
Abstract
Objective
To determine whether musculoskeletal ultrasound (MSUS) abnormalities were associated with thyroid dysfunction.
Methods
This study included 109 patients with thyroid diseases, including thyroid dysfunction or autoimmune thyroid disease. Patients were categorized as euthyroid, hypothyroid, or hyperthyroid based on their recent thyroid function tests. To evaluate MSUS, an experienced rheumatologist examined the presence of synovial fluid, synovial hypertrophy, and grade of inflammation in both gray-scale and power Doppler scans of the knee joint. Associations between MSUS abnormalities, thyroid status, visual analog scale (VAS) score for knee pain, and presence of thyroid autoantibodies were investigated.
Results
MSUS abnormalities were more frequently associated with hyperthyroid or hypothyroid states than with a euthyroid state. High knee VAS score was significantly associated with overall MSUS severity score regardless of knee osteoarthritis. However, there was no difference in MSUS abnormalities based on the presence of thyroid autoantibodies.
Conclusions
Both hypothyroid and hyperthyroid states were associated with MSUS abnormalities and knee arthralgia. MSUS examination may be helpful in uncontrolled thyroid dysfunction and knee arthralgia.
Keywords
Introduction
Hypothyroidism and hyperthyroidism are found in 4.6% and 5.6% and 0.6% and 1.3% of the general population, respectively.1,2 It has been reported that the prevalence of hypothyroidism and hyperthyroidism in Korea is 3.8% and 3.5%, respectively. 3 Thyroid dysfunction and the presence of thyroid autoantibodies are more frequently found in patients with rheumatic disease, such as Sjogren’s syndrome, rheumatoid arthritis, systemic lupus erythematosus, and scleroderma.4,5 One study demonstrated that patients with autoimmune thyroid disease (AITD) are at significantly increased risk of additional autoimmune conditions. 6 These results firmly suggest an association between thyroid dysfunction and other forms of inflammatory states. There have also been studies showing the association of thyroid disease with rheumatoid arthritis (RA). The presence of thyroid diseases in RA patients may affect arthritis progression and lead to a poorer treatment response. 7 Another study showed that joint destruction was amplified in RA patients who had thyroid autoantibodies. 8 Thyroid dysfunction often causes musculoskeletal signs and symptoms. Hypothyroidism is associated with an increased incidence of arthritis, including carpal tunnel syndrome, calcium pyrophosphate deposition disease (CPPD) arthritis, and shoulder capsulitis.9–11 Decline in bone mineral density due to altered bone metabolism and proximal muscle weakness is also a common and serious manifestation of hyperthyroidism.10,11
Musculoskeletal ultrasound (MSUS) is a commonly used modality in the detection of even minimal synovitis, and has advantages including non-invasiveness and lack of ionizing radiation hazards. According to numerous studies, MSUS has higher sensitivity, specificity, and accuracy for detecting inflammation and synovial fluid compared with a normal physical examination.12,13 One study showed subclinical synovitis using MSUS in persons without joint pain; MSUS detected synovitis even in 13% of asymptomatic joints. 13 Among the joints affected by thyroid dysfunction, such as hypothyroidism, the knee joints can be easily examined clinically, and can be evaluated as objective joints if the knee osteoarthritis (OA) is controlled.14–16
Here, we evaluated the association between knee MSUS abnormalities and thyroid status in patients with thyroid dysfunction. The purpose of our study was to determine whether differences in MSUS abnormalities were observed according to the state of thyroid function.
Materials and methods
Study design and subjects
The study was approved by the Institutional Review Board of Soonchunhyang University Seoul Hospital (2015-06-006), and written informed consent was obtained from all participants.
Patients who were diagnosed with thyroid diseases, including thyroid dysfunction or AITD, were enrolled consecutively between June 2015 and July 2016. All patients underwent MSUS of both knee joints and a visual analog scale (VAS) score evaluation for knee pain. Subjects were excluded if they had chronic diseases such as diabetes mellitus, alcoholism, liver or kidney disease, connective tissue disease, and other severe illnesses, or were taking medications that caused musculoskeletal symptoms. Subjects taking medications such as analgesics that can mask musculoskeletal pain were excluded. Subjects who underwent knee arthroplasty with a prosthesis were also excluded.
