
Abstract
Very few cases of bilateral and recurrent teratomas have been reported. We present the case of a 21-year-old nulliparous female who presented to an outside facility complaining of left flank pain and was found to have bilateral ovarian teratomas. The physician proceeded with a laparotomy. Five years later, the patient presented to our facility complaining of abdominal pain. Imaging revealed a second incidence of bilateral dermoid cysts for which she underwent a bilateral laparoscopic cystectomy. The patient retained her fertility and was able to deliver a newborn 2 years later. At the age of 31, and during a regular check-up, the patient was found again to have a third incidence of bilateral dermoid cysts for which she underwent bilateral laparoscopic cystectomy with preservation of her ovaries. In conclusion, laparoscopic removal of dermoid cysts is of utmost importance to retain the fertility of young patients. Regular check-up by ultrasound post-operatively is necessary to screen for recurrences and prevent painful presentations.
Introduction
Mature cystic teratomas are benign well-differentiated germ cell tumors. 1 They usually involve all three embryologic germ layers: endoderm, ectoderm, and mesoderm. 1 These tumors may undergo malignant transformation in around 0.1%–0.2% of cases. 2 Around 90% of mature cystic teratomas are unilateral. 1 In addition, these tumors tend to recur in around 4% of cases. 3 In this case report, we describe a rare case of bilateral mature cystic teratomas that recurred bilaterally three times within a 10-year period. Laparoscopic cystectomies allowed the patient to conceive and deliver within this period. We emphasize the need of regular follow-up of both ovaries after the first diagnosis irrespective of the clinical status of the patient.
Case description
A 21-year-old nulliparous female presented to an outside facility with what would turn out to be her first incidence of bilateral ovarian teratomas. Our patient presented complaining of pain in the left flank and hip of 1-day duration. A subsequent pelvic ultrasound showed a left ovarian torsion with a cyst measuring 11 cm. As such, the physician proceeded with a mini laparotomy at the outside facility. During surgery, three dermoid cysts, 4 cm, 2.5 cm, and 1 cm in size, were found in the left ovary in the setting of an ovarian torsion without ovarian necrosis. Due to the high incidence of bilateralism, the surgeon decided to inspect the right ovary for any suspicious lesions. The right ovary was also found to have five dermoid cysts, the biggest of which measured 3 cm. Left ovarian untwisting with bilateral ovarian cystectomies were performed. The patient was discharged on her second post-operative day. Histopathological findings confirmed the presence of mature teratomas bilaterally with no signs of malignancy and immature elements. The benign tumors consisted of a center of pilosebaceous material with calcified fat areas surrounded by cystic and gelatinous components.
After 5 years, the patient, still nulliparous and not seeking conception, presented to our out-patient department with increased bloating and intermittent abdominal pain. The pain was localized to the lower quadrant bilaterally, described as severe discomfort of 1-month duration. The patient denied any history of dysmenorrhea, menorrhagia, or fever. Contrast-enhanced computed tomography (CT) scan done revealed bilateral ovarian teratomas (Figure 1). A transvaginal sonography (TVS) was done as well. There was a complex right ovary measuring 72 × 40 mm. The normal ovarian tissue measured approximately 3 cm. Two dermoid cysts were noted, one of which was hemorrhagic. One of the dermoid was homogeneously hyperechoic and measures 3.3 × 2.5 cm. The other dermoid contained hyperechoic tissues and cystic spaces. It measured 4.0 × 2.9 cm. The left ovary was obscured by bowels and was not identified. No free fluid or collection was seen (Figure 2). The uterus was normal measuring 85 mm showing no lesions with an endometrial thickness of 10 mm. She underwent laparoscopic bilateral ovarian cystectomy in our hospital, and the pathological report revealed bilateral ovarian teratomas with an absence of malignancy.

Enhanced CT scan of the abdomen and pelvis showing a hypodense, non-enhancing right ovarian mass, measuring 3.3 × 3 × 3 cm (anteroposterior, transverse, and craniocaudal dimensions), mostly composed of macroscopic fat and containing internal calcification (red arrow). There is another hypodense, non-enhancing mass at the left ovary measuring 2.8 × 2.5 × 2.7 cm (anteroposterior, transverse, and craniocaudal dimensions) also composed of fat (yellow arrow). Findings are consistent with bilateral ovarian teratomas.
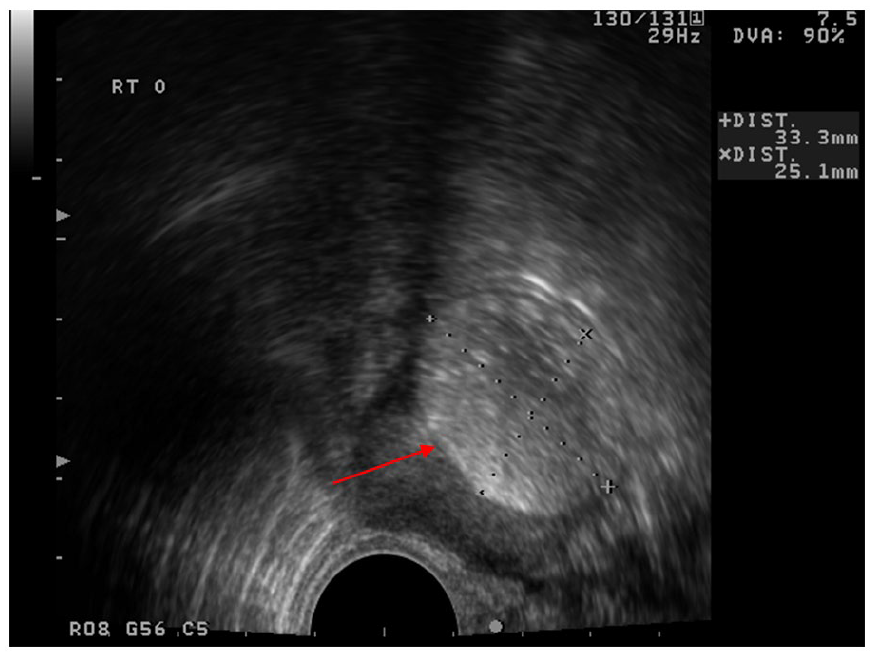
Transvaginal ultrasound (TVUS) showing a 33 × 25 mm homogeneous hyperechoic dermoid cyst in the right ovary.
Two years later, patient became pregnant spontaneously. She was closely followed up with first trimester screening showing an active fetus with normal fetal heart rate. Nuchal translucency was normal for gestational age, and low risk of neural tube defects, Patau’s, Down’s, and Edward’s syndrome. The patient was closely followed up during the rest of the pregnancy. Her second trimester was uneventful and her pelvic ultrasounds and appropriate screens including gestational diabetes were all within normal limits. At 34 weeks, she got an obstetrical growth scan ultrasound that showed a normal 2.885 g fetus in cephalic presentation and with normal cardiac activity. The placenta was anterior and with no evidence of previa, the cervix was closed, and the amniotic fluid was adequate. She presented to the hospital at 39 weeks + 5 days for induction of labor for decreased fetal movements and pelvic ultrasound showed an AFI (amniotic fluid index) of 8 cm. Normal fetal heart rates were noted on Doppler ultrasound. Pitocin augmentation was started since cervix was favorable and under epidural anesthesia she delivered by spontaneous vaginal delivery a live baby boy, Apgar score of 9 and 10 at 1 and 5 min respectively. Complete placenta and membranes were delivered without complications, and she had a good uterine tone post-delivery with minimal blood loss. She was discharged and received regular follow-up care in 6 weeks for postpartum check and then yearly exams as usual. She had been well for the next 4 years. At the age of 31, during a routine yearly visit, patient was found to have pelvic fullness on exam, pelvic ultrasound was performed and bilateral dermoid cysts were noted. The patient was completely asymptomatic prior to the exam. For the third time, the patient underwent a bilateral laparoscopic ovarian cystectomy. Pathology results again this time revealed findings suggestive of benign mature cystic teratomas (Figure 3). Histopathological findings confirmed teratomas, composed of sebaceous and keratinous materials as well as hair shaft components. No evidence of malignancy was found. Her carbohydrate antigen (CA) 19-9 level was elevated, 92.27 U/mL.

Right ovarian cyst (2018): Benign mature cystic teratoma. Hematoxylin & eosin staining features. Section showing tissue elements from different germ cell layers featuring skin (right), thyroid surrounded by adipose (middle), and cartilaginous (left) tissues. Magnification: x40.
After discharge, the patient underwent follow-up at 1, 3, and 9 months. She did not report abdominal pain or menstrual abnormalities, and a pelvic sonography did not demonstrate any signs of recurrence or residual tumor.
Discussion
Benign teratomas are the most common ovarian neoplasms, constituting around 25% of all ovarian neoplasms and up to 90% of ovarian germ cell tumors.2,4 The word teratoma could be literally translated to monstrous growth. They are, by definition, cystic structures containing elements of the three germ layers. The tissue may include skin, bone, or teeth. 4 Teratomas tend to be bilateral in 10%–15 % of the cases. Almost all teratomas are 46 XX, as it is postulated that a teratoma rises from a single oocyte that underwent an arrest of development after meiosis I. 4 While one hypothesis postulates that a teratoma arises by parthenogenesis from a single oocyte, another one states that a teratoma is the product of fusion of the second polar body with an oocyte. What is certain, however, is that a teratoma is not a product of neither a somatic cell nor a single oogonium, and it usually begins after the 13th week, the time at which the first meiotic division takes place. 4
Ovarian teratomas are most commonly detected as incidental findings upon abdominal imaging. 4 Other presenting symptoms include pain, abdominal or pelvic pressure, or any other signs related to one of its complications, including hemorrhage, infection, torsion, or rupture. Unusual presentations include autoimmune hemolytic anemia, thyrotoxicosis, and carcinoid syndrome. 4 Our patient had three different presentations successfully. Her first presenting sign was left flank pain radiating to the iliac fossa, and she was found to have a left ovarian torsion with bilateral ovarian teratomas. On her second admission, the patient was complaining of abdominal pain, bloating, and fullness, but no torsion was detected at that time. In contrast, the bilateral teratomas on her third admission were incidental findings on regular yearly pelvic exam that prompted an ultrasound, as the patient was asymptomatic.
Ultrasound is most commonly used to diagnose mature teratoma. Most teratomas show nonspecific findings on imaging.5,6 It may, however, present as an echogenic mass with areas of attenuation attributed to the sebaceous component. Another imaging finding includes the presence of echogenic streaks related to the hair component of the teratoma.5,7 A teratoma may also present on ultrasound as cystic lesion with an echogenic tubercle projecting in the lumen. 5
Taking into consideration the low specificity of the ultrasonographic findings and the wide differential diagnosis, serum markers are used to support the diagnosis of teratomas. CA 19-9 appears to have an important clinical significance. In a retrospective study done at the Department of Obstetrics & Gynecology at the Third Affiliated Hospital of Suzhou University, Changzhou (China), five serum biomarkers (CA 19-9, cancer antigen (CA) 125, alpha fetoprotein (AFP), carcinoembryonic antigen (CEA), and CA 153) were analyzed in 312 patients who were diagnosed with ovarian teratomas. 8 It was found that CA 19-9 was elevated in 45.83% of the cases, compared to 6.09% for CA 125. 8 It was also found that bilateral torsion–associated or multilocular teratomas have higher levels of CA 19-9. This highlights CA19-9 as an important marker in guiding the need for surgery, of close examination of the lesion, or even an examination of the other ovary. Last, it was also shown that CA 19-9 may be used as a marker of recurrence. 8 Other studies suggest that an elevated level of CA 19-9, associated with a low CA 125, is a useful marker in differentiating between ovarian teratoma and carcinoma.9,10 Our patient did not have any markers assessed in her first or second admission but had elevated CA 19-9 levels (92.27 U/mL) in her third admission. 8 Unfortunately, CA 125 levels were not assessed.
Laparoscopic surgery is the gold standard approach for the removal of mature cystic teratomas. It is associated with less bleeding, reduced post-operative pain, fewer adhesions, better cosmetic results, and a shorter hospital stay. 11 In addition, laparoscopic surgery is more cost-effective as it is associated with earlier hospital discharge. 12 Laparotomy may be considered in the presence of a large mass (usually >10 cm) with solid components. 11 It is important to note that the decision to go for laparoscopy and laparotomy should, in most instances, take several factors into consideration, including the patient’s age and wishes, the available equipment, and the surgeon’s skills, in addition to the lesion’s characteristics, including its size, probable nature, and complexity. Ovarian cystectomy is usually the technique of choice in young woman. 11 Oophorectomy is usually performed if the patient is postmenopausal, perimenopausal with multiple large cysts, or wishes to remove her ovaries. In addition, surgeons may go for oophorectomy if the mass is large enough so that no ovarian tissue is conserved. 11 Although content spillage is higher using the laparoscopic technique, the risk of chemical peritonitis or chronic pelvic pain is minimal when a tissue retrieval bag is used and adequate peritoneal lavage is performed at the end of the procedure.11,13 Expectant management may be adequate if the mass is small; size limits are still controversial, but usually <5–6 cm is acceptable.11,14 If the patient is not a surgical candidate and there are no imaging features suggestive of malignancy, then expectant management is highly advised. The length and frequency of follow-up by TVS are still controversial. 11 Finally, in the case of an ovarian torsion, untwisting is considered if the patient is young, is willing to conceive, and ovarian tissue is conserved.
In a retrospective study involving 382 patients at the Department of Obstetrics and Gynecology, Faculty of Medicine, University of Tokyo, Tokyo, Japan, three main predictive factors for ovarian teratoma recurrence after surgical excision were determined. 3 These included: bilateralism, young age (<30 years), and size >8 cm. 3 Particularly, laparoscopy, unlike previous beliefs, was not associated with an increased risk of recurrence compared to laparotomy. Any combination of the previously mentioned predictive factors further increased the recurrence risk. 3 In our case discussed above, two out of three mentioned factors were present: the patient was younger than 30 years old at her first and second presentation, and she had bilateral ovarian teratomas in all her presentations as well.
Conclusion
In conclusion, this is a case of a bilateral teratoma recurring twice with preserved fertility before the third incidence. We would like to reiterate previous recommendations concerning frequent post-operative follow-up with sonographic examinations. Routine inspection of the contralateral side is necessary during preoperative and intraoperative examination to minimize surgical re-interventions. In addition, conservative management to preserve fertility and rule out malignancy is recommended.
Footnotes
Data availability
All data are obtained from the patient’s medical charts at the Obstetrics and Gynecology Clinics at St. Georges Hospital University Medical Center. Data cannot be shared without the patient’s consent.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This case report was written in accordance with the ethical principles agreed upon in the Declaration of Helsinki. A written informed consent was provided by the patient.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.