
Abstract
Objective
Hemorrhage from the stump of the gastroduodenal artery (GDA) is a significant postoperative risk with pancreaticoduodenectomy (PD). Studies have shown that wrapping the GDA stump using the omentum or the falciform ligament can help prevent bleeding. We aimed to determine whether wrapping the GDA stump with the ligamentum teres hepatis (LTH) would reduce postoperative PD hemorrhage.
Methods
We retrospectively reviewed data for 148 patients who underwent laparoscopic pancreatoduodenectomy (LPD) at our hospital from November 2015 to September 2021. We compared perioperative data from 63 LPD patients without wrapping of the GDA (unwrapped group) and 85 whose GDA stumps were wrapped (wrapped group).
Results
There were no significant differences in the groups’ baseline characteristics. The postoperative GDA stump bleeding incidence was significantly lower in the wrapped group than that in the unwrapped group (7.9% vs. 0, respectively). There was also no significant difference in the incidence of other complications (intra-abdominal infection, postoperative pancreatic fistula (POPF), biliary fistula, and gastrointestinal bleeding).
Conclusion
Using the LTH to wrap the GDA stump during LPD can reduce bleeding from the GDA stump but not the incidence of other complications.
Keywords
Introduction
Pancreaticoduodenectomy (PD) is performed to treat pancreatic head and periampullary malignancies. 1 PD also involves resection, lymph node dissection, and digestive tract reconstruction.2,3 Bleeding from the gastroduodenal artery (GDA) stump is a significant risk after PD and may lead to the need for reoperation, or death.4–10 Bleeding is often caused by postoperative pancreatic fistula (POPF) and erosion of blood vessels owing to pancreatic fluid leakage or local inflammation.3,8,11–13 Recently, the use of somatostatin and octreotide has significantly decreased the bleeding incidence; 3 nevertheless, the incidence of massive bleeding caused by POPF remains high at 16% to 40%.10,14–16 POPF is unavoidable in PD;17–19 therefore, protecting the GDA stump from erosion caused by pancreatic fluid leakage is essential.
Wrapping the GDA stump using the omentum or the pedicled falciform ligament can help prevent bleeding.20–26 However, a recent study found that using the omentum and the pedicled falciform ligament to wrap the GDA stump is controversial. 26
We performed a retrospective cohort analysis to determine whether wrapping the GDA stump with the ligamentum teres hepatis (LTH) during LPD would reduce the incidence of bleeding.
Methods
We retrospectively analyzed data for patients who underwent LPD with vs without wrapping of the GDA stump at our hospital from November 2015 to September 2021. We compared baseline preoperative information, intraoperative variables, total hospital stay, and postoperative bleeding treatment between the groups. The reporting of this study conforms to the STROBE guidelines. 27
Ethics statement
This study was approved by the Medical Ethics Committee of Li Huili Hospital, Ningbo Medical Center (approval number: AF/SC-08/03.0). The clinical data were retrospectively registered on 5 November 2022. We obtained verbal informed consent from all patients for treatment and for publication of this report.
Preoperative data collection
Preoperative data comprised gender, age, body mass index, total bilirubin, transaminases, prothrombin time, globulin, and platelets (Table 1). Intraoperative variables comprised operation time, tumor size, intraoperative bleeding, blood transfusion, and death (Table 2). Postoperative complications comprised GDA stump bleeding, anastomotic bleeding, POPF, bile fistula, arterial stenosis, abdominal infection, delayed gastric emptying (DGE), time to first water intake, time to first food intake, time to first passage of flatus, and total hospital stay (Table 3).
Basic preoperative information of the patients in both groups.

BMI, body mass index; TBil, total bilirubin; AST, aspartate aminotransferase; ALT, alanine aminotransferase;
PT, prothrombin time; GLB, globulin; PLT, platelets.
Comparison of the intraoperative findings in the two groups of patients.

SD, standard deviation; IPMN, intraductal papillary mucinous neoplasm; NS, not significant.
Comparison of postoperative complications between the two groups.

Values are presented as n (%) or mean ± standard deviation.
GDA, gastroduodenal artery; DGE, delayed gastric emptying.
