
Abstract
Pelvic masses frequently originate from the pelvic cavity and are often associated with uterine, ovarian, or intestinal disorders. This report describes the case of a patient with a pelvic mass diagnosed as a retroperitoneal dermoid cyst at our hospital. We analyzed this case and conducted a literature review, to mitigate the risk of misdiagnosis and enhance the treatment of retroperitoneal masses.
Keywords
Introduction
Pelvic masses represent a common and challenging clinical issue in gynecological practice, with diverse origins, involving both gynecological and non-gynecological diseases. These masses can be benign or malignant, with significant variations in symptoms and management approaches. The diagnostic process can be particularly complex and challenging when the masses are located in atypical areas, such as the retroperitoneum. We report the case of a 40- to 45-year-old female patient initially diagnosed with a pelvic mass, in whom further diagnostic assessments revealed that the mass was actually a dermoid cyst located in the retroperitoneum. This case emphasizes the importance of comprehensive diagnostic evaluations and explores the role of targeted surgical interventions in managing complex pelvic masses, highlighting the critical nature of an accurate diagnosis for implementing effective treatment strategies. Through this case, we aim to enhance the diagnostic awareness and management capabilities of clinicians regarding pelvic masses and their surrounding regions.
Case report
A female patient, aged 40 to 45 years, presented with a 5-day history of a pelvic mass and irregular menstruation over the last 6 months. An ultrasound examination revealed adenomyosis of the uterus and a heterogeneous mass measuring 87 × 64 mm in the left adnexal region. The patient had no significant history of infectious diseases or chronic conditions and no prior abdominal surgeries. A preoperative magnetic resonance imaging (MRI) examination was conducted (Figure 1). The CA125 tumor marker level was 67.29 U/mL, and CA19-9, alfa-fetoprotein, carcinoembryonic antigen, and HE4 were within normal ranges. The results of other blood tests, including liver and kidney functions and coagulation profiles, were unremarkable, except for a white blood cell count of 2.89 × 109/L. Upon admission, the provisional diagnosis was “pelvic mass, uterine adenomyoma”. The possibility of a retroperitoneal origin was not ruled out because of the low location of the pelvic mass. Granulocyte colony-stimulating factor (G-CSF) was administered to normalize the white blood cell count, after excluding surgical contraindications.
