (a) The flexor digitorum profundus tendon was expanded and surrounded by proliferating synovial-like tissue and pannus formation. (b) A large amount of synovial-like substance was found within the tendon. (c) After complete removal, the broken tendon was weaved back together using an uninterrupted suture.

Pathologic examination. (a) Proliferation of synoviocytes (hematoxylin and eosin stain; magnification, ×400). (b) Lymphocyte infiltration (hematoxylin and eosin stain; magnification, ×400).
The patient received cefuroxime (Glaxo Wellcome Operations, Hertfordshire, UK) at 0.25 g twice a day for 3 days after the surgery. Active finger motion was promoted by physical therapists at the end of the first week. The sutures were removed at the end of the second week. A brace with the index finger in a functional position was used for 3 weeks. A physiotherapist supervised the patient’s rehabilitation until full active range of motion was achieved. Normal tendon gliding returned without recurrence by the 1-year follow-up. The active flexion angle of the PIP joint improved to 100°.
Discussion
The mechanism of synovial hyperplasia within the tendon in this case is still unclear. It may have been caused by minor injuries that occurred in daily life. It was not detected at the beginning of the clinical course. Synovial hyperplasia inside and outside the FDP tendon quickly appeared. The tendon increased in size, resulting in incarceration at the pulley that affected the flexor function of the PIP joint.
The patient’s mass was first misdiagnosed as TGCT, 4 the second most common soft tissue tumor of the hand. TGCTs are benign lesions that usually arise from the synovium or tendon sheaths; they are characterized by synovial proliferation and composed of multinucleated giant cells with osteoclast-like phenotypes, macrophages, histiocytes, and other inflammatory cells.5,6 Although diffuse-type TGCT may occur in the joints and extend into the tendon sheaths, it generally exhibits a lobulated or casting mold pattern with a hypointense ring on proton density-weighted imaging. 7 In patients with diffuse-type TGCT, it is uncommon to see a hypointense signal inside the tendon. Although TGCT was not definitively diagnosed and was finally excluded as a differential diagnosis, we used its treatment for reference. The differential diagnoses included tuberculous tenosynovitis and sarcoidosis, both of which develop around the flexor tendons. 8 Tuberculosis may present with tenosynovitis, arthritis, cutaneous nodules, or ulceration.9,10 However, we found no evidence of tuberculosis from the patient’s medical history, symptoms, laboratory studies, or pathological examination. Tumors such as synovial chondromatosis; arthritis including rheumatoid arthritis, 11 psoriatic arthritis, 12 and Lyme arthritis; 3 and other conditions such as gout 13 were excluded. Lesions inside tendons have not been documented in patients with any of these differential diagnoses.
Doctors should be aware of the properties of synovitis in the hand so that early diagnosis and treatment can be achieved. Surgical resection seems to be a simple and effective tool when conservative treatments fail or the patient’s subjective symptoms worsen. The pulley should be kept intact as much as possible. As mentioned above, we preserved the proximal one-third of the A2 pulley and the distal half of the A4 pulley. The FDP tendon was dissected longitudinally and then weaved back together. We believe that this helped to protect the tendon as much as possible.
The integrity of the tendon was restored in this case. A protective splint was used to help with early exercises and guard against tendon rupture, as we suggested in previous studies.14,15 MRI can be used to monitor the healing quality of tendons and recurrence of synovitis during the follow-up period as necessary. 16 We intend to monitor the long-term postoperative results of the patient discussed in this case.
In conclusion, this is the first reported case of nontraumatic synovitis within the flexor tendon leading to flexor dysfunction of the finger. The manifestation of a double-ring sign on MRI is quite characteristic. Early diagnosis and monitoring of the hyperproliferation and invasiveness of the synovial tissue are required. Surgical excision can be a simple and effective tool if required.
Footnotes
Acknowledgements
I (QJ, first author) would like to express my sincere gratitude to my colleague, Dr. Hui Lu, who provided support in every step of this study. Additionally, I thank the funding program for sponsoring our research. Finally, I would like to thank my fiancé, lawyer Hui Cai, for assisting with the figures and ethical principles of this study.
Authors’ contributions
QJ and HZ conceived of the study. HL and HZ participated in the design of the study. QJ drafted the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics
This study protocol was approved by the Medical Ethics Committee of the First Affiliated Hospital, College of Medicine, Zhejiang University. Written informed consent for publication of the girl’s clinical details and clinical images was obtained from her parents. Upon request, a copy of the consent form is available for review by the Editor of this journal.
Funding
The data collection and analysis in this study were supported by the National Natural Science Foundation of China (grant number 81702135).