
Abstract
Objective
This study was performed to compare the modified direct closure method and traditional skin grafting for wounds at the anterolateral thigh (ALT) flap donor site.
Methods
Among 29 consecutive patients with wounds at the ALT flap donor site, 14 underwent the modified direct closure method (MDC group) and 15 underwent traditional skin grafting (SG group). The operative time, follow-up time, complications, Vancouver Scar Scale (VSS) score, and Scar Cosmesis Assessment and Rating (SCAR) score of the two groups were statistically analyzed.
Results
The mean follow-up times in the MDC and SG group were 16.1 and 16.7 months, respectively. Two patients showed partial skin necrosis after skin grafting, but the remaining patients’ wounds healed uneventfully. The operative time in the MDC group was an average of about 64 minutes shorter than that in the SG group. The average VSS and SCAR scores in the MDC group were 2.1 and 3.0 points lower, respectively, than those in the SG group.
Conclusions
Compared with traditional skin grafting, the modified direct closure method is more efficient for repair of wounds at the ALT flap donor site because of its shorter operative time, better postoperative appearance of the donor site, and higher patient satisfaction.
Keywords
Introduction
The anterolateral thigh (ALT) flap has been widely used to repair soft tissue defects of the limbs in clinical practice. It is known as the “universal skin flap” because of its concealed position, constant vascular pedicle, wide vascular diameter, large area, and minimal limb damage. 1 With the development of society and the economy, patients now have higher requirements for wound repair. In addition to good function, a satisfactory appearance is also very important. Most surgeons, however, pay more attention to the harvesting of the ALT flap and the survival rate of the flap after transplantation 2 and less attention to the treatment of the donor site and related complications.3–5 In fact, if the donor site is not properly treated, many complications are likely to occur.6–8
Skin-related complications in the donor area of the ALT flap are among the main complications that occur after harvesting because of the large scar, skin depression, and poor appearance caused by skin grafting at the donor site. 9 , 10 In our previous work we found that direct tension-free closure is definitely the best choice for wounds at the donor site; however, if the flap is very wide, the donor site cannot be sutured directly. 11 The donor sites of ALT flaps with a width of ≤6 cm can be directly sutured in most cases. 12 However, for ALT flaps with a width of >6 cm, osteofascial compartment syndrome (OCS) can readily occur if the donor site is sutured directly with high tension. Skin grafts are by far the most commonly used repair method for the donor sites of wide ALT flaps, but skin grafting is also associated with complications such as wound dehiscence and skin necrosis, resulting in patient discomfort and dissatisfaction. 13 , 14 Some surgeons have reported the use of steel needles to penetrate the skin and continuously tighten screws to close the wound day by day, hoping to avoid skin grafting and reduce the incidence of complications.15–18 However, because of the serious trauma and long treatment time associated with this technique, it is not widely used in clinical practice. At present, the repair of donor sites of ALT flaps with a width of >6 cm remains challenging. This study was performed to compare a modified direct closure method with traditional skin grafting for repair of the donor site of ALT flaps with a width of >6 cm.
Materials and methods
This study was approved by the institutional review board of our hospital, and each patient provided written informed consent before the study. Patients who underwent ALT flap surgery in our institution from September 2016 to August 2018 were selected. After communicating with and providing an explanation to the patients, the surgical method was selected according to the patients’ wishes and the actual situation during the operation. The patients were divided into two groups according to the repair method used for the donor site: the modified direct closure (MDC) group and skin graft group (SG) group. The inclusion criterion was a ≥6-cm-wide ALT flap. The exclusion criteria were poor cardiopulmonary function, a history of diabetes, and a history of trauma or skin disease in the thigh flap donor area.
In the MDC group, we sutured the donor site with 2-0 Coated Vicryl Plus Antibacterial Suture (Ethicon, Somerville, NJ, USA) to tighten both sides of the wound after the ALT flap was harvested (Figure 1(a)) and transferred to the grafting site. We then pierced the skin along the sewn edge of the skin to create holes with a 5- to 10-mm diameter (Figure 1(b)). We adjusted the number of holes in each row and the number of rows of holes according to the skin tension. After the skin tension was reduced to a satisfactory level, a vacuum-assisted closure device (V.A.C.; Kinetic Concepts, Inc., San Antonio, TX USA) was used to cover the donor site for continuous negative-pressure drainage and was removed in 5 to 7 days. In the SG group, before covering the wound with skin grafts, we designed various local flaps to reduce the area of the wound. Full-thickness skin grafts from other limbs were transferred to the thigh to cover the flap donor site (Figure 1(d)) after the flap was designed (Figure 1(c)) and harvested. We then used the V.A.C. device to provide continuous compaction to the skin graft and removed the V.A.C. device after 5 to 7 days. The skin graft donor area was wrapped with gauze.