Main surgical points
The same surgeon performed all operations. Unified laparoscopic resection and standard anastomosis procedures were performed in all patients. The resection scope comprised the distal stomach (approximately 60% of the entire stomach), duodenum, head of the pancreas, uncinate process, gallbladder, and common bile duct. The sequence of anastomosis was pancreaticojejunostomy, biliojejunostomy, and gastrointestinal anastomosis. In pancreaticojejunostomy, we placed a suitable catheter stent into the pancreatic duct to support the duct, and the pancreatic duct mucosa was used to suture the jejunal mucosa. The wrapped group was distinguished from the unwrapped group, as follows: The LTH was retained in the unwrapped group. In the wrapped group, 8 to 12 cm of the LTH was preserved after being freed from the abdominal wall. The anterior side of the LTH was cut open and wrapped 360° around the common hepatic artery and GDA stump and fixed with a 3-0 barbed suture (Figure 1). Two drains were placed: one from the posterior side of the pancreaticoenteric anastomosis and the anterior side of the superior mesenteric vein on the left side of the abdomen; the other was placed on the posterior side of the pancreaticoenteric anastomosis on the right side of the abdomen.

Schematic diagram showing ligamentum teres hepatis (LTH) wrapping of the gastroduodenal artery (GDA) stump. (a) Freeing the ligamentum teres hepatis. (b, e) The anterior side of the LTH is cut open and (c, d, f, g) The common hepatic artery and GDA stump are wrapped 360°.
Postoperative treatment
The patients remained in the intensive care unit for at least 12 hours after surgery. When vital signs were stable, the patients were transferred to the general ward and given somatostatin 4 mL/hour (6 mg dissolved in 100 mL saline) by micropump injection for 3 days (when drainage amylase exceeded 2000 U/L; administration was sometimes extended depending on a patient’s symptoms.
Definition of complications
In accordance with the International Study Group of Pancreatic Surgery (ISGPS), postoperative POPF was classified as grade A, B, or C. 28 Bile fistula was defined as bile output >100 mL/day. 29 DGE was defined as the nasogastric tube remaining for more than 10 days with at least one of the following conditions: (I) repeat vomiting after removal of the gastric tube; (II) use of gastric motility agents for more than 10 days after surgery; (III) reinsertion of a nasogastric tube for decompression; or (IV) inability to resume oral food intake. 30 Patients were also diagnosed with DGE when they had nasogastric tube retention for less than 10 days, and DGE was confirmed by iodine imaging or upper abdominal computed tomography.
Statistical analysis
Continuous data were expressed as the mean ±standard deviation and compared using Student’s t-test for normally distributed data. Categorical variables were compared using the chi-square or nonparametric test (as appropriate). Statistical analysis was performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). P < 0.05 was considered statistically significant.
Results
We analyzed data for 148 patients who underwent LPD at our hospital from November 2015 to September 2021. We treated 63 patients (39 men and 24 women, mean age: 69.13 ± 8.96 years) without wrapping of the GDA (unwrapped group) and 85 patients (52 men and 33 women, average age: 68.12 ± 10.26 years) with wrapping of the GDA (wrapped group).
The baseline conditions did not differ between the groups of patients (Tables 1 and 2). We followed all patients preoperatively to 3 months after removing all drains; no patients were lost to follow-up. We successfully wrapped 85 patients. The average time of GDA stump wrapping was approximately 15 minutes, which was not long considering the total operation time.
After surgery, 10 patients experienced GDA stump hemorrhage in the unwrapped group (6.8% (10/148) of all surgeries). Two cases were found on the third postoperative day, one on the fourth postoperative day, one on the fifth postoperative day, and one on the seventh postoperative day. No GDA stump hemorrhage occurred in the wrapped group (P = 0.013) (Table 3). Because of our limited early experience managing intra-abdominal hemorrhage after PD, we found four of the hemorrhages by reoperation, whereas the fifth was detected by digital subtraction angiography on the third postoperative day and treated with angiographic embolization of the GDA stump (Figure 2).
