
Abstract
Objective
Clinicopathological features and surgical outcomes in patients with solid pseudopapillary neoplasm (SPN) of the pancreas were analysed.
Methods
Data regarding clinicopathological features, surgery and outcome for patients with SPN were retrospectively collected and analysed. Patients were followed-up by telephone interview.
Results
The study included 102 patients (89 females/13 males), 99 of whom underwent surgical resection. A total of 89 patients (87.3%) were followed-up (mean duration 26.98 months, range 2–95 months); 86 (96.6%) had no relapse or metastasis.
Conclusions
Surgical resection is the primary therapy for SPN, and results in a good prognosis.
Introduction
Solid pseudopapillary neoplasm (SPN) is defined by the World Health Organization as a pancreatic tumour with undetermined borderline or malignant potential and uncertain origin, 1 with an incidence of 1–3% of all pancreatic tumours.1–4 Despite improvements in SPN detection, diagnosis and reporting,4–6 misdiagnosis as pancreatic adenocarcinoma and lack of consensus regarding treatment remain major obstacles in disease management.5,7
Studies have shown that SPN usually occurs in young women,6,8 but clinical manifestations, pathological features and treatment modalities vary. The aim of the current study, therefore, was to analyse the clinicopathological characteristics and treatment outcomes of patients with SPN, retrospectively.
Patients and methods
Study population
This retrospective analysis included all patients with pathologically confirmed SPN 9 admitted to the Department of Oncology, Chinese People’s Liberation Army General Hospital, Beijing, China, between October 2001 and June 2010. Clinicopathological and treatment data were extracted from clinical records. Patients were followed-up at regular intervals by telephone interview until September 2010.
The Ethics Committee of the Chinese People’s Liberation Army General Hospital, Beijing, China approved the study, and all patients provided written informed consent prior to enrolment.
Immunohistochemistry
Immunohistochemical analysis of tumour tissue was performed using a streptavidin peroxidise-conjugated method, 10 using antibodies to chromogranin A, synaptophysin, neural endopeptidase (CD10), neural cell adhesion molecule (CD56), glucagon, vimentin and insulin (Santa Cruz Biotechnology, Santa Cruz, CA, USA). Immunohistochemical staining was analysed by two independent pathologists (L.J.W. and L.B.).
Results
The study included 102 patients with SPN (13 males/89 females; ratio 1 : 6.85); mean age 42.9 ± 14.6 years in males (range: 16–71 years) and 27.3 ± 11.6 years in females (range: 9–52 years).
Age distribution of Chinese patients with solid pseudopapillary neoplasm of the pancreas, stratified according to sex (n = 102).
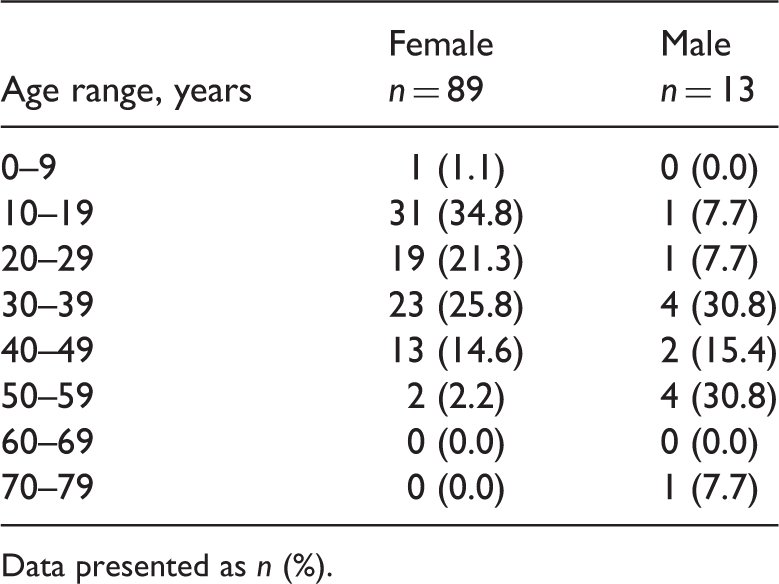
Data presented as n (%).
Clinical and pathological features of Chinese patients with solid pseudopapillary neoplasm of the pancreas.
