
Abstract
The complex reconstruction of nerves and soft tissue in the head and neck region is still challenging, especially in cases requiring external auditory canal reconstruction with facial nerve reconstruction. We report a case of left facial schwannoma extending into the external auditory canal beyond the tympanic membrane with facial paralysis in which the reconstruction of both the facial nerve and external auditory canal was successfully performed using an anterolateral thigh flap as a super-thin full-thickness skin flap, including vascularized lateral femoral cutaneous nerve. Resection of 20 mm × 46 mm facial schwannoma, including the skin of the external auditory canal, tympanic membrane, incus and malleus, was performed. The 8-cm nerve gap was repaired using a vascularized lateral femoral cutaneous nerve included in the anterolateral thigh flap. An 8 cm × 2 cm super-thin, free anterolateral thigh flap was then rolled up as a sac (diameter of 2 cm, height of 2 cm) and inset to the external auditory canal defect. The postoperative course was uneventful, and the flap survived completely. One year and nine months after the surgery, the patient’s facial movement has improved to the pre-surgery level.
Keywords
Introduction
Facial nerve schwannomas presenting facial paralysis (FP) and hearing loss because of the tumor invasion into the external auditory canal (EAC) are rare situation. Especially in cases requiring EAC reconstruction, the complex reconstruction of the facial nerve and soft tissue after tumor resection is challenging. We report a case in which the reconstruction of both the facial nerve and EAC was successfully performed using an anterolateral thigh (ALT) flap as a full-thickness skin flap 1 including vascularized lateral femoral cutaneous nerve (LFCN).
Case
A 37-year-old woman with a left facial nerve schwannoma exhibited left FP and hearing loss. Twelve years prior, she noticed left FP. Two years prior, temporalis muscle transfer and fascia lata transfer were performed for progressing FP at another hospital. Two years after the surgery, she noticed hearing loss, and further examinations were performed. Progression of the FP up to Yanagihara grading system 16/40 with synkinesis and contracture was observed, and pure-tone audiometry showed an average 37-dB conductive hearing loss. Computed tomography (CT) and magnetic resonance imaging (MRI) revealed a well-circumscribed mass lesion in the left EAC, tympanic cavity and mastoid air cells with the invasion into the parotid gland (Figure 1). The tumor size was 20 mm × 46 mm. Therefore, tumor resection and reconstruction of the resected facial nerve and EAC were planned. Resection of schwannoma, including the skin of the EAC, tympanic membrane, incus and malleus, was performed. The facial nerve was also resected with an 8-cm nerve gap; the proximal edge was at the horizontal part, and the distal was edge at the posterior margin of the parotid gland. After resection and tympanoplasty, the vascularized LFCN with an 8 cm × 2 cm, super-thin, free ALT full-thickness skin flap was elevated from the left thigh region (Figure 2(a) and (c)). The flap was then rolled up as a sac (diameter of 2 cm, height of 2 cm) and inset to the EAC defect (Figure 2(b)). The ALT artery and vein were anastomosed end to end with the facial artery and the branch of the retromandibular vein. The neurorrhaphy of the LFCN and the facial nerve was performed in order to fill the nerve gap.
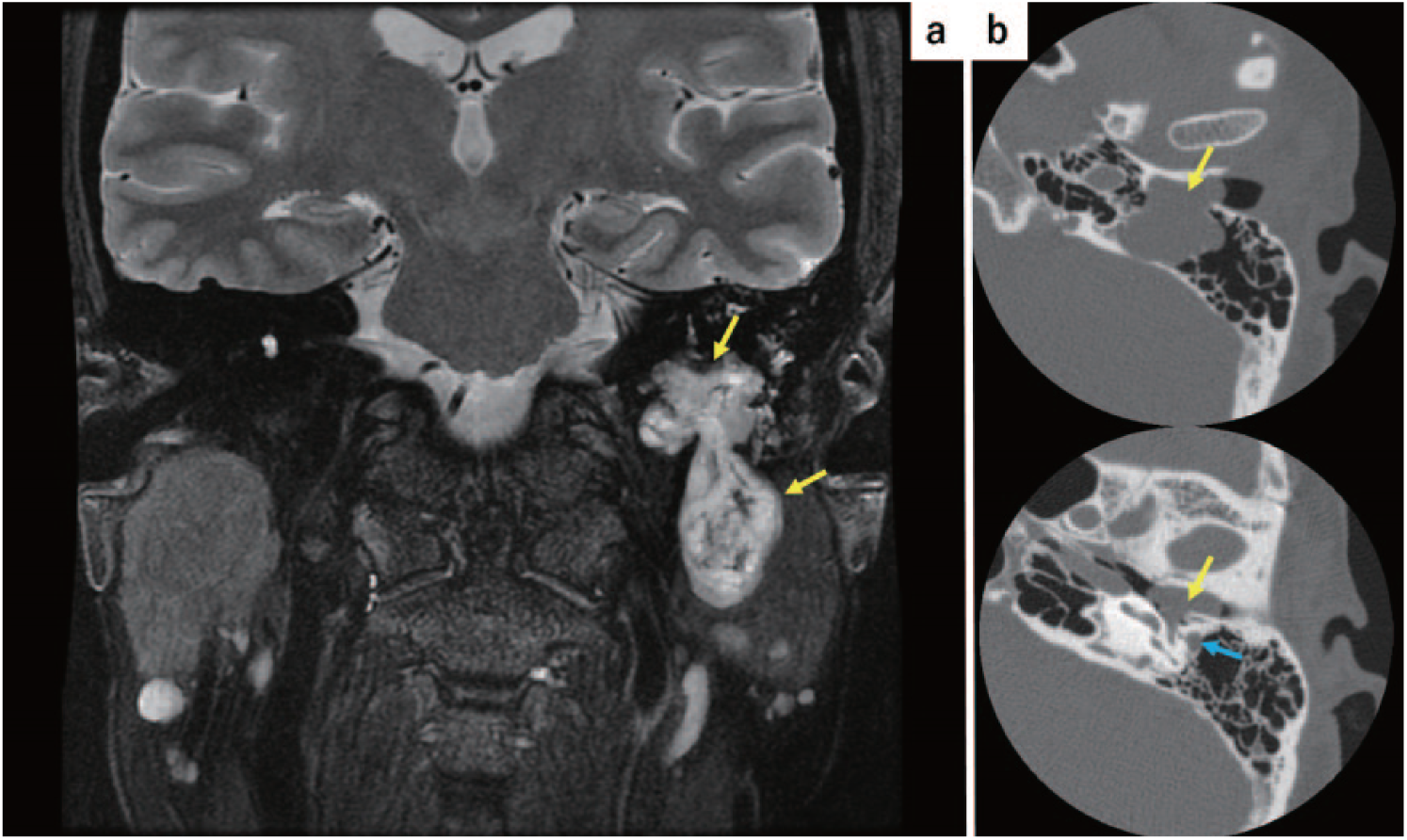
(a) Magnetic resonance imaging showing a 20 mm × 46 mm well-circumscribed mass lesion (yellow arrow) and (b) computed tomography showing well-circumscribed mass lesion in the left external auditory canal, tympanic cavity and mastoid air cells (yellow arrow), blue arrow shows facial nerve.

(a) A super-thin, free anterolateral thigh pure skin perforator flap was elevated from the left thigh region. (b) The flap was rolled up as a sac: yellow arrow: nerve, red arrow: pedicle, blue arrow: skin flap and (c) intraoperative appearance after the resection of left facial nerve schwannoma.
Slight ear discharge was seen after the operation, but it improved immediately. The postoperative course was uneventful, and the flap survived completely (Figure 3). Good patency of the reconstructed EAC was accomplished without revisional debulking surgery. Postoperative conductive hearing loss was the same degree as preoperative, despite extensive tumor resection including the tympanic membrane, ossicles and EAC.

Otoscope showing completely survived anterolateral thigh (ALT) flap at the osseous potion of auditory canal: blue arrow: tympanum, green arrow: ALT flap.
Postoperatively, the facial nerve has gradually recovered through the vascularized nerve flap. One year and nine months after the surgery, her facial movement improved to the same extent as preoperative: Yanagihara grading system 18/40. Synkinesis and contracture were also improved (Figure 4).

The facial appearance 21 months after the surgery.
Discussion
Some experimental studies have described the superiority of nerve regeneration with a vascularized nerve flap over that with a non-vascularized conventional nerve graft.2,3 Experiments using rats by Koshima and Harii 2 revealed the increased density and diameter of regenerating axons and accelerated axonal sprouting of vascularized nerve flaps in poor vascular beds. Experiments using rabbits by Yun et al. 3 have demonstrated that the vascularized nerve flap is superior for facial nerve repair. Doi et al. 4 compared the outcomes of vascularized and conventional sural nerve grafts in the reconstruction of the extremities and suggested that the vascularized nerve flap should be used for nerve reconstruction when the nerve gap is more than 6 cm. Therefore, we used a vascularized LFCN for reconstruction of the facial nerve in order to fill an 8-cm nerve gap.
Combined nerve and soft tissue reconstruction using a free ALT flap with the LFCN has been reported.5 –7 Yamamoto et al. 5 reported a case using a free ALT flap with vascularized LFCN for treatment of recurrent carpal tunnel syndrome with severe pain due to large neuroma. Villarreal et al. 7 reported a case using an extended free ALT flap with vascularized LFCN for the reconstruction of complex neck, head and facial nerve defects following total parotidectomy. In this case, a super-thin flap was essential for the reconstruction of the EAC in order to prevent major complications such as lateralization of tympanum, stenosis and chronic ulcer. Narushima et al. 1 reported a case using a superficial circumflex iliac artery perforator pure skin perforator (SCIP-PSP) flap for microtia and congenital aural atresia and demonstrated that the perforator penetrating the dermis alone could nourish the skin flap without subdermal tissues. Therefore, we combined the two concepts for this case.
We experienced a case that underwent the reconstruction of both the facial nerve and EAC using a super-thin ALT flap with a vascularized LFCN after resection of schwannoma. Postoperative conductive hearing loss was the same degree as preoperative, though it was expected that extensive tumor resection including the tympanic membrane, two ossicles and the proximal part of EAC would exacerbate hearing loss. Good patency of reconstructed EAC using a super-thin skin flap might make it possible to keep auditory capacity. A super-thin full-thickness skin flap may still be more useful for cases with well preserved ossicles.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from the University of Tokyo Hospital ethics committee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI Grant Number JP17H06578.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article. The patient consent included consent for publishing patient images.