
Abstract
Postpancreatectomy hemorrhage (PPH) is one of the most common complications after pancreatoduodenectomy (PD). It mainly includes gastrointestinal hemorrhage and abdominal hemorrhage. With the development of digestive endoscopy and ultrasonic/radiological interventional technology, hemostasis can be effectively performed by minimally invasive methods in many patients with PPH. This report describes the successful treatment of multiple episodes of postoperative hemorrhage after PD. The patient developed anastomotic hemorrhage after PD and was successfully treated by endoscopic hemostasis. However, he also developed intra-abdominal hemorrhage after PD caused by a pseudoaneurysm that had formed next to the common hepatic artery. We effectively performed hemostasis by injecting lyophilized thrombin powder into the pseudoaneurysm with ultrasound guidance, which is a rarely used method. This case indicates that digestive endoscopy provides great advantages in the treatment of gastrointestinal hemorrhage after PD. For patients who develop PPH with a pseudoaneurysm, interventional ultrasonography is an option if transcatheter arterial embolization or covered stenting fails.
Keywords
Introduction
Pancreatoduodenectomy (PD) is the second most commonly performed procedure after liver transplantation in the field of general surgery. Delayed gastric emptying, pancreatic leakage, biliary leakage, and postpancreatectomy hemorrhage (PPH) are the most common and important complications after PD. PPH occurs in 5% of patients with a 99% confidence interval of 4% to 7%, 1 and it is associated with high mortality. 2 Delayed PPH (>24 hours after PD) is always the result of multiple pathological factors, such as a pancreatic fistula and intra-abdominal abscess. 3 In addition, recent studies have shown that preoperative hyperbilirubinemia is an independent risk factor for PPH after PD 2 and that postoperative hypertension is also a risk factor for PPH after PD. 4
Historically, PPH after PD had always required repeat open surgery. However, with the development of digestive endoscopy and ultrasonic/radiological interventional technology, hemostasis can be effectively performed by minimally invasive methods for many patients with PPH. Endoscopic hemostasis plays an important role in the treatment of anastomotic hemorrhage after PD. 5 Transcatheter arterial embolization or covered stenting is an effective minimally invasive method for the treatment of delayed intra-abdominal hemorrhage after PD. 6 Additionally, ultrasound-guided injection of lyophilized thrombin powder to eliminate a pseudoaneurysm is a new method that has been reported in recent years. It has been successfully used in the treatment of hepatic artery hemangioma formation after surgery 7 and radial artery pseudoaneurysm formation after coronary angiography. 8 However, this method has not been reported in the treatment of abdominal pseudoaneurysm formation after PD.
We herein describe a patient who developed multiple episodes of PPH after PD and was successfully treated by endoscopic hemostasis and ultrasound-guided percutaneous thrombin injection to a common hepatic artery aneurysm.
Case report
History
The reporting of this study conforms to the CARE guidelines. 9 A 73-year-old man with a history of diabetes and hypertension was admitted to our hospital on 29 December 2020 because of a >1-month history of recurrent abdominal pain accompanied by fever. Laboratory tests revealed a total bilirubin concentration of 287 μmol/L, direct bilirubin concentration of 213 μmol/L, alanine aminotransferase concentration of 19 U/L, leukocyte count of 5.1 × 109/L, neutrophilic granulocyte percentage of 65%, and C-reactive protein concentration of 14 mg/L. Therefore, we considered that the patient had developed obstructive jaundice.
Endoscopic examination and treatment
The day after admission, endoscopic ultrasonography revealed a mass in the ampulla (Figure 1). The mass was biopsied, and endoscopic nasobiliary drainage was performed to alleviate the jaundice. Pathologic examination of the biopsy specimen indicated adenocarcinoma on 31 December 2020.

A tumor of the ampulla was found by endoscopic ultrasonography.