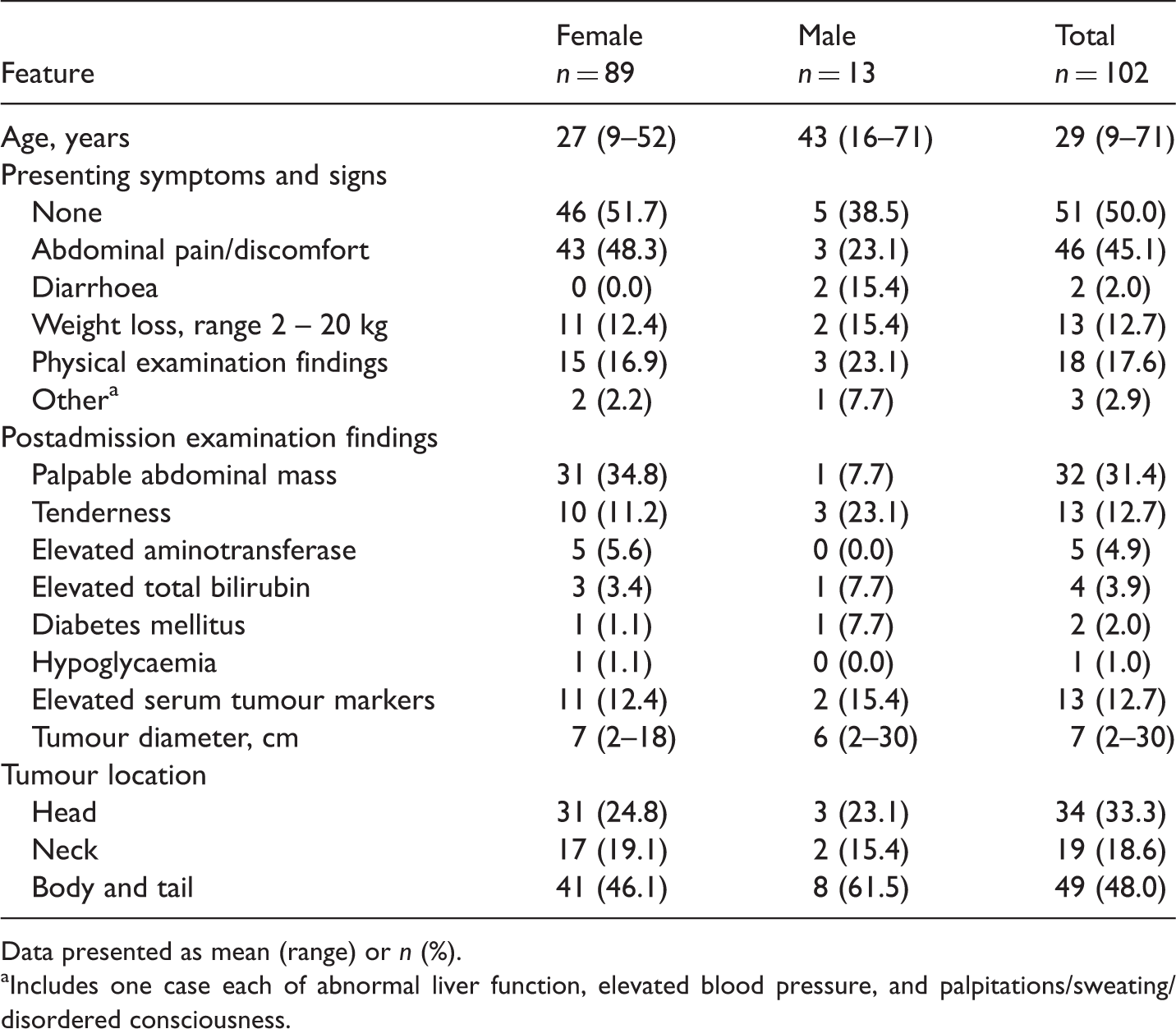
Data presented as mean (range) or n (%).
Includes one case each of abnormal liver function, elevated blood pressure, and palpitations/sweating/disordered consciousness.