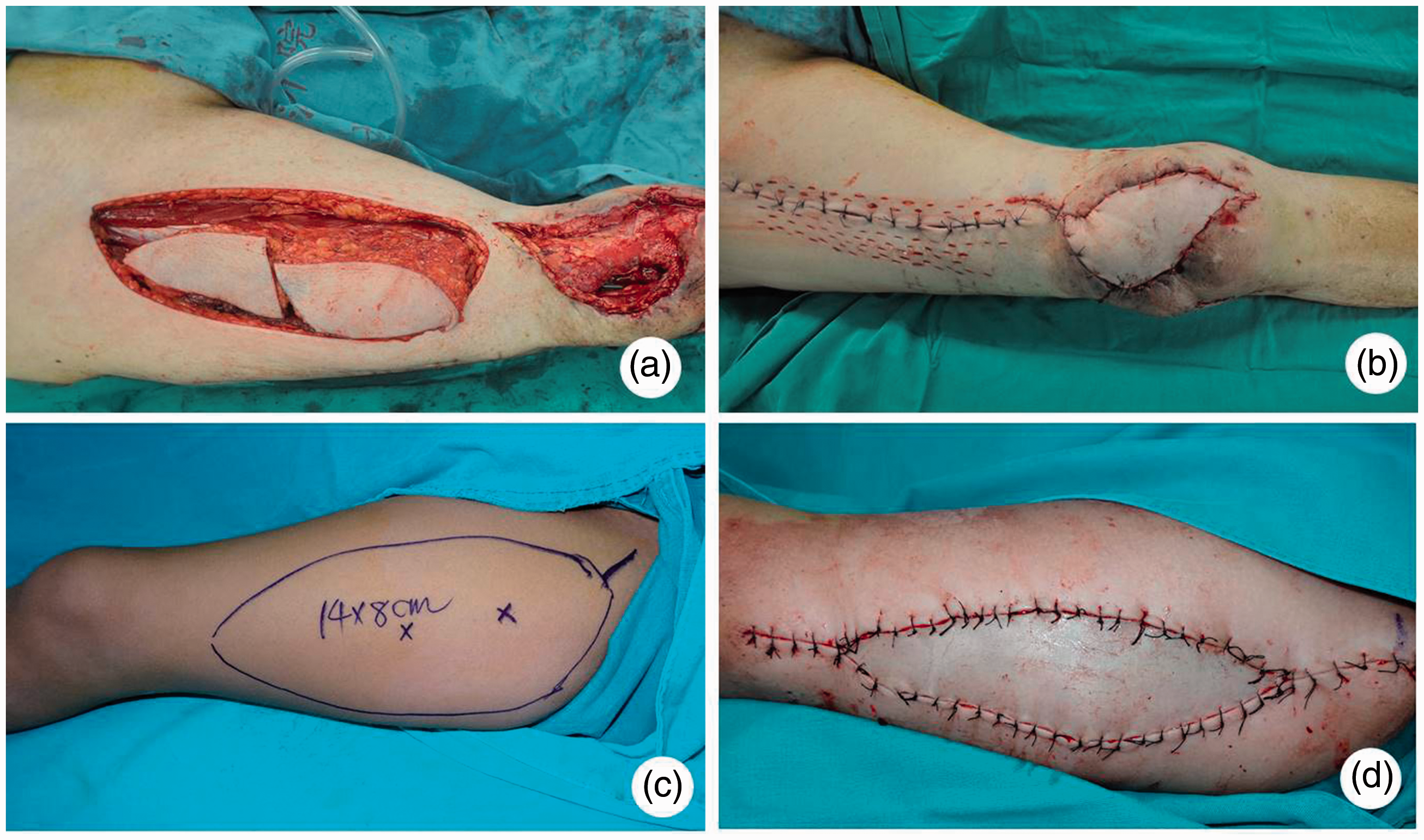
(a) The anterolateral thigh (ALT) flap of Patient 13 was designed and harvested. The size of the flap was 23 × 6 cm2. (b) The skin was pierced along the sewn edge to create holes of 5 to 10 mm in diameter in Patient 13. (c) The ALT flap of Patient 24 was designed and ready to be harvested. (d) A full-thickness skin graft was transferred to the thigh to cover the flap donor site of Patient 24.
We recorded each patient’s age, flap size, donor site coverage method, operative time (from skin incision to end of dressing), and follow-up time. Postoperative complications such as wound dehiscence, skin necrosis, and OCS were also recorded. We evaluated the donor site scar at the last follow-up according to the Vancouver Scar Scale (VSS) score and Scar Cosmesis Assessment and Rating (SCAR) score. 19 During follow-up, both the data recording and scar assessments were performed by the same group of surgeons. The mean and standard deviation of the VSS and SCAR scores were calculated, and one-way analysis of variance was performed. A p value of <0.05 was defined as statistically significant, and SPSS 21.0 software (IBM Corp., Armonk, NY, USA) was used for statistical analysis.