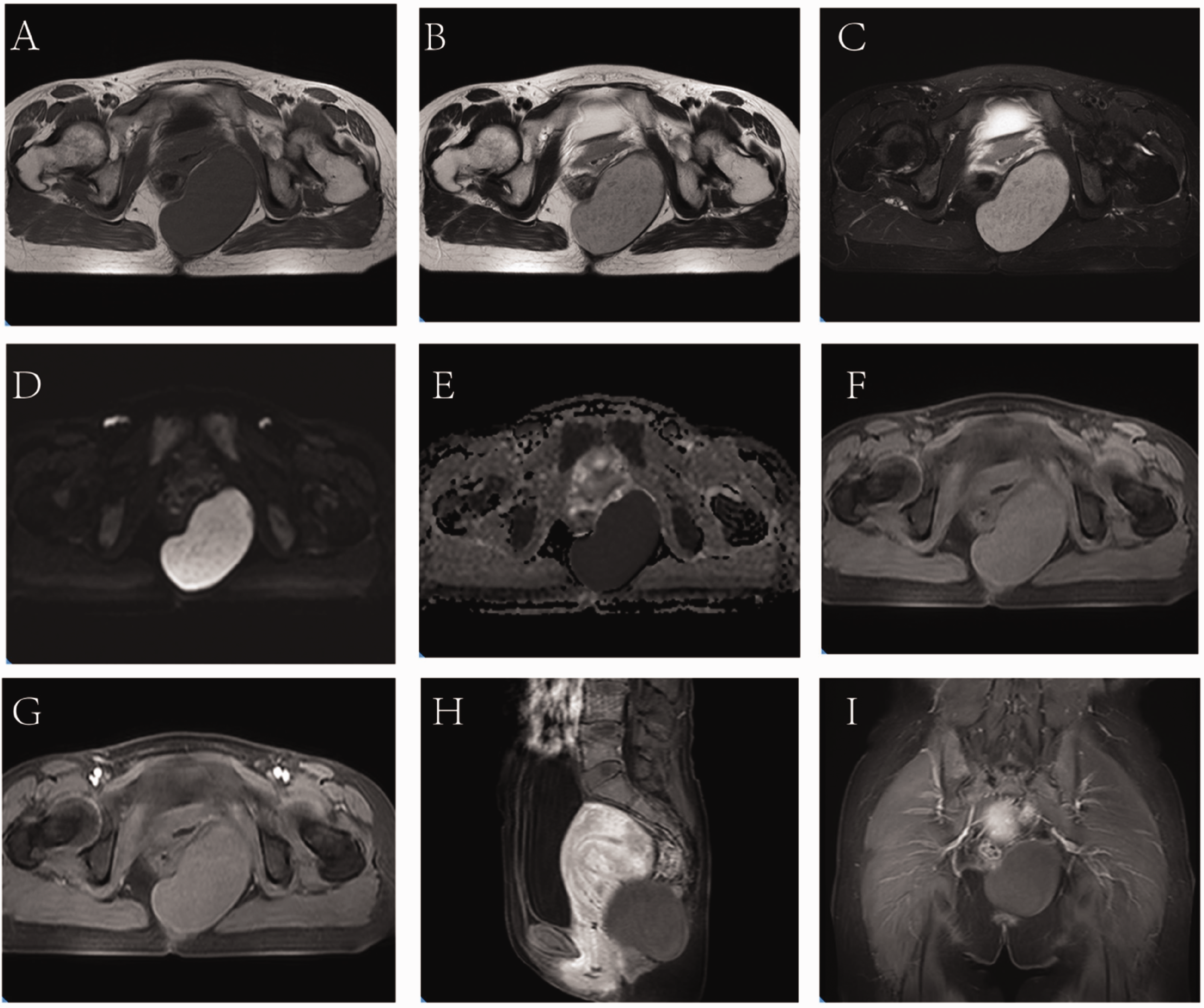
Preoperative magnetic resonance imaging features of a retroperitoneal dermoid cyst. (a) Axial T1-weighted imaging (T1WI) revealed an elliptical mass in the left side of the pelvis, measuring approximately 8.9 × 5.5 cm, with clear borders, smooth walls, and no internal septations. The mass exhibited low signal intensity with a rim of low signal intensity at the periphery (“black rim sign”, arrow). (b) Axial T2-weighted imaging (T2WI) demonstrated the heterogeneous high signal intensity of the mass, with multiple small round areas of low signal intensity and a rim of low signal intensity visible at the periphery. (c) Axial fat-suppressed T2WI demonstrated the heterogeneous high signal intensity of the mass, with no obvious decrease in signal. (d, e) Axial diffusion-weighted image (DWI) demonstrated high signal intensity and an apparent diffusion coefficient (ADC) map demonstrated low signal intensity, indicating restricted diffusion. (f) Axial fat-suppressed T1WI revealed no obvious decrease in signal and (g–i) contrast-enhanced axial, sagittal, and coronal images, respectively, revealed no enhancement of the solid portion of the mass but a thin peripheral rim of enhancement surrounding the wall of the cystic portion. The mass exhibited a well-defined margin with surrounding organs.
After admission, the patient underwent exploratory laparotomy under general anesthesia. An enlarged and irregularly shaped uterus was observed intraoperatively, with an adenomyoma-like protrusion measuring approximately 4 × 4 cm on the posterior wall. Both adnexa appeared normal. A palpable cystic mass measuring approximately 8 × 8 × 7 cm was also identified in the left retroperitoneum. A gynecologist excised the uterine adenomyoma, after which the general surgeon resected the left retroperitoneal mass. During the resection, viscous tissue with adipose characteristics was observed to flow out from the cystic mass.
The tumor was situated in the ischiorectal fossa, extending upward to the level of the S5 sacrum and downward to the middle of the gluteus maximus, with its lower edge approaching the contour line of the skin of the buttocks. It was nestled deep within the pelvis and close to critical structures such as the rectum, ureter, and bladder, and enveloped by a complex tangle of blood vessels and nerve networks. Its narrow and deep anatomical location restricted the surgical operability and visual accessibility, rendering complete tumor removal highly challenging. Following communication with the patient’s family during the procedure, a pararectal-transabdominal combined surgery was chosen. The procedure began by locating the base of the abdominal tumor and then incising along the rectum to create a new pathway. This new route was integrated with the original abdominal surgical approach, allowing for the gradual dissection and removal of the tumor. After surgery, pelvic drainage and a rectal tube were placed to facilitate drainage and maintain intestinal patency. The drainage tube was removed at 7 postoperative days. Postoperative pathological examination confirmed the diagnosis of a retroperitoneal dermoid cyst (Figure 2) and a uterine adenomyoma (Figure 3). The patient showed good postoperative recovery and remained recurrence-free within 1 year of follow-up.

Postoperative pathological examination of a dermoid cyst. All images stained with hematoxylin and eosin. (a, b) Mature squamous epithelium; (c, d) sebaceous glands, hair follicles, and adipose tissue. (a, c) ×4 and (b, d) ×10.

Postoperative pathological examination revealed uterine adenomyoma, with endometrial glands and stroma observed within the myometrium of the uterine wall. (a) ×4 and (b) ×10. Hematoxylin and eosin staining.
Verbal informed consent was obtained from the patient for this case report, and all procedures adhered to the ethical standards set by the institution and/or national research committee, as well as the principles outlined in the revised Helsinki Declaration of 2013. This study was approved by the Ethics Committee of Binhai County People’s Hospital. The reporting of this study conforms to CARE guidelines. 1
Discussion
Uterine adenomyomas represent benign tumors characterized by the infiltration of endometrial tissues into the myometrium, and their coexistence with a retroperitoneal dermoid cyst is rare. The etiology of retroperitoneal dermoid cysts remains poorly understood and mature cystic teratomas are often regarded as the same type of tumor; however, the term “dermoid cyst” typically refers to cysts composed primarily of a single tissue type, predominantly skin and its appendages, whereas a “mature cystic teratoma” encompasses cysts containing a broader array of tissue types derived from all three germ layers. Various hypotheses have been proposed to elucidate their origins,2–6 and there are several mainstream hypotheses regarding the histogenetic mechanism of mature cystic teratomas. The ectopic germ cell theory suggests that retroperitoneal dermoid cysts may originate from the aberrant differentiation and migration of primordial embryonic tissues during fetal development, which could lead to abnormal fusion of skin and peritoneal tissues in the retroperitoneal region, culminating in cyst formation. 7 Alternatively, the residual maternal cell hypothesis posits that primordial skin cells in the retroperitoneal region are left behind during early embryonic development and subsequently evolve into cysts. Thirdly, inflammatory reactions play a pivotal role in the development of many tumors and may contribute to the formation of retroperitoneal dermoid cysts. 8 Inflammation could activate maternal cells and stimulate ectopic tissue proliferation, thus promoting cystogenesis. Retroperitoneal dermoid cysts are relatively rare and their histological mechanism of occurrence is still unclear, but it may be related to the mechanism of mature teratoma development.
The manifestations and clinical characteristics of retroperitoneal dermoid cysts vary widely among individuals. Retroperitoneal dermoid cysts are often asymptomatic if they do not exert pressure on surrounding organs, and may thus only be detected incidentally during routine medical examinations or even at autopsy.9–10 Alternatively, patients may have abdominal symptoms, including abdominal pain, distension, and discomfort, typically intermittent and exacerbated following activity or meals, with symptom severity correlated with cyst size and location. 11 Some patients may exhibit mild symptoms of peritoneal irritation, such as tenderness or rebound pain, following cyst rupture, due to stimulation of the surrounding tissues by the contents of the cyst.12–14 Retroperitoneal dermoid cysts in the abdominal region can also elicit gastrointestinal symptoms, such as indigestion, loss of appetite, nausea, vomiting, and, in cases involving the lower abdomen, constipation and rectal bleeding.15,16 Finally, patients may have neurological symptoms resulting from nerve root compression by large dermoid cysts near vertebral bodies. 17 The clinical presentations of retroperitoneal dermoid cysts thus manifest differently across cases.
