
Abstract
Objective
This study investigated the correlations of digit ratio (relative length of second and fourth fingers, 2D: 4D) and muscular strength with the progression of chronic obstructive pulmonary disease (COPD).
Methods
In total, 164 patients with COPD were enrolled in this prospective study. In all patients, the following parameters were measured: body compartments, pulmonary function, digit ratio (i.e., 2D: 4D), muscle function, and levels of partial pressure of oxygen and partial pressure of carbon dioxide in arterial blood.
Results
The right-hand digit ratio (R2D: 4D) was associated with dominant hand muscle dysfunction, non-dominant hand muscle dysfunction, and inspiratory muscle dysfunction. Logistic regression analysis showed that right-hand 2D: 4D (odds ratio [OR] = 0.01) and dominant hand muscle dysfunction (OR = 5.60) were significantly associated with past hospital admission. After adjustment for forced expiratory volume in 1 second, the following factors were associated with present acute exacerbations: right-hand 2D: 4D (OR = 0.01), dominant hand muscle dysfunction (OR = 3.83), expiratory muscle dysfunction (OR = 3.80), and inspiratory muscle dysfunction (OR = 3.61).
Conclusions
Lower digit ratio may be associated with higher prevalence of muscle dysfunction. This factor could be used to identify patients with COPD who are at higher risk of acute exacerbation.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) exacerbation is clinically defined by worsening of dyspnea, increased sputum volume and/or change in sputum color, and new or worsened cough. 1 Peripheral muscle dysfunction may result in reduced exercise capacity. 2 Hence, there is increasing interest in identifying factors that affect exacerbation and that are linked to muscle dysfunction in patients with COPD. The ratio between the second and fourth digits (2D: 4D) is reportedly related to various parameters of athletic performance, which suggests that it may be a useful predictor of muscle mass, strength, and endurance. 3 However, with the exception of the study by Maddocks et al., 4 there is minimal evidence that muscle dysfunction may serve as a modifiable risk factor in patients with COPD. This study was performed to explore the role of digit ratio in muscle dysfunction and acute exacerbations in patients with COPD.
Materials and methods
Participants
Patients with COPD were recruited from the Department of Feibing in the Fourth Affiliated Hospital of Xinjiang Medical University from March 2017 to December 2017. The inclusion criteria were as follows: (1) admission to the hospital due to exacerbations of COPD, or (2) a diagnosis of stable COPD and regular follow-up at the hospital. All patients were classified on the basis of clinical stability (present or absent). Patients were grouped on the basis of hospital admission history (none, present, or multiple), as follows: patients who attended regular hospital follow-ups, but never required hospital admission; patients with clinically stable COPD, defined as ≥3 months from the last exacerbation, who had a history of multiple hospital admissions during the previous year; patients admitted to the hospital for the first time with a diagnosis of acute exacerbation of COPD; patients with acute exacerbation who were admitted to the hospital on ≥3 occasions, in accordance with the 2017 guidelines from the Global Initiative for Chronic Obstructive Lung Disease. 5
Exclusion criteria were as follows: (1) a history of pneumonia, left heart failure, infection from any other organ, previous or present pulmonary embolism, and/or chronic systemic steroid therapy; (2) presence or suspicion of recent orthopedic or surgical diseases that could affect muscle structure and function; (3) lack of right-handedness, presence of skeletal dysplasias, or history of injury to the fingers; (4) refusal to provide informed consent.
This study was conducted in accordance with the tenets of the Declaration of Helsinki and approved by the Ethics Committee of Xinjiang Medical University and the Fourth Affiliated Hospital (Approval no: 201709601). Written informed consent was obtained from all participants.
Body compartment analysis
Body compartment was determined using bioelectrical impedance analysis. The Quantum II Bioelectrical Body Composition Analyzer (RJL Systems, Clinton Township, MI, USA) was used to assess multisystem diseases and myogenic changes. 6
Pulmonary function and blood sample analysis
All patients were diagnosed with COPD in accordance with international guidelines. 7 Based on forced expiratory volume in 1 second, patients were stratified into 2013 Global Initiative for Chronic Obstructive Lung Disease stages.
Forced spirometry, airway resistance, static lung volumes, and carbon monoxide diffusing capacity were assessed in all patients. Inspiratory and expiratory muscle strengths were assessed by determining maximal respiratory mouth pressures during voluntary maneuvers. Patients were instructed to perform maximal respiratory efforts with an occluded airway. Maximal inspiratory pressure was determined on the basis of maximal expiratory pressure, which was obtained from pulmonary residual volume and total lung capacity. Maximal inspiratory pressure and maximal expiratory pressure values were both assessed in absolute (cmH2O) and relative pressure values. Arterial blood was collected using conventional techniques. Briefly, a radial or femoral artery was punctured with a blood-gas needle containing heparin and saline; 1 mL of arterial blood was collected within the blood-gas needle, then mixed with heparin within the needle prior to analysis.
Grip strength measurement
Grip strength was measured using a dynamometer to record the maximal voluntary hand grip strength of finger flexors in both dominant and non-dominant hands during three consecutive maneuvers separated by 3-minute intervals. The maximal value of grip strength for each hand was used for the analysis. Absolute and relative values were analyzed in relation to the reference values. 8
Digit measurement
The 2D and 4D measurements were performed using a standard Vernier caliper (recorded to a precision of 0.01 mm) from the basal palmar crease of the finger to the tip. When two creases were visible at the base of the digit, the crease proximal to the palm was chosen. All measurements were performed twice by two investigators (both investigators were present during all measurements), and the mean value of the two measurements was used. 9
Statistical analysis
The normality of the distribution was analyzed by using the Shapiro–Wilk test. Data were compared by the t-test, Kruskal–Wallis test, and chi-squared test, as appropriate. Pearson-product moment correlations were used to assess the relationships of digit ratio with muscle strength and lung function. An unconditional multivariate logistic regression model was used to assess associations between muscle dysfunction and exacerbations of COPD, as well as between digit ratio and exacerbations of COPD, after adjustment for potential confounders. All statistical analyses were performed using SPSS Statistics, version 19.0 (IBM Corp., Armonk, NY, USA), with a two-sided significance level of p < 0.05.
Results
Patient characteristics
In total, 164 patients with COPD were recruited for this study. Of these 164 patients, 102 showed clinical stability, while 62 patients were admitted to the hospital due to acute exacerbation. Patients with acute exacerbation demonstrated lower forced expiratory volume in 1 second, compared with patients who had stable COPD (p < 0.01). Furthermore, patients with acute exacerbation who had multiple admissions exhibited lower fat mass, greater pulmonary residual volume, and lower capacity for transfer of lung carbon monoxide (p < 0.01 for all), when compared with patients who had stable COPD without previous admissions (Table 1).
Demographic and clinical characteristics, digit ratio, and muscle function measurements among patients with chronic obstructive pulmonary disease.

ap<0.05, p values correspond to comparisons with the stable COPD with no previous admission group; bp<0.01, p values correspond to comparisons with the stable COPD with no previous admission group.
Abbreviations: COPD, chronic obstructive pulmonary disease; TBW, total body water; FM, fat mass; FFMI, fat-free mass index; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; TLC, total lung capacity; RV, pulmonary residual volume; PaO2, partial pressure of oxygen; PaCO2, partial pressure of carbon dioxide; TLCO, transfer of lung carbon monoxide; KCO, carbon monoxide transfer coefficient; R2D: 4D, right-hand digit ratio; L2D: 4D, left-hand digit ratio; DoHGS, dominant hand grip strength; NDoHGS, non-dominant hand grip strength; PImax, maximal inspiratory pressure measured at the mouth (Muller maneuver); PEmax, maximal expiratory pressure measured at the mouth (Valsalva maneuver).
Digit ratio and muscle function measurements
Table 1 presents the digit ratio and muscle function measurements. There was a significant relationship between a history of multiple hospital admissions and right-hand 2D: 4D in patients with COPD. Furthermore, muscle dysfunction (reduced hand grip strength) was strongly associated with past and present exacerbations of COPD (p < 0.01) (Table 1). Specifically, dominant hand muscle dysfunction (p = 0.026), non-dominant hand muscle dysfunction (p = 0.048), and inspiratory muscle dysfunction (p = 0.015) were associated with right-hand 2D: 4D in patients with COPD (Table 2).
Relationship between main factors and 2D: 4D values.
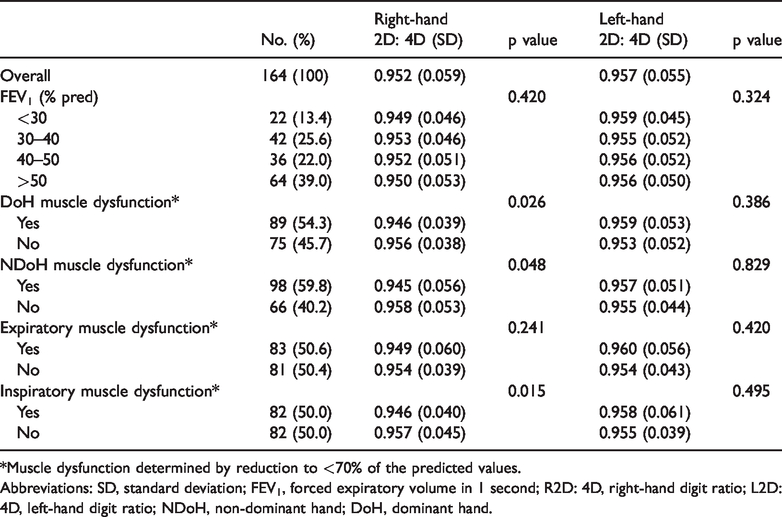
*Muscle dysfunction determined by reduction to <70% of the predicted values.
Abbreviations: SD, standard deviation; FEV1, forced expiratory volume in 1 second; R2D: 4D, right-hand digit ratio; L2D: 4D, left-hand digit ratio; NDoH, non-dominant hand; DoH, dominant hand.
Factors associated with hospitalizations and acute exacerbations
Individual parameters were evaluated using univariate analysis to identify associations with present and past hospitalizations. Right-hand 2D: 4D (p < 0.01), dominant hand muscle dysfunction (p < 0.01), and non-dominant hand muscle dysfunction (p = 0.03) were associated with an increased risk of multiple hospital admissions. Right-hand 2D: 4D and dominant hand muscle dysfunction (p < 0.01 for both) were significantly associated with past hospital admission after adjustment for forced expiratory volume in 1 second. Moreover, after adjustment for forced expiratory volume in 1 second, the following factors were associated with present acute exacerbations: right-hand 2D: 4D (p < 0.01), dominant hand muscle dysfunction (p < 0.01), expiratory muscle dysfunction (p = 0.04), and inspiratory muscle dysfunction (p < 0.01) (Table 3).
Logistic regression to identify factors associated with hospitalizations and acute exacerbations.

*Adjusted for forced expiratory volume in 1 second (FEV1).
Abbreviations: COPD, chronic obstructive pulmonary disease; R2D: 4D, right-hand digit ratio; L2D: 4D, left-hand digit ratio; OR, odds ratio; CI, confidence interval; DoH, dominant hand; NDoH, non-dominant hand.
Discussion
The exacerbation of COPD may be characterized by worsening airflow obstruction, as well as increased respiratory and systemic demand in the patient. 10 With respect to inspiratory muscles, a risk related to functional deterioration during exacerbation is the progressive recession of functional residual capacity due to dynamic air trapping. 11 In addition, systemic inflammation is associated with reduced muscle strength and exercise tolerance in patients with COPD. 12 Exacerbations due to inflammatory bursts are characterized by increased levels of inflammatory mediators in both sputum and plasma. 13
A prior study showed that digit ratio was associated with a sudden surge of testosterone in competitive situations and that low digit ratios were predictive of high aggression in competitive situations. 14 These emergency changes are presumably related to acute breathing and muscle disorders. Hill et al. 15 revealed relationships between digit ratio and cardiovascular efficiency. Specifically, digit ratio was associated with maximal oxygen uptake, velocity at maximal oxygen uptake, and maximum lactate concentration in 14-year-old boys. We suspect that these differences may be related to acute exacerbations in patients with COPD.
There were some limitations in this study. The endocrine system and biochemical mechanism were not investigated in a systematic manner, and should be the focus of future research. Our findings should be confirmed in large, multi-center, prospective studies.
In conclusion, lower digit ratio may be associated with an increased prevalence of muscle dysfunction; lower right-hand 2D: 4D may be useful for identification of patients with COPD who are at higher risk of acute exacerbation.
Footnotes
Acknowledgements
We thank the collaborators from the First Affiliated Hospital of Xinjiang Medical University, as well as the medical workers and the health center staff.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work is supported by the Natural Science Foundation of Xinjiang Uygur Autonomous Region (Grant No. 2018D01C194).