Results
Twenty-nine patients were included in this study. The MDC group comprised 14 patients (12 men and 2 women; average age, 47.8 years; wound area, 18.0 × 6.0 to 27.0 × 10.0 cm2). The SG group comprised 15 patients (12 men and 3 women; average age, 44.9 years; wound area, 14.0 × 8.0 to 20.0 × 11.5 cm2). The average flap dimension in the MDC group was 20.1 × 7.7 cm2, and that in the SG group was 20.2 × 9.4 cm2. The patients’ demographic information is shown in Tables 1 and 2.
Patients’ demographic data in the MDC group.
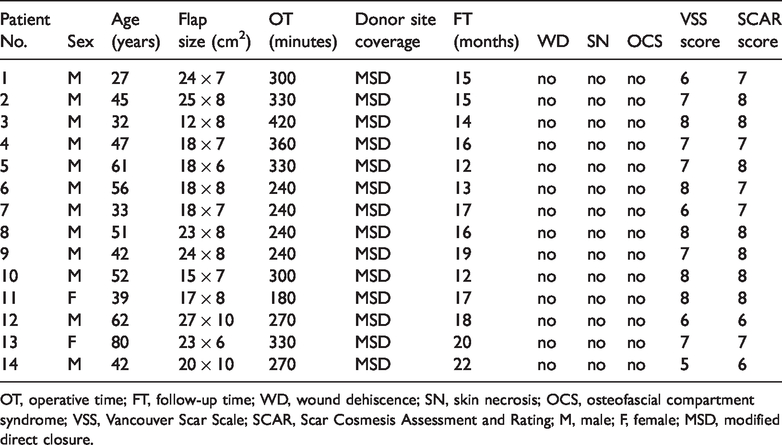
OT, operative time; FT, follow-up time; WD, wound dehiscence; SN, skin necrosis; OCS, osteofascial compartment syndrome; VSS, Vancouver Scar Scale; SCAR, Scar Cosmesis Assessment and Rating; M, male; F, female; MSD, modified direct closure.
Patients’ demographic data in SG group.

OT, operative time; FT, follow-up time; WD, wound dehiscence; SN, skin necrosis; OCS, osteofascial compartment syndrome; VSS, Vancouver Scar Scale; SCAR, Scar Cosmesis Assessment and Rating; M, male; F, female; SG, skin grafting.
The follow-up time was not significantly different between the two groups. The operative time in the MDC group was about 64 minutes shorter than that in the SG group with a significant difference (p < 0.05). Harvesting of the skin graft and treatment of the skin graft donor area took an average of about 1 hour. The operative times for Patient 3 in the MDC group and Patients 16, 21, and 27 in the SG group were >400 minutes, which might have been related to the difficult harvest of the ALT flap caused by anatomical variation during the operation. In Patients 16 and 25 of the SG group (Figure 2(a)), partial skin graft necrosis occurred (Figure 2(b)) and the donor sites healed after nearly 1 month of dressing changes. This might have been related to failure of the V.A.C. device to provide reliable and continuous compression because of the depression of the wound surface. None of the remaining 27 patients developed wound dehiscence, skin necrosis, or OCS. After the donor site repair, each patient developed some degree of scarring, but the severity in the MDC group was significantly less than that in the SG group (p < 0.05) (Table 3). The VSS and SCAR scores were 2.1 and 3.0 points lower, respectively, in the MDC group than in the SG group, and the difference was statistically significant (p < 0.05). In contrast to the VSS score, the SCAR score includes patients’ subjective evaluation of itching and pain, which might explain the large gap in the SCAR scores between the two groups in our study. This result also indicates that itching and pain at the donor site were more serious after skin graft repair than after modified direct closure.

(a) The anterolateral thigh (ALT) flap of Patient 25 was designed and ready to be harvested. (b) Partial skin necrosis occurred 3 months after skin grafting in Patient 25. (c) The ALT flap of Patient 14 was designed and ready to be harvested. (d) The appearance of the ALT flap donor site of Patient 14 at 3 months after repair by the modified direct closure method.
Comparison of operation time, follow-up time, complications, VSS score, and SCAR score in the two groups.
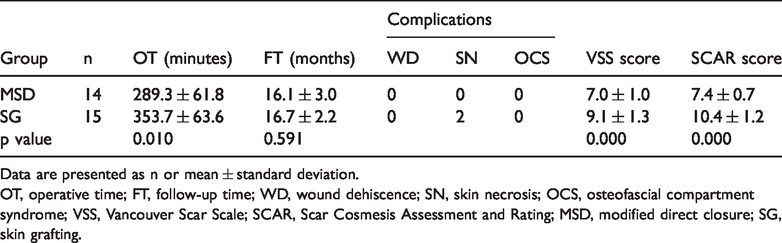
Data are presented as n or mean ± standard deviation.