Operation
The patient’s jaundice slowly resolved after endoscopic nasobiliary drainage, but his serum total bilirubin was still high at 274 μmol/L before the operation. Radical PD was performed on 12 January 2021. Intraoperatively, a tumor of about 1 cm in size was found in the ampulla. For digestive tract reconstruction, we performed gastrojejunostomy (Braun’ anastomosis), kissing pancreaticojejunostomy (the pancreatic duct was tightly connected to the jejunal mucosa via a tent tube), 10 and end-to-side choledochoduodenostomy (modified Child method). Drainage tubes were placed at the pancreaticojejunostomy site and bilioenteric anastomosis.
Postoperative care
Symptomatic treatments were administered after the operation, including anti-infection measures, hepatic protection, enzyme inhibition, acid inhibition, and parenteral nutrition. The patient developed repeated postoperative hypertension with poor drug control, but his serum total bilirubin slowly decreased after the operation.
Gastrointestinal hemorrhage and management
Twelve days postoperatively, the patient developed hematemesis and melena with no obvious inducement. His blood pressure was 90/55 mmHg, and his heart rate was 84 beats/minute. His hemoglobin concentration decreased from 9 to 5 g/dL. Therefore, we diagnosed upper gastrointestinal hemorrhage and hemorrhagic shock and administered 3.5 units of erythrocyte suspension. Emergency endoscopy was performed immediately, and active hemorrhage was found at the gastrointestinal anastomosis (Figure 2(a)). Hemostasis was performed using an endoscopic endoloop (LeoMed, Changzhou, China) and metal clips (Micro-Tech, Nanjing, China), and a good outcome was attained (Figure 2(b), (c)).

(a) One vessel from the gastrointestinal anastomosis was bleeding. (b, c) Hemostasis was attempted by using an endoscopic endoloop and metal clips.
Intra-abdominal hemorrhage and management
On the sixth day postoperatively, the pancreaticojejunostomy drainage tube was removed because of a low drainage volume and an amylase concentration of <1000 U/L in the drainage fluid (low-flow biochemical leak). However, 14 days after surgery, the patient developed persistent epigastric pain, and abdominal computed tomography (CT) showed moderate amounts of effusion around the left aspect of the liver. After ultrasound-guided puncture and drainage, gray purulent fluid drained from this area. The amylase concentration in the drainage fluid reached 32,000 U/L, and bacterial culture of the drainage fluid revealed numerous Enterococcus faecalis. The patient was considered to have developed an infected postoperative pancreatic fistula (POPF). Therefore, the effusion was adequately drained, and ertapenem injection was added to the anti-infection measures. However, on the 19th day postoperatively, bright red fluid was ejected from the abdominal drainage tube and the patient’s hemoglobin concentration decreased from 9 to 6 g/dL. His blood pressure was 90/50 mmHg, and heart rate was 92 beats/minute.
We diagnosed intra-abdominal hemorrhage and hemorrhagic shock and administered 4 units of erythrocyte suspension. Abdominal CT angiography showed that a pseudoaneurysm had formed next to the common hepatic artery (Figure 3(a)). Thus, we considered that the patient had grade B PPH according to the definition established by the International Study Group of Pancreatic Surgery. 10 Transcatheter celiac arteriography was performed to locate the hemorrhagic site and perform hemostasis. Unfortunately, celiac arteriography showed no contrast medium extravasation (Figure 4). After several days of conservative treatment with hemostatic drugs including hemocoagulase atrox for injection, tranexamic acid, and thrombin, the patient’s condition slightly improved; however, he continued to develop intermittent abdominal hemorrhage. To stop the bleeding, we injected lyophilized thrombin powder into the pseudoaneurysm with ultrasound guidance on 9 February 2021. Contrast-enhanced ultrasound showed that a pseudoaneurysm had formed next to the common hepatic artery. With ultrasound guidance, the puncture needle was inserted into the pseudoaneurysm, and a mixture of 100 U of lyophilized thrombin powder with 5 mL of normal saline was injected. The pseudoaneurysm then significantly shrank on contrast-enhanced ultrasound (Figure 5). The patient’s condition remained stable for the next several days, and no further bloody fluid exited the drainage tube. Abdominal CT angiography conducted 3 days after the treatment showed that the pseudoaneurysm had disappeared (Figure 3(b)).

(a) A pseudoaneurysm next to the common hepatic artery was seen on computed tomography angiography. (b) Repeat computed tomography angiography 3 days after treatment revealed that the pseudoaneurysm had disappeared.