Diagnosis was confirmed by imaging in 31 cases (30%). An additional 12 cases (12%) were thought to be pancreatic adenocarcinomas; the remaining 59 cases (58%) could not be definitively diagnosed. Typical abdominal ultrasonography findings were of a single nonhomogeneous hypoechoic space-occupying lesion or a cystic-solid lesion of irregular shape with a clear edge in the pancreatic area, inside which the arterial and venous flow spectrum could be explored. Common bile duct expansion could be detected in some cases. Plain computed tomography examinations generally revealed round or oval low-density space-occupying lesions (Figure 1a). Irregular enhancement was observed around the tumour edge during enhanced arterial scan, even in the absence of obvious intermediate enhancement. A few tumours were surrounded by punctate calcification. Magnetic resonance imaging identified a variety of tissue structures inside the tumour. Slight enhancement was observed during the arterial phase. Solid tumours gradually strengthened and cystic tumours were insignificantly enhanced during the portal venous and delayed phases (Figure 1b).
Cross-sectional imaging of a solid pseudopapillary tumour of the pancreas. (a) Axial computed tomography image showing round or oval low-density space-occupying lesions in the head of the pancreas (arrow). (b) Magnetic resonance image showing space-occupying lesions in the body and tail of the pancreas, and intrahepatic metastases (arrows).
Characteristics of surgery in Chinese patients with solid pseudopapillary neoplasm of the pancreas.

Data presented as n (%).
Includes five cases of pylorus-preserving pancreaticoduodenectomy.
Adequately controlled by symptomatic treatment.
A total of 89 patients (87%) were followed-up, for a mean of 27 months (range 2–95 months, median 22 months). Of these patients, 86 (97%) had no relapse or metastasis. Three patients died: one due to relapse and metastasis, one due to acute pulmonary embolism, and one (who did not undergo surgical resection) due to advanced disease progression. A single patient with hepatic, pulmonary and retroperitoneal lymphatic metastases received two cycles of gemcitabine + cisplatin + anti-EGFR antibody. Disease progression was reassessed and the chemotherapy regimen was changed to paclitaxel + carboplatin + anti-EGFR antibody. During chemotherapy, the patient had abdominal and lumbosacral pain, refused to continue chemotherapy, and was transferred to a local hospital for radiotherapy.
Immunohistochemical findings of tumour tissue samples from 91 Chinese patients with solid pseudopapillary neoplasm of the pancreas.

Discussion
This retrospective analysis of patients with SPN revealed that the majority were young women, with a gender ratio of 6.85 : 1 and a mean age of 29 years, which are higher rates than those reported by others.6–8,11 In accordance with other findings, 50% of the current patients were asymptomatic at presentation, while others presented with diarrhoea and abdominal pain, distension or masses.12,13 Since abdominal discomfort and pain are qualitative parameters, useful SPN markers are required.
Imaging is of limited value in the diagnosis of SPN because of the difficulty in distinguishing these from cystic or solid tumours. 9 The majority (58%) of patients in the current study could not be diagnosed by imaging alone, although this rate was lower than that reported elsewhere (80–90%). 14 In addition, abnormal liver function and elevated serum tumour markers did not allow definitive diagnosis of SPN in the current study.
Over 50% of the patients in the current study were found to have obvious tumour adhesion to surrounding tissues (mainly the spleen, duodenum, colon, stomach, greater omentum, bile duct, left kidney and liver) and three patients had metastatic disease. This finding is in accordance with other research 15 that SPN has high malignant potential, necessitating further investigation. A high percentage of tumours expressed CD56 and vimentin, but this may be simply representative of the diversity of exocrine, endocrine and epithelial origin of SPN. 12
The optimal treatment of SPN is surgical resection. 16 The present study included a variety of surgical procedures (including simple resection, distal pancreatectomy, pancreaticoduodenectomy and tumour resection with pancreaticojejunostomy) that were selected according to the tumour site. Due to the anatomical location of the pancreas and the tendency of tumour cells to invade major blood vessels of the abdominal cavity, SPN surgery should include resection and reconstruction of the portal vein or peripancreatic artery.17,18 Repeat surgery or metastasis resection can significantly prolong survival in cases of recurrence. 9
There is no evidence demonstrating a positive effect of postoperative adjuvant chemotherapy on prognosis of SPN.19–22 Further studies are required to investigate the benefits, if any, of postoperative neoadjuvant therapy on prognosis in SPN.
In conclusion, the primary therapy for SPN is surgical resection, and this results in a good prognosis for patients.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Beijing Medicine Research and Development Fund for independent innovation and promotion of the popularization of project (2007-3048).