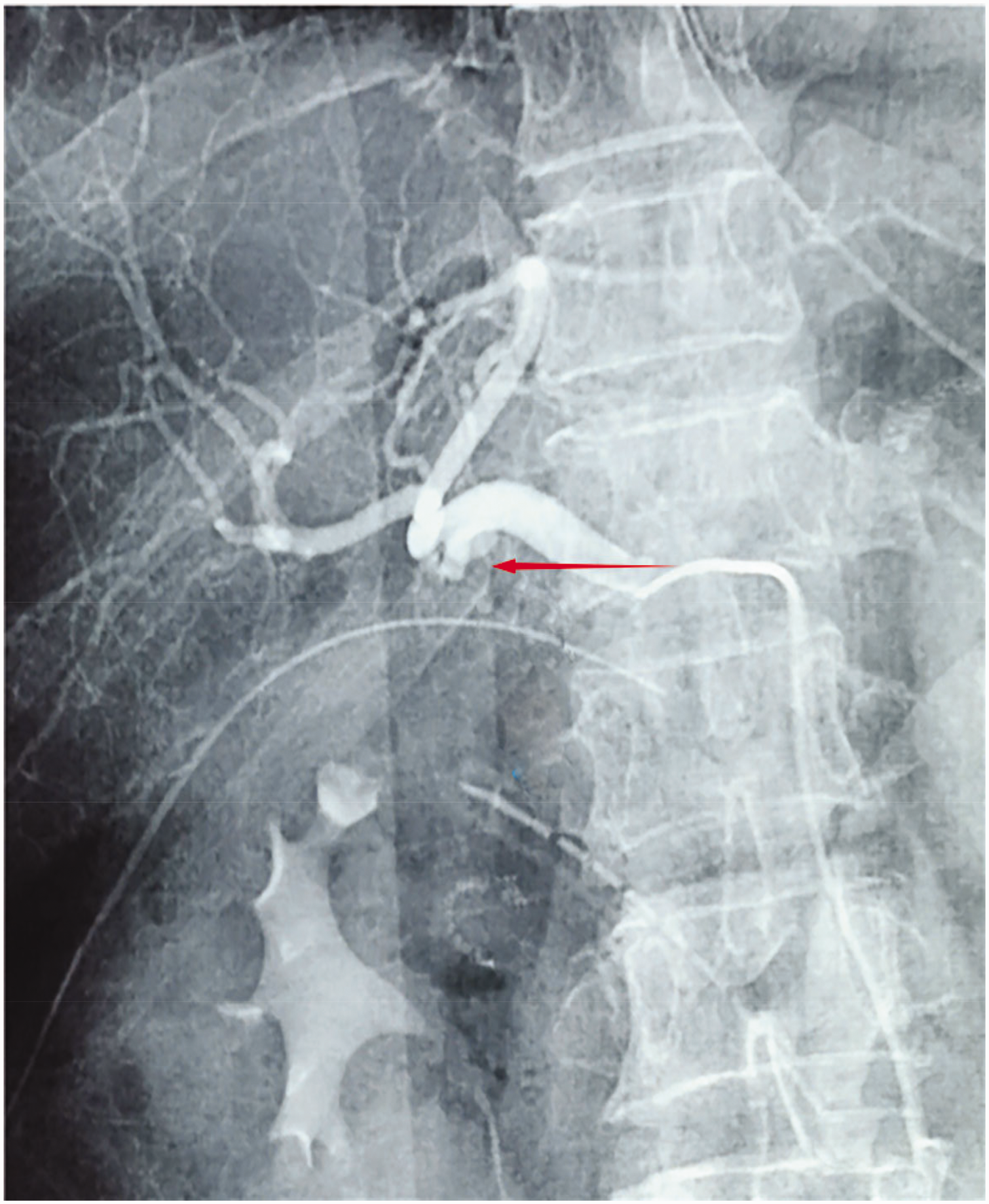
Gastroduodenal artery (GDA) stump hemorrhage (red arrow).
Among the 148 patients who underwent PD in our hospital, 57 developed POPF (overall incidence: 38.5%). There were 21 (POPF incidence: 33.3%) patients with POPF in the unwrapped group and 36 (POPF incidence: 42.4%) with POPF in the wrapped group. Differences in POPF incidence were not statistically significant. Two patients in the unwrapped group died during hospitalization due to bleeding from the pancreaticoenteric anastomosis. In the wrapped group, one patient died of a severe abdominal infection, which developed during postoperative hospitalization (duration: 81 days). There were no significant differences between the groups for bile leakage, arterial stenosis, abdominal infection, DGE, time to first food intake, total hospital stay, or death during hospitalization.
Discussion
GDA stump bleeding after PD is a significant surgical risk.4,6,7 The primary cause of bleeding is vascular erosion caused by POPF.3,8 However, POPF is an inevitable problem with PD, and many research centers worldwide have proposed an improved suture method and performed retrospective analyses; nevertheless, no significant effect has been reported.19,31 Because the pancreatic enterostomy requires suturing the pancreas, the suture pierces the pancreatic duct (which is challenging to avoid) and causes POPF. 19
As POPF cannot be avoided, protecting the GDA stump is critical. Some authors reported covering the main blood vessels with omentum or the falciform ligament to avoid erosion of blood vessels by pancreatic fluid. Sakamoto et al. reported no cases of GDA stump bleeding in 136 patients. 21 Ray et al. reported using the LTH to wrap the GDA stump in 182 patients and found the method equally effective compared with using omentum or the falciform ligament. 20 These findings suggest that wrapping the GDA stump reduces the incidence of intra-abdominal hemorrhage after PD.
In accordance with the ISGPS standard, the incidence of postoperative POPF in our center was 38.5% for all surgeries. This value is higher than that in previous studies, 13 which may be owing to issues caused by the lack of early surgical experience in our institution and may improve with additional cases in the future. Ten cases of pancreaticojejunostomy bleeding or GDA stump bleeding occurred due to clinical POPF (postoperative bleeding rate: 6.8% (10/148) of all surgeries). Nine patients (6.1%) underwent reoperation owing to bleeding, and in 1 patient (0.7%), GDA stump bleeding was identified by digital subtraction angiography. Bleeding was treated successfully by angiography and embolization (Figure 2).
The use of the LTH for GDA stump wrapping has been reported rarely3,4 and remains controversial. We found no GDA stump bleeding in 85 patients who underwent LPD with stump wrapping, suggesting that wrapping the GDA stump with the LTH can reduce the incidence of abdominal bleeding.
We found that 42.4% of the patients had POPF in the wrapped group vs. 33.3% in the unwrapped group. However, there were only two cases of abdominal bleeding in the wrapped group (both had pancreaticoenteric anastomotic bleeding), and no GDA stump hemorrhage was found. In contrast, in the unwrapped group, eight patients had abdominal bleeding, three had pancreaticoenteric anastomosis bleeding, and five had abdominal bleeding due to POPF (Table 3). This finding suggests that GDA stump wrapping reduces the risk of GDA stump bleeding due to erosion associated with POPF. However, there was no significant difference between the wrapped and unwrapped groups regarding pancreaticoenteric anastomotic hemorrhage, POPF, gastric obstruction, time to first passage of flatus, and abdominal infection. Therefore, wrapping the GDA stump did not reduce the incidence of POPF, which causes pancreaticojejunostomy bleeding, DGE, delayed time to first passage of flatus, and abdominal infection. After PD, secondary bleeding usually occurs 2 to 3 weeks after surgery and is accompanied by persistent POPF. In the unwrapped group, two cases of GDA stump bleeding occurred on the third postoperative day, and one occurred on the fourth postoperative day; all were grade B or C POPF. We suspect that bleeding may have occurred because the GDA stump was unprotected; therefore, the GDA stump induced an inflammatory response. Additionally, the drainage tube impacts the GDA stump when the patient is active, leading to bleeding from the stump. Therefore, we can assume that wrapping the GDA stump using the LTH can reduce hemorrhage.
Notably, a retrospective analysis found that using the falciform ligament or omentum to wrap the GDA stump did not reduce the incidence of intra-abdominal bleeding after LPD. 32 We propose the following: (I) The study used multicenter retrospective data, and the standard of operation or the surgeon might have resulted in differences between the previous study and our study. The same surgeon performed all procedures in our study. (II) Because the omentum is thin, PD is likely to damage the omentum, resulting in the infiltration of pancreatic fluid, causing tissue erosion and bleeding. (III) Although the pedicled falciform ligament contains the LTH, which can be used to wrap the GDA stump, the pedicled falciform ligament takes up more space, and pancreatic juice drainage is difficult. These issues may lead to pancreatic juice infiltration, erosion, and bleeding. In contrast, the LTH is thick enough to wrap the GDA stump while leaving sufficient room for drainage of pancreatic juice. Because this was a single-center study with a small sample size, there remains a need for prospective analysis of data from larger samples.
Conclusion
Wrapping the GDA stump with the LTH can reduce bleeding after PD. Owing to our limited clinical data, this finding requires prospective analysis and larger sample sizes. Nevertheless, this technique has the potential to prevent GDA stump hemorrhage after LPD.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231188288 - Supplemental material for Ligamentum teres hepatis wrapping of the gastroduodenal artery stump for protection in total laparoscopic pancreaticoduodenectomy: a single-center experience
Supplemental material, sj-pdf-1-imr-10.1177_03000605231188288 for Ligamentum teres hepatis wrapping of the gastroduodenal artery stump for protection in total laparoscopic pancreaticoduodenectomy: a single-center experience by Zongdong Yu, Xiang Wu, Xinhua Zhou, Xiaodong Hu, Jun Lu, Shenzhe Fang, Luoluo Wang, Yi Ruan, Yeting Lu and Hong Li in Journal of International Medical Research
Footnotes
Acknowledgement
We thank Dr Kevin Li for revising the language in the manuscript.
Author contributions
Zd.Y. and X.W. drafted the manuscript. Xh.Z. and H.L. performed the procedures. J.L. performed the literature review. Xd.H., Sz.F., Ll.W., Y.R., and Yt.L. collected and analyzed the data. All authors read and approved the final manuscript.
Availability of data and materials
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there is no competing interest.
Funding
This work was supported by the Ningbo Digestive System Cancer Clinical Medicine Research Center [2019A21003].
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.