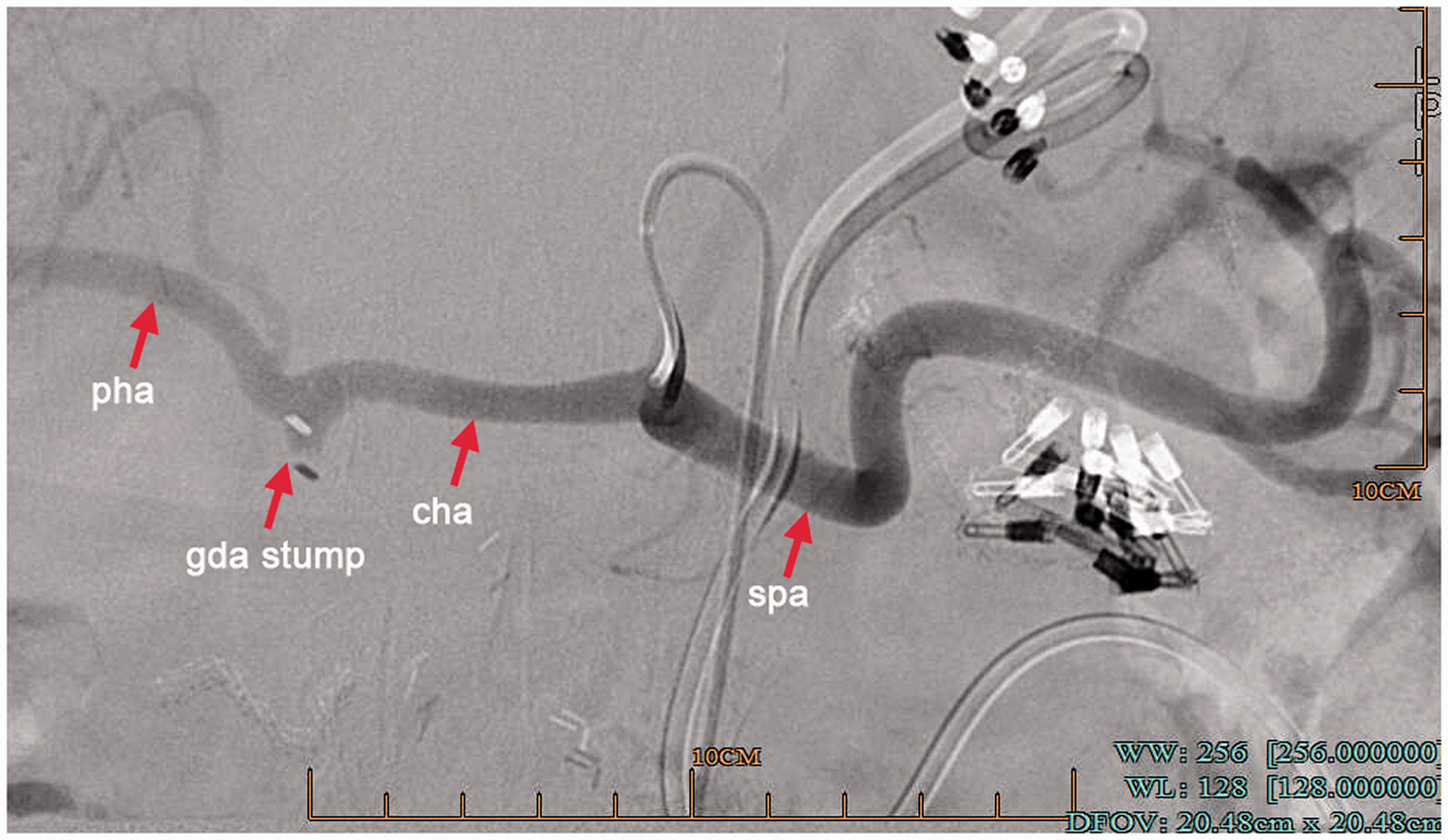
Transcatheter celiac arteriography revealed no leakage of contrast medium.

(a) A pseudoaneurysm next to the common hepatic artery was seen on contrast-enhanced ultrasound. (b) A puncture needle was inserted into the pseudoaneurysm, and lyophilized thrombin powder was injected. (c) The pseudoaneurysm shrank significantly after treatment.
Prognosis
No other complications such as gastrointestinal anastomotic leakage, bile leakage, or gastric retention occurred during the perioperative period. Pathologic examination of the biopsy specimen led to a diagnosis of poorly differentiated adenocarcinoma of ampulla with four positive lymph nodes (T1N2M0 stage IIIB) according to the 8th Edition of the Union for International Cancer Control and the American Joint Committee on Cancer Staging Manual. 11 The patient recovered well and was discharged on 18 February 2021. At discharge, his serum total bilirubin concentration had decreased to 44 μmol/L. The patient returned to the hospital for further consultation on 22 March 2021. Two days later, we administered oxaliplatin plus capecitabine combined chemotherapy. His serum total bilirubin concentration was normal at that time, and he was very satisfied with the therapeutic outcome.
Discussion
Recent studies have shown that preoperative hyperbilirubinemia and hypertension are risk factors for PPH after PD.2,4 Our patient developed upper gastrointestinal hemorrhage after PD because of the following two factors. First, he had severe obstructive jaundice before surgery, and the jaundice slowly improved after surgery. Therefore, liver insufficiency and a disorder of coagulation factor synthesis were considered. For such patients, an appropriate amount of vitamin K1 and thrombin can be administered preoperatively and postoperatively to improve the perioperative coagulation function. Preoperative biliary drainage before PD is controversial. According to a retrospective propensity score-matched analysis by Shen et al., 12 preoperative biliary drainage for severe obstructive jaundice can decrease overall postoperative complications after PD, and it should be performed for patients with a serum total bilirubin concentration of >250 μmol/L. Our patient’s preoperative total bilirubin concentration reached 287 μmol/L. He also had a recurrent fever before surgery, which may have been caused by cholangitis. Therefore, we performed biliary drainage before PD. Second, the patient’s blood pressure increased continuously after surgery, and drug control was poor. Thus, blood pressure fluctuation was another important factor that contributed to the development of hemorrhage in this case. This led us to conclude that perioperative blood pressure control is very important to prevent PPH. For patients with a history of severe hypertension, preoperative consultation with a cardiologist is necessary. Endoscopic hemostasis is always applied in patients with anastomotic hemorrhage after PD. 5 In this case, we successfully treated the postoperative gastrointestinal hemorrhage by endoscopic hemostasis, and repeat open surgery was avoided. Therefore, endoscopic hemostasis provides great advantages in the treatment of gastrointestinal hemorrhage after PD.
Despite hyperbilirubinemia and hypertension, POPF was considered to be an important cause of abdominal hemorrhage in this patient. 3 Therefore, adequate drainage must be performed when POPF occurs after PD. Transcatheter arterial embolization or covered stenting is a preferred and effective method to cure PPH. 6 However, this method was not successful in our case. Ultrasound-guided injection of lyophilized thrombin powder to eliminate the pseudoaneurysm is a new method that has been rarely reported.7,8 There is no relevant report on the treatment of an abdominal pseudoaneurysm after PD using this method. The PPH in this case was successfully treated with the cooperation of the interventional ultrasonography team of our hospital, and repeat open surgery was avoided.
In conclusion, digestive endoscopy provides a great advantage in the treatment of gastrointestinal hemorrhage after PD. For patients who develop PPH with a pseudoaneurysm, interventional ultrasonography is an option if transcatheter arterial embolization or covered stenting fails. To the best of our knowledge, this is the first report of using this technique to treat PPH with a pseudoaneurysm. The outcome was good, suggesting that this technique is safe and effective. In addition, it has the advantages of precision and minimal invasiveness.
Footnotes
Availability of data and materials
Available upon the request of the readers.
Ethics
The publication of this case report was approved by the Scientific Research Department, Affiliated Hangzhou First People’s Hospital, Zhejiang University School of Medicine. The patient herein described provided written informed consent for publication of this case report.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was funded by the National Natural Science Foundation of China (82003248).