Musculoskeletal ultrasound
A LOGIQ (General Electric, Chicago, IL, USA) ultrasound machine with a linear-array 12 MHz linear transducer was used to evaluate the knee joints. Three areas of the suprapatellar recess, medial compartment, and lateral compartment of the knee were assessed. Patients were assessed with the knee partially flexed to 30°, and each compartment was scanned in the longitudinal and transverse planes. The suprapatellar recess was defined as the area above the patella, the medial compartment as the area medial to the patella running inferiorly past the medial joint line to the inferomedial aspect of the joint capsule, and the lateral compartment as the area lateral to the patella running inferiorly past the lateral joint line to the inferolateral aspect of the joint capsule.9,17 MSUS was performed by an experienced rheumatologist who had undergone appropriate training programs in the Korean College of Rheumatology. The clinician performed MSUS without knowing the clinical thyroid status of the patients.
In a study of healthy Korean adults, the mean suprapatellar recess thickness was 0.9 ± 0.9 mm. 17 Both knee joints were scanned for the presence of synovial hypertrophy, joint effusion in gray-scale (GS), and presence of the power Doppler (PD) signal. In GS, synovial hypertrophy was defined as an abnormally hypoechoic joint space, which was not compressible with the transducer. Joint effusion was defined as the presence of an abnormally anechoic joint space, which was compressible with the transducer. In the PD scale, PD signal was considered positive in the presence of vessel dots on the PD image. For assessing GS, a normal knee or grade 0 involves a ‘slit’ of fluid, synovium without elevation of the pre-patellar fat pad, and minimal extension beyond the prepatellar fat pad. A mild or grade 1 knee shows a minimal joint effusion, synovial hypertrophy with elevation of the prepatellar fat pad, and extension <50% of the visualized portion of the quadriceps tendon. A moderate or grade 2 knee shows a moderate joint effusion, synovial hypertrophy with elevation of the prepatellar fat pad, and extension >50% of the visualized portion of the quadriceps tendon. A severe or grade 3 knee shows significant distension of the suprapatellar recess between the undersurface of the quadriceps tendon and the pre-femoral fat pad, extension throughout the image, and the most proximal portion of the synovial recess is at >50% of the maximum distension of the recess. 18 For assessing PD scale, a normal PD or grade 0 knee includes the presence of no signal. Grade 1 includes one to three signals, or up to one confluent spot and two single spots, or up to two confluent spots within the area of synovial hypertrophy. Grade 2 includes more than three signals or confluent signals present in <50% of the area of synovial hypertrophy. Grade 3 includes confluent signals present in >50% of the area of synovial hypertrophy.18,19 Synovitis was graded according to the European League Against Rheumatism (EULAR)-Outcome measurement in Rheumatology clinical trials (OMERACT) combined scoring system. 19 A joint with MSUS abnormalities was defined as a joint in which synovial hypertrophy, joint effusion, or PD signal were at least grade 1. If the grade of a patient’s two knee joints was different, the patient’s MSUS abnormalities were defined as the higher grade. For example, in one patient the synovial hypertrophy of the left knee was grade 1 and the synovial hypertrophy of the right knee was grade 2, so the synovial hypertrophy of the patient’s knees was defined as grade 2. The overall MSUS severity scores (calculated as the sum of the severity ratings obtained in each joint, each ranging from 0 to 9) for synovial hypertrophy, joint effusion, and PD signal (each ranging from 0 to 3) were calculated for each patient. 20
Thyroid dysfunction status
All patients had undergone thyroid function tests, including those for thyroid stimulating hormone (TSH), free T3 (fT3), and free T4 (fT4), within the preceding 12 weeks. Thyroid dysfