
Abstract
Objective
To investigate the potential association between the ratio of the second digit length to the fourth digit length (2D:4D) and schizophrenia, to provide evidence regarding the pathogenesis of schizophrenia.
Methods
In this study, we enrolled 843 patients with schizophrenia (387 men and 456 women), all of whom met the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV), and 1050 normal healthy controls (477 men and 573 women). The digit lengths of both hands were measured in all subjects and the 2D:4D ratio was analyzed.
Results
In the healthy controls, the 2D:4D ratio was sexually dimorphic, with a larger value in women than in men. In addition, the 2D:4D ratio in the schizophrenia patients was significantly larger than in the healthy controls. The 2D:4D ratio of the right hand was more sexually dimorphic than the left hand. Furthermore, the difference in 2D:4D ratios between the male patients and male controls was significantly larger than in their female counterparts.
Conclusions
By analyzing the 2D:4D ratio and considering alternative factors related to schizophrenia, our findings support the hypothesis that there are abnormal cerebral conditions in schizophrenia patients.
Introduction
Schizophrenia is a serious and common mental illness, 1 with a prevalence as high as 1%. The resulting mental disability seriously affects the quality of life of patients and their families, with the disease burden being ranked fourth among various diseases. 1 The etiology of schizophrenia is complex, with diverse clinical manifestations. Investigations into the etiology and pathogenesis of schizophrenia have been a main focus of the psychiatric field.
The neurodevelopmental hypothesis of schizophrenia suggests that genetic or environmental factors (or an interaction between the two) may cause issues during both synapse pruning and correction and neurogenesis regulation in the adolescent brain. 1 This may lead to the emergence of psychiatric symptoms and other mental illnesses with onset in young adults, including schizophrenia. In line with this hypothesis, neurodevelopmental disorders are now generally considered to be a main cause of schizophrenia. Many features of schizophrenia (age of onset, epidemiology, neuropathology, and clinical manifestations) suggest that abnormal cerebral conditions during brain development can lead to impaired and asymmetric features in brain structure and function, which relate to the pathogenesis of this disease.1,2
Gonadal hormones, including testosterone and estrogen, are important for brain development. 1 In particular, testosterone has major effects on processes such as neuronal migration and synaptogenesis, 2 which are manifested in sex differences in motor, cognitive, and linguistic abilities. 3 Kimura et al. 4 reported that gonadal hormones play an organizational role in the prenatal development of individuals, and they also affect different brain regions, brain and body asymmetry, sexual orientation, and cognitive development.
In 2010, Chura et al. 5 demonstrated that testosterone levels before birth are positively correlated with right asymmetry of the posterior corpus callosum; that is, higher testosterone levels are related to a greater right-side volume of the brain compared with the left side. We hypothesize that intrauterine testosterone in the embryonic phase can stimulate the development of certain brain regions in the right hemisphere of the brain, while simultaneously having the opposite effect in the left hemisphere, resulting in abnormal cerebral lateralization. Autopsy and structural brain imaging studies suggest that schizophrenia patients have reduced or reversed asymmetry of brain structures. 6 A meta-analysis of brain anatomy also revealed that schizophrenia patients are more likely to have reversed cerebral torque and have reduced asymmetry in the temporal plane and lateral fissure. 7 Compared with normal controls, both Crow et al. 8 and Daftary et al. demonstrated that patients with schizophrenia exhibit right-sided lateralization in the parietal and temporal lobes. 9
The ratio of the second digit length (2D) to the fourth digit length (4D) has garnered attention as an indicator of testosterone levels during embryonic development. The 2D:4D ratio is determined during embryogenesis 10 and does not present substantial changes after birth.10,11 The development of the 2D:4D ratio is influenced by sex hormone levels during embryonic development, including the balance between estrogen and testosterone. 12 The digit ratio is sexually dimorphic and men typically have lower 2D:4D ratios than women, suggesting that intrauterine testosterone during embryonic development stimulates 4D growth, while female hormones stimulate 2D growth. Nevertheless, it remains possible that the 2D:4D ratio may vary among different individuals or specific sub-populations. In addition, studies have shown that the human 2D:4D ratio of the right hand is more affected by sex hormones than the left hand, 10 and similar results have also been reported in other mammals. 13 This observation therefore suggests that the right-hand 2D:4D value may be more sensitive to the effects of prenatal androgen levels.
The 2D:4D ratio therefore acts as a morphological index that is correlated with embryonic testosterone levels. As an index that is easily measured and does not change after birth, further investigation is warranted into whether 2D:4D values correlate with the development of schizophrenia. This study therefore analyzes the 2D:4D ratios of schizophrenia patients and normal controls, and subsequently explores the potential association between 2D:4D ratios and schizophrenia.
Material and methods
Study subjects
Schizophrenia patients
The inclusion criteria were as follows: (1) aged 16 to 60 years; (2) voluntary participation in this study, with written informed consent; and (3) met the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) diagnostic criteria for schizophrenia. 14
Exclusion criteria were as follows: (1) other organic brain diseases, neurological diseases, or severe endocrine or metabolic diseases; (2) diagnosis was complicated with other DSM-IV axis-I and -II diseases (e.g., mood disorders, substance-related disorders, or mental retardation); and (3) unilateral or bilateral physical disability.
Healthy controls
Inclusion criteria were as follows: (1) aged 16 to 60 years; (2) normal social functioning (e.g., subjects can go to work or school normally, and were not retired because of illness) with normal capabilities and responsibilities; and (3) voluntary participation in the study, with written informed consent. Both the schizophrenia patients and healthy controls were from a Han Chinese population.
Exclusion criteria were as follows: (1) DSM-IV axis-I and -II diseases; (2) taking antipsychotic drugs, antidepressants, benzodiazepines, or other drugs that affect the central nervous system; (3) a history of mental illness or a family history of mental illness within three generations of both parental lines; 4) organic brain diseases; (5) color blindness, color weakness, stuttering, deafness, or mental retardation; and (6) a history of head injury.
Measurement methods
The connection site between the finger and the palm was used to find the lowest fold line (that is, the line closest to the palm). Using the midpoint of this fold line as the starting point of measurement, the long axis of the rule was placed parallel to the finger to measure its length. Vernier calipers were used to measure the finger length in centimeters, and the level of preciseness was set at 0.01 cm. To ensure the consistency of results, all finger length measurements were completed by two psychiatrists. Both psychiatrists were trained in the measurement methods, and internal consistency tests were conducted prior to the measurements being taken. The intra-group correlation coefficient was greater than 0.7.
Statistical analysis
All data were analyzed using SPSS for Windows, Version 21.0 (IBM Corp., Armonk, NY, U.S.). The results are expressed as the mean ± standard deviation (SD). The independent sample t-test and chi-squared test were used to compare differences between two groups. All analyses were performed using bilateral tests, and a P value of less than 0.05 was considered to be statistically significant. This experiment was reviewed and approved by the Ethics Review Committee of West China Hospital, Sichuan University.
Results
Demographic data
In this study, we enrolled 843 schizophrenia patients who met the DSM-IV criteria (387 men and 456 women). In addition, 1050 healthy controls were also recruited (477 men and 573 women). The general demographic data from all subjects are shown in Table 1. There were no significant differences in age or sex ratio between the schizophrenia patients and healthy controls. The education levels of the schizophrenia patients were significantly lower than those of the healthy controls (t = 0–13.31, P < 0.001).
Demographic data of the enrolled subjects.

Sexual dimorphism in 2D:4D ratios
The left and right 2D:4D ratios were significantly larger in the healthy female controls compared with their male counterparts (P < 0.05). In the schizophrenia patients, the 2D:4D ratio of the right hand was significantly larger in the female patients compared with their male counterparts (P < 0.05) (Table 2).
2D:4D ratios of males and females.
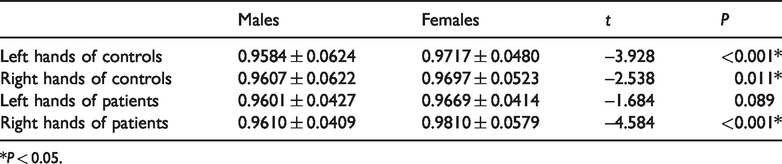
*P < 0.05.
Comparison of the 2D:4D ratios between hands
In both the healthy controls and schizophrenia patients, there was no significant difference in the overall mean 2D:4D ratio between the left and right hands. The right-hand 2D:4D ratio was significantly larger than the left-hand 2D:4D ratio in the female schizophrenia patients (P < 0.05). There was no significant difference in 2D:4D ratios in the male patients (Table 3).
2D:4D ratios of left and right hands.

*P < 0.05.
Comparison of 2D:4D ratios between schizophrenia patients and healthy controls
The 2D:4D ratios of the right and left hands were significantly larger in the schizophrenia patients than in the healthy controls (both P < 0.05). Within the same sex, the female schizophrenia patients had a significantly larger right-hand 2D:4D ratio than the female healthy controls (P < 0.05). In addition, the 2D:4D ratios of both the left and right hands of the male schizophrenia patients were significantly larger than those of the male healthy controls (P < 0.05) (Table 4). Moreover, the difference in 2D:4D ratio between the male schizophrenia patients and healthy controls was significantly larger than between the female schizophrenia patients and healthy controls (Figure 1).
2D:4D ratios of patients and controls.

*P < 0.05.

2D:4D ratios of both hands between schizophrenia patients and healthy controls.
Discussion
Our study demonstrated that the 2D:4D ratio is sexually dimorphic in normal controls, with a larger 2D:4D ratio in women than in men. This finding is consistent with many previous studies, and also supports our hypothesis that maternal intrauterine androgen (testosterone) in the embryonic stage can stimulate the growth of the fourth finger, whereas estrogen stimulates the growth of the second finger. 15
Previous studies of 2D:4D values in schizophrenia have given inconsistent results. Goldstein et al. 16 reported that female, but not male, schizophrenia patients have lower 2D:4D values compared with the normal population. Another study, by Grimshaw et al., 17 found that men and women with schizophrenia have higher 2D:4D values than normal controls, while Jabeen et al. 18 reported that both men and women with schizophrenia have so-called “feminized” 2D:4D ratios (2D ≥4D). Furthermore, Hajek et al. 19 demonstrated that sexual dimorphism in 2D:4D values is disrupted in adolescent patients with schizoid personality disorder compared with the normal population, suggesting that prenatal sex hormone levels are also a risk factor for this disease. In addition, Honekopp et al. 20 reported that primary symptoms in schizophrenia patients are associated with low 2D:4D values and low 2D:4D asymmetry coefficients. However, no abnormalities were found in related studies of populations with a high risk of schizophrenia. 21
In the present study, the 2D:4D ratios of the left and right hands were 0.958 ± 0.062 and 0.961 ± 0.062 in normal men and 0.972 ± 0.048 and 0.970 ± 0.052 in normal women, respectively. A large-sample study from the United Kingdom reported the 2D:4D ratios of the left and right hands as 0.985 ± 0.05 and 0.984 ± 0.05 in men and 0.993 ± 0.05 and 0.994 ± 0.05 in women, respectively. Our digit ratios are therefore slightly lower than those of previous findings.
Littlemore et al. 22 reported that, although 2D:4D values are sexually dimorphic, the sex difference in 2D:4D ratios is much smaller than the sex difference in testosterone levels in fetal amniotic fluid. In addition, the sex difference in 2D:4D values is approximately 0.25 SDs, whereas that of testosterone levels in fetal amniotic fluid is much higher, at approximately 1.9 SDs. These differences suggest that sex hormone levels in the amniotic fluid have limited effects on the 2D:4D ratio; thus, the 2D:4D ratio is likely also influenced by many other factors.
At present, the widely recognized view of schizophrenia etiology is that the pathogenesis of schizophrenia is not caused by a single factor, but rather by the combined impact of genetic, environmental, and multiple other factors. 23 There are therefore a wide variety of methods that can be used to investigate the biological basis of schizophrenia pathogenesis.
Many studies have demonstrated that embryonic neurodevelopmental disorders are associated with the pathogenesis of schizophrenia, 24 , 25 suggesting that some prenatal factors should be investigated to better understand this pathogenesis. In addition, large amounts of evidence suggest that schizophrenia patients have reduced or reversed hemispheric structural and functional lateralization. 9
In the study of hormones, the theory of androgens suggests that hemispheric lateralization occurs early in nervous system development, and reflects prenatal androgen/estrogen hormone levels. 3 However, ethical considerations mean that it is difficult to directly measure intrauterine androgen/estrogen levels in the embryonic stages. However, the 2D:4D ratio can be used as an indicator of intrauterine sex hormone levels in the embryonic stages, and its relationship with schizophrenia warrants investigation.
In psychiatric disorders, recent studies have revealed that a low 2D:4D ratio is associated with social difficulties in children with autism spectrum disorder. 26 In addition, Manning et al. 26 reported that a low 2D:4D ratio is associated with the symptoms of attention deficit hyperactivity disorder, although Lemiere et al. 27 presented contrasting results. It has also been reported that a low 2D:4D ratio is associated with alcohol dependence. 28
In our study, compared with the normal controls, schizophrenia patients had higher 2D:4D ratios, suggesting that the 2D:4D ratio in the patients was feminized, which is consistent with many previous studies. Manning et al. 29 reported that, in schizophrenia patients from Asian populations, the male patients had higher 2D:4D ratios than the normal controls. In addition, Jabeen et al. 18 demonstrated that both male and female schizophrenia patients had higher 2D:4D ratios compared with normal controls; that is, the patients exhibited a feminized digit ratio. Grimshaw et al. 17 also reported that the 2D:4D ratio was feminized in both male and female schizophrenia patients. Furthermore, Sommer et al. 30 analyzed the 2D:4D ratio in a Chinese population in Shanghai and revealed that the 2D:4D ratio was positively correlated with schizoid personality traits in the normal population, suggesting that a high 2D:4D ratio may be a predisposing factor of schizophrenia. Considering the relationship between 2D:4D ratios and embryonic intrauterine sex hormone levels, the results from these studies suggest that intrauterine androgen levels may have a protective effect on the pathogenesis of schizophrenia, whereas estrogen levels may have the opposite effect.
In the present study, we also revealed that the sex difference in left-hand 2D:4D ratios in schizophrenic patients was smaller than in normal controls. Sexual dimorphism in 2D:4D ratios is a result of the effects of prenatal intrauterine sex hormone levels, particularly testosterone. The schizophrenia patients showed a smaller sex difference than the normal controls, suggesting altered intrauterine hormone levels in schizophrenia patients in the embryonic stages. However, other studies of the 2D:4D ratio and cerebral lateralization in schizophrenia have revealed contrasting findings.
Honekopp et al. 20 reported that women with schizophrenia had a lower 2D:4D ratio compared with same-sex normal controls. They also calculated the 2D:4D lateralization index (LI), as LI = (left-hand 2D:4D–right-hand 2D:4D)/(left-hand 2D:4D + right-hand 2D:4D), and found that the 2D:4D LI of male schizophrenia patients was lower than that of male controls. Additionally, Goldstein et al. 16 demonstrated that women with schizophrenia had lower 2D values, though they did not calculate 2D:4D values. Hrabooszky et al. 31 compared the 2D:4D ratio between a high-risk schizophrenia group and normal controls, and they did not reveal any significant differences. Mendrek et al. 32 also reported no differences between populations at high risk of schizophrenia and normal controls. Moreover, in a study on adolescents with schizoid personality disorder, there were sex differences in the 2D:4D ratio (smaller 2D:4D ratio in men than in women) of normal controls, but no sex differences in patients with schizoid personality disorder. 19
The 2D:4D ratio is an interesting indicator of schizophrenia. The reasons for the inconsistent findings in the present and previous studies may be related to different sample sizes, ethnic groups, and research methods (e.g., some previous studies used the 2D:4D ratio as an index for analysis, whereas others only analyzed the 2D:4D ratio of one hand). The present study indicated that schizophrenia patients are subjected to abnormal levels of intrauterine sex hormones in the embryonic period, supporting the view that schizophrenia patients have abnormal cerebral lateralization. Our results suggest that the presence of abnormal cerebral lateralization in schizophrenia should be further investigated from a neurodevelopmental perspective.