Gynecological retroperitoneal masses are relatively uncommon and often lack specific clinical manifestations, and may sometimes be misdiagnosed as pelvic masses originating from adnexal sources. Reported cases include patients initially suspected to have pelvic masses but later diagnosed with uterine fibroids, retroperitoneal fibrosis, and retroperitoneal dermoid cysts. 18 Nonetheless, surgical intervention remains the preferred treatment for pelvic masses, aligning with the treatment principles for retroperitoneal masses.
Retroperitoneal dermoid cysts are indeed rare and their radiological diagnosis poses challenges, because of limited experience of these lesions. Typically, retroperitoneal dermoid cysts are situated posterior to the lumbar vertebrae between the bilateral iliac muscle crests, and may extend into the posterior pelvic region, occasionally abutting the kidneys. This unique localization can lead to diagnostic confusion. A retroperitoneal teratoma was initially misidentified as an adrenal cyst in an 18-year-old female patient, 19 and a retroperitoneal dermoid cyst in another patient was initially suspected to be a solid pseudopapillary tumor of the pancreas but was later confirmed after surgery. 20 In 2021, a case report described a 12-year-old boy presenting with right rib pain in whom palpation revealed a painless, well-defined mass in the right lumbar region. Computed tomography also detected a clearly uneven mass in the right kidney area, measuring 11.5 × 11 cm. Postoperative diagnosis confirmed a retroperitoneal dermoid cyst containing fat and soft tissue degeneration, as well as calcification. 21 Notably however, the absence of specific radiographic features such as calcification and air-fluid levels in certain retroperitoneal dermoid cysts makes them difficult to distinguish from other retroperitoneal fat lesions, such as liposarcomas. This is highlighted by a previous case report in which the preoperative suspicion was “retroperitoneal liposarcoma,” but postoperative diagnosis confirmed a retroperitoneal dermoid cyst. 10 Dermoid cysts typically manifest as cystic or oval-shaped lesions with well-defined borders and variable sizes, ranging from a few centimeters to tens of centimeters. Internally, they often display hypoechoic characteristics with low density and occasional internal septations. The cyst contents may include fat, cartilage, or hair,2,10,22 and the cyst wall tends to be thin, ranging from 1 to 3 mm. Retroperitoneal dermoid cysts typically exhibit clear demarcations from surrounding structures such as the lumbar vertebrae, kidneys, and adrenal glands, with no evidence of infiltration or invasion. 10 In the current case, MRI revealed a cystic lesion with distinct borders and a smooth wall in the left pelvic floor.
The management of postperitoneal dermoid cysts is generally based on the patient’s clinical symptoms, the size and location of the cyst, and the physician’s judgment. Complete surgical removal is the preferred treatment in cases with severe symptoms, continuous cyst enlargement, or the risk of complications. 23 Complete resection of the cyst is the primary aim of surgery, thereby protecting and repairing the surrounding tissues. Both abdominal and laparoscopic approaches can be applied, while a combination approach with a pararectal route may be considered in cases of deep-seated or large cysts. 24 The challenging location of postperitoneal dermoid cysts however, adjacent to the intestines and ureters, increases the surgical difficulty and the risk of associated injuries. Careful identification of the anatomical structures, preventing injuries, and applying the techniques used in laparoscopic surgery for endometriosis, including the preoperative placement of bilateral ureteral stents, can thus help to identify and protect the ureters. 25 Furthermore, the potential for significant fluid leakage and the development of adhesive and chemical peritonitis warrants the use of postoperative drainage. 26 In some situations, intraoperative irrigation with diluted povidone-iodine solution may be used to remove extravasated adipose tissue within the cystic cavity; however, evidence to support this practice is currently lacking.
A comprehensive medical diagnostic and treatment process is paramount for disease prevention, in which each step directly affects the health of the patient. In the current case, the preoperative administration of G-CSF and selection of laparotomy as the surgical approach were both justified. Regarding the rationale for preoperatively administering G-CSF, the patient exhibited a low white blood cell count, possibly increasing the risk of perioperative infection. Considering that the patient had no history of hematological diseases and the probable benign nature of the leukopenia, preoperative G-CSF administration was a prudent course of action to help increase the white blood cell count and prevent perioperative infections. Furthermore, regular postoperative hematological reviews and specialist follow-ups are required to monitor the patient’s white blood cell count and overall hematological status, to ensure that the white blood cell count remains within a reasonable range or to help reveal and track the potential reasons for a decreased white blood cell count.
We also considered the rationale for adopting laparotomy. Preoperative radiographic investigations such as MRI can provide significant information on diagnostic positioning for retroperitoneal masses; however, in cases where malignancy cannot be eliminated, a comprehensive laparotomy may be a justifiable course of action. This procedure provides the surgical team with good visibility and operational space to allow the complete excision of possible malignancies. Although laparoscopy has advantages, including minimal trauma and faster recovery times, incomplete procedures can result in metastasis or residual cancer cells if the mass is malignant, adversely affecting patient prognosis. It is therefore vital to prioritize the prevention and complete removal of potential malignancies during the diagnostic and treatment processes.
Percutaneous drainage can be an alternative treatment option in cases where surgery is not feasible or well-tolerated 27 ; however, this method is not recommended for postperitoneal dermoid cysts because of their predominant fatty content, which can result in catheter occlusion. Moreover, malignant potential cannot be completely ruled out, and the risk of tumor dissemination should be taken into account when considering drainage or biopsy. 23 For asymptomatic cases with small cysts, the progression and symptomatology of the cysts can be evaluated by close observation and follow-up. Furthermore, other less common treatment modalities, including injection of an intracystic sclerosing agent, can be considered, based on the circumstances of individual patients, taking inspiration from the management of simple renal cysts and giant hepatic hemangiomas.28,29
Conclusion
This case report highlights the importance of considering a postperitoneal origin for pelvic masses with ambiguous diagnostic findings. In clinical settings, the differential diagnosis and treatment planning of benign and malignant postperitoneal lesions should be carefully considered.23,30
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241255810 - Supplemental material for Retroperitoneal dermoid cyst complicated with uterine adenomyoma: a case report and literature review
Supplemental material, sj-pdf-1-imr-10.1177_03000605241255810 for Retroperitoneal dermoid cyst complicated with uterine adenomyoma: a case report and literature review by Yanhua Zhang, Hailing Liu, Wenjing Hou, Hui Cheng, Feng Wang, Lingyan Zhang, Jianbo Zhou, Feng Han and Weipei Zhu in Journal of International Medical Research
Footnotes
Acknowledgements
The authors thank Binhai County People’s Hospital for providing the tissue samples and medical records. We thank Bullet Edits Limited for linguistic editing and proofreading of the manuscript.
Authors’ contributions
Yanhua Zhang and Weipei Zhu authored the paper. Hailing Liu, Wenjing Hou, and Feng Han conducted radiological and pathological analyses. Hui Cheng, Feng Wang, Lingyan Zhang, Jianbo Zhou, and Yanhua Zhang performed the surgical procedures. All authors have reviewed and approved the final manuscript
Availability of data and materials
The datasets used and/or analyzed in the present study are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare that they have no competing interests.
Ethics approval and consent to participate
Informed consent was obtained from the patient for publishing this case report. This case report was exempted from ethical review with the approval of the Ethics Committee of the People’s Hospital of Binhai County. This case report follows the CARE guidelines.
Funding
This work was supported by the China Health Promotion Foundation, under the funding of the Public Hospital High Quality Development Scientific Research Public Welfare Project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.