
Abstract
Posterior fossa dermoid cysts are uncommon benign congenital abnormalities. Meningitis is seen as a primary symptom in these situations, more rarely we can find cerebral abscesses. In this case, we describe a 4-year-old Syrian boy who presented with headaches and frequent vomiting as his major complaints. No indication of cerebellar injury was present. He had signs of hydrocephalus like grade III bilateral papilledema but did not develop meningitis. The patient was diagnosed with a complete dermal sinus of the posterior cranial fossa in combination with an infected intradural dermoid cyst and a secondary abscess formation. In Conclusion, the preoperative diagnosis of infected dermoid cysts and dermal sinus tracts lacking signs of infection or meningitis poses challenges, particularly when accompanied by hydrocephalus that can resemble cerebellar tumors. Thorough preoperative assessment is vital for these complex cases.
Introduction
Dermoid cysts in the posterior fossa are uncommon, benign, congenital lesions. They originate from defects in the separation of the ectoderm and neuroectoderm during the 3rd to 5th weeks of gestation.1,2 Clinically, these cysts primarily manifest as intracranial hypertension. Additionally, they can lead to meningitis, which may result from a bacterial infection that could also cause abscesses within the dermoid cyst itself. 3 The preoperative diagnosis of an infected dermoid cyst and a complete dermal sinus tract, especially in the absence of infection or meningitis symptoms, can pose a significant challenge. This challenge is further compounded when the cyst is accompanied by hydrocephalus, which can mimic a cerebellar tumor. In this paper, we present a case of an infected intradural dermoid cyst with a dermal sinus tract.
Presentation
A 4-year-old Syrian male was admitted to the hospital with a 3-week history of severe frontal headaches and frequent vomiting, occurring 6–7 times daily. The headaches, which often awakened him from sleep, were partially relieved by analgesics.
Upon admission, he was alert and cooperative, with average or low vital signs. Despite being underweight, pale, and lethargic, he showed no signs of fever or mental confusion. He exhibited no signs of cerebellar injury (no ataxia, seizures, or nystagmus). However, he did exhibit grade III bilateral papilledema and indicating hydrocephalus. Neurologic examination revealed normal sensory and motor function, with normal psychomotor development.
The patient’s tests are presented in Table 1.
Laboratory values results for patient tests.
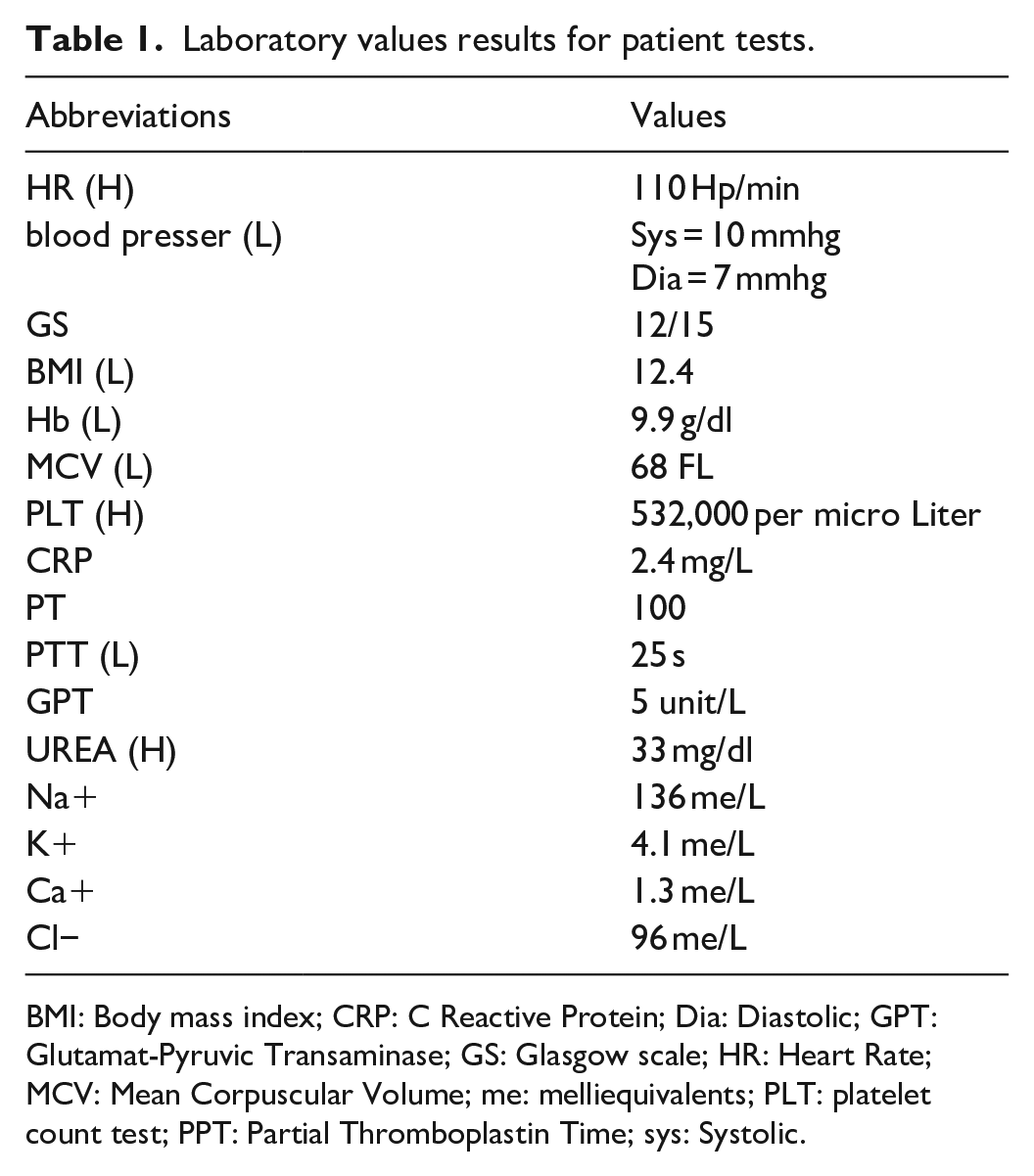
BMI: Body mass index; CRP: C Reactive Protein; Dia: Diastolic; GPT: Glutamat-Pyruvic Transaminase; GS: Glasgow scale; HR: Heart Rate; MCV: Mean Corpuscular Volume; me: melliequivalents; PLT: platelet count test; PPT: Partial Thromboplastin Time; sys: Systolic.
Several days before admission, the patient underwent computed tomography (CT) scan at another facility where an MRI was not available. The CT scan revealed a well-defined, rounded, cranial hypodense lesion on the midline of the posterior fossa (Figure 1).

Preoperative computed tomography image shows a round, cranial hypodense dermoid cyst on the midline of the posterior fossa.
Besides, according to the parents, the patient was given antibiotics medications for probable meningitis, which we believe had been taken into consideration after a cerebrospinal fluid (CSF) test, However, no available documents for either a CSF test or the antibiotics the patient have taken.
Upon admission to our hospital, an MRI was performed, which revealed a median, rounded, cystic, subtentorial mass in the posterior fossa with ring enhancement of the cystic walls and a linear dermal sinus connecting with the dura (Figure 2).

(a) and (b) Sagittal and axial cranial magnetic resonance imaging shows a median, rounded, cystic, subtentorial mass in the posterior fossa with ring enhancement of the cystic walls AND a linear dermal sinus connecting with the dura.
The radiological study revealed cerebellar lesions along the midline and left side, suggestive of abscesses. These lesions resulted in cerebellar tonsillar herniation and severe obstructive hydrocephalus. Differential diagnosis considered posterior cranial fossa tumors such as astrocytoma, in addition to dermoid cysts and dermal sinuses.
Considering the possibility of dermoid cysts, a more thorough clinical examination was performed. After shaving the occipital region of the scalp, a small dimple covered by hair was discovered. Further investigation revealed intermittent drainage of creamy purulent fluid from this site, which had closed spontaneously and was overlooked until admission.
These clinical findings, correlated with the prior MRI results (Figure 2), which demonstrated a cyst communicating from the meninges to the skin surface, led to the suspicion of an infection in the cyst. An investigative biopsy was performed through a burr hole in the occipital bone, using the dimple as a leading point.