OT, operative time; FT, follow-up time; WD, wound dehiscence; SN, skin necrosis; OCS, osteofascial compartment syndrome; VSS, Vancouver Scar Scale; SCAR, Scar Cosmesis Assessment and Rating; MSD, modified direct closure; SG, skin grafting.
Discussion
ALT flaps have been popular since they were first introduced by Song et al. 20 in 1984. These flaps are now considered the mainstay of tissue reconstruction because of their advantages of a wide application range, reliability, and stability. However, complications at the ALT flap donor site remain a difficult problem to solve. Complications at the donor site, such as extensive scarring, wound dehiscence, skin necrosis, or even OCS, are being given increasingly more attention by surgeons today. 21 , 22 The occurrence of these complications is related to excessive tension at the donor site, which is too wide for direct suturing. According to multiple clinical retrospective reports,23–25 the width of most ALT flaps is >6 cm. For the ALT flaps of <6 cm in width, the donor site can be safely and directly sutured with few complications. Therefore, donor site repair is very challenging for ALT flaps with a width of ≥6 cm, and research in this field is of great clinical value. Zhou et al. 26 used a modified anteromedial thigh perforator flap to repair 16 ALT free flap donor sites, but this method was associated with a risk of additional damage to the normal limbs and an increased range of iatrogenic injury. Based on the concept that the coverage area can be increased by piercing the skin and creating multiple holes to decrease tension, we designed this modified method combined with our previous work on ALT flaps. In this study, a modified direct closure method was used to repair the wound at the ALT flap donor site, and the efficacy was compared with that of traditional skin grafting.
After the flap was harvested, we sutured the wound at the donor site to tighten the skin. In real practice, we have noticed that it is easier to use a sharp knife to pierce tight skin. When creating the holes, we tried to keep the diameter of each hole within 5 to 10 mm because when suturing wounds on the thigh, most surgeons keep the distance between two stitches within 5 to 10 mm. Creating holes that are too small would affect the extension of the area and the efficiency of drainage. However, in the actual surgical operation, we had to make corresponding adjustments according to each patient’s situation. It was easier to pierce the medial than lateral skin with the patients in the supine position. The middle part of the wound had the highest tension; therefore, the number of rows of holes was increased in this area, and creation of holes on both ends was sometimes unnecessary because of little tension. If we were unsure of the intensity of skin tension during the operation, more holes were made to ensure safety. If the skin tension was not that high, there was no need to deliberately make holes because the holes will heal with scarring. We should also avoid too many holes in the medial sensitive part of the thigh because scarring may cause a significant increase in discomfort. After the holes were made, the V.A.C. device was applied in the donor area to maintain continuous negative pressure, which was set to 125 mmHg. The largest width of the ALT flaps in the MDC group was 10 cm (Patients 12 and 14) (Figure 2(c)). During our follow-up, these two patients were satisfied with the appearance of the donor sites (Figure 2(d)). Our current study shows that this method is more suitable for repair of ALT flap donor sites with a width of >6 cm but <10 cm. The efficacy and safety of this method for donor sites with a width of >10 cm need to be further studied.
In summary, we have herein evaluated a modified direct closure method for wounds at the ALT flap donor site. This method has the following advantages. First, compared with traditional skin grafting, this method can avoid a wide range of scars, pigmentation, and additional trauma to the normal tissues of other limbs. The retention of subcutaneous tissue avoids depression of the donor site, substantially shortens the operative time, and improves patient satisfaction scores. Second, multiple holes can not only reduce the skin tension but also improve the drainage from subcutaneous tissues and muscles in the donor area, avoid edema, and reduce the incidence of infection and OCS. Third, this method is adjustable: according to the individual patient’s situation (e.g., limb length, limb circumference, fat thickness, flap width, skin tension after closure), the appropriate range of holes is selected to achieve personalized treatment and precision medicine. However, this method also has its weaknesses. For example, the appearance of the skin will inevitably heal with scars after the skin is pierced, and the use of the V.A.C. device will also increase medical expenses. Notably, this method is not applicable to wide wounds at the donor area. Because the number of holes and rows are dependent upon the different physical condition of each patient, surgeons must have high technical skill and experience.
This study has two main limitations. First, the number of patients was relatively small, and the flap dimensions between the two groups were unequal. Although the results are encouraging, more cases must be evaluated to confirm the curative effect and resolve the problem of inequality of the flap dimensions. Second, the proper distance between the holes and rows requires more in-depth research. Considering this, we aim to continue this work in future.