Culture results confirmed a Staphylococcus epidermidis infection.
Although there is some debate about performing surgery during an active infection.
Besides knowing that the patient’s condition is stable, MRI images did not reveal any radial signs of meningitis, and the infection is limited by the content of the cyst in the posterior fossa, it is generally considered prudent to delay the surgery until the infection is controlled. Therefore, intravenous antibiotic therapy (metronidazole, vancomycin, and cefotaxime) was initiated and continued for 1 week.
Subsequently, the patient underwent a sub-occipital craniotomy, during which a midline dermal cyst connected to a complete cerebellar fistula was identified and completely resected (Figure 3). The meninges were closed with a patch.
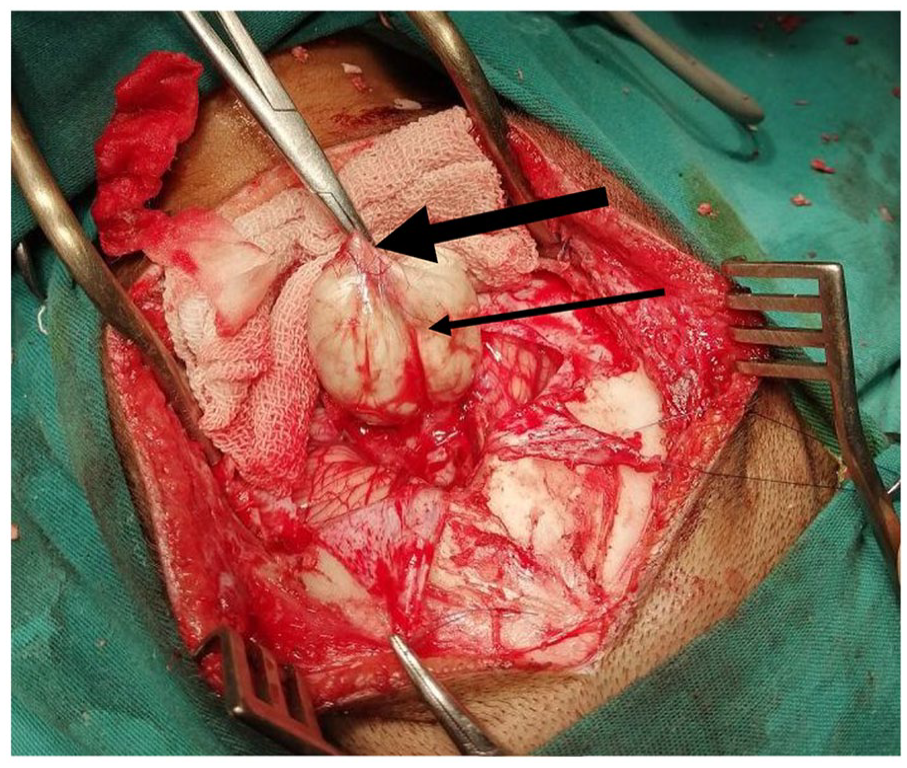
Intraoperative photograph indicates, the sinus tract (thick arrow), and the dermoid cyst (thin arrow).
Pathologic examination revealed an open cystic mass measuring 4 × 3 × 2 cm. The cyst wall was thin and lined by stratified squamous epithelium. Contents included keratin, dermal appendages such as hair, pasty material, and purulent fluid with macrophages and giant cells. These findings were consistent with an infected intradural dermoid cyst associated with a complete dermal sinus tract.
Postoperatively, the patient recovered well on antibiotic therapy containing vancomycin 40 ml/kg and metronidazole 15 ml/kg for 1 week, with nutrition, analgesia, and close monitoring. He was discharged after 10 days with normal neurologic and sepsis examination findings according to the doctors treating him. However, clinical and radiological follow-up was not documented.
Discussion
Given the rarity of this condition, the objective of this paper is to present our unique case while also conducting a comprehensive literature review. This review aims to provide insights into the characteristics, Complications, treatment approaches, and Diagnoses of patients with infected dermoid cysts with associated dermal sinus. To achieve this, a systematic search was conducted in the PubMed database spanning from the year 1987 to April 2023. This search was specifically limited to English-language publications using keywords. It’s important to note that this review exclusively includes cases of infected dermoid cysts with associated dermal sinus, excluding cases reported by (HAYER et al., 4 and Groen et al. 5 ) (Table 2).
Review of the literature regarding the previously published cases of infected dermoid cyst with associated dermal sinus.

CT: computed tomography; EAD: external abscess drainage; EVD: external ventricular drainage; MR: magnetic resonance; RICP: raised intracranial pressure.
Classification
Intracranial dermoid cysts, which are rare and benign, originate congenitally. They gradually enlarge due to progressive epithelial desquamation and glandular secretion within the cyst. These lesions represent only 0.1%–0.7% of intracranial tumors.3,20,21
In a similar vein, dermal sinus tracts, first described by Ogle in 1865, 22 are a rare form of craniospinal dysraphism. They are characterized by a cutaneous depression or tract that communicates between the skin surface and deeper structures. 23 Dermal sinus tracts can occur anywhere along the craniospinal axis. They are most commonly found in the lumbar (41%) or lumbosacral (35%) regions, followed by the occipital, thoracic (10%), and cervical (1%) areas.23,24
Logue and Till have classified posterior fossa dermoid cysts into four groups. This classification is based on location (extradural vs. intradural) and the degree of dermal sinus tract development 25 :
Extradural cyst with a complete sinus.
Extradural cyst without a sinus.
Intradural cyst with an incomplete sinus.
Intradural cyst with a complete sinus.
Our case falls into the fourth category.
Clinical presentation
Intracranial dermoid cysts generally present with meningitis as the most prevalent manifestation. However, they can occasionally lead to increased intracranial pressure due to the mass effect that dermoids can mimic. This can result in a range of symptoms of varying severity, such as headaches, seizures, and vomiting. Late diagnosis can lead to the rupture of dermoid cysts, which may indicate the presence of chemical meningitis. Additionally, if the cyst is large and interrupts the ventricular system, hydrocephalus is a possibility. Such cases are most commonly seen when the dermoid cyst is located in the posterior fossa or fourth ventricle. The presence of fever is a unique feature of infectious mass lesions in this area.14,26,27
In our literature review of cases of infected dermoid cysts with dermal sinuses in the posterior cranial fossa, three patients presented with symptoms of meningitis (referenced as 7, 9 in the literature file). All patients had increased intracranial pressure due to the mass effect of the lesion, and six patients presented with symptoms of infection.9–13,19
Radiological imaging can provide strong evidence for diagnosis by showing a well-defined, midline, unilocular cystic mass that contains actual fat or if a fat-fluid level is observed. Despite the slow growth of dermoid cysts, they can compress nearby structures. 26 This was observed in the imaging findings for all patients included in our review.
Dermoid cysts diagnosis
The patient’s clinical condition plays a central role in selecting the type of radiological imaging, which aids in the accurate diagnosis and management of the situation. Symptoms such as hydrocephalic hypertension, seizures, and vomiting may suggest the presence of intracranial tumors. These tumors create a mass effect, which is evident in the clinical presentation of the case, making a CT scan the first-line diagnostic tool. This tool is specifically used for obtaining accurate details about the size and precise location of the cyst, detecting any contraction or discontinuity in the skull’s bony borders, and determining any chronic calcification.
Typically, dermoid cysts appear on CT as well-defined hypodense or slightly isodense lesions on the midline. 7 This can be clarified if the cyst is not infected; otherwise, the CT scan may show peripheral enhancement instead. 3 This was exactly what was found in all cases in our literature review, except for the last one. 18
In our case, the preoperative CT showed a posterior fossa hypodense lesion at the midline, with a mass effect on the brainstem and cerebellar hemispheres, resulting in fourth ventricle compression and active obstructive hydrocephalus (Figure 1).
Consequently, when a professional, clinically based diagnosis is required, doctors can rely on the CT scan as a comprehensive technique. 3
On the other hand, if the previously mentioned symptoms are associated with any skin openings or dimples on the midline of the posterior scalp, suggesting intracranial dermoid cysts, then MRI imaging would be the modality of choice. We can find a hyperintense appearance on T1WI in typical cases, while T2WI shows varying degrees of hypo- to hyperintensity, providing nonhomogeneous lesions. For diffusion-weighted images (DWIs), they tend to show average restriction.3,14 This was clearly what was found in MRI images in all cases in Table 2, as we considered only infected dermoid cyst cases in our review.
In this case, the MRI revealed a sub-tentorial cystic mass with ring enhancement of the cyst walls, and a linear dermal sinus tract connecting to the intracranial lesion (Figure 2).
However, in cases of ruptured dermoid cysts or formation of cranial abscesses, we can notice the hypointensity on T1WI images and marked restriction on DWI images. 12 Also, the local bony defect that connects the dermal sinus with intracranial lesions can be clearly exposed on sagittal MRI.3,14
Additionally, the presence of meningitis symptoms, including persistent fever, neck stiffness, and photophobia, strongly suggests an intracranial infection, whether it is an infected lesion or brain abscesses. With guiding radiologic images that reveal an intracranial lesion, this situation is mostly described in dermoid cyst cases due to the possible connection between the internal lesion and the skin surface.
In our case, despite the cyst infection, our patient exhibited no signs of meningitis. The isolated organism was Staphylococcus epidermidis. According to Kara et al., 23 Staphylococcus aureus is the predominant organism in infected dermal sinus tracts.
It is clear in our literature review that only three cases were diagnosed with Staphylococcus epidermidis in the past 36 years.11,15,19
The history of vomiting and frontal headache that our patient presented with, along with MRI findings, was more indicative of obstructive hydrocephalus than a dermoid cyst, initially suggesting posterior cranial fossa tumors as the probable diagnosis.
Complications
Due to their slow growth, insidious symptoms, and a lack of healthcare and awareness from birth, lesions such as intracranial dermoid cysts often remain undiagnosed for extended periods.
As a result, many severe neurological complications can arise. Dermoid cysts could rupture, and their content could disseminate through the CSF, causing recurrent meningitis, known as aseptic meningitis. The formation of infections and abscesses is also cited. However, in the absence of any cause or sign of infection, we can observe the mass effect through manifestations such as hydrocephalus, stroke, or secondary epilepsy. 28
Treatment
The treatment of posterior fossa dermoids and sinus tracts is primarily surgical. During surgery, great care must be taken as the sinus tract typically courses near the torcula. The goal is the total excision of the dermoid cyst and tract, after which recurrence is unknown.5,25
The timing of surgery during an active infection remains a topic of debate. A comprehensive literature review by Vinchon et al. 29 concluded that surgery should be performed as soon as possible when a cyst infection is present. However, another report suggested that it might be wise to delay the surgery for weeks until the infection is controlled. 30
In this case, after 1 week of intravenous antibiotics, surgical excision was performed, followed by a 10-day course of systemic antibiotic therapy. The patient was discharged without complications following the complete removal of the lesion. However, the post-treatment clinical and radiological follow-up was undocumented, which we consider a limitation in our case.
Conclusion
The preoperative diagnosis of an infected dermoid cyst and a complete dermal sinus tract without any clinical evidence of infection or meningitis can be extremely difficult, especially in the presence of hydrocephalus that may mimic a cerebellar tumor. Careful evaluation of such cases is critical.
Footnotes
Acknowledgements
We wish to show our appreciation to Stemosis for Scientific Research, an official Syrian Scientific Research entity managed by Nafiza Martini for the scientific environment they provide and their considerable contribution in publishing this paper. The authors wish to express gratitude to Majd Hanna for her assistance with bibliography and reviewing the paper.
Author contributions
E.M. contributed to drafting, reviewing, editing, and approving the final manuscript. H.A. is a co-first author equally with E.M., contributing to drafting, reviewing, editing, and approving the final manuscript. N.M. contributed to conceptualization, supervising, drafting, reviewing, corresponding, editing, and approving the final manuscript. R.A. contributed to reviewing, supervising, and approving the final manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient’s parents for the anonymized information to be published in this article.
Provenance and peer review
Not commissioned, externally peer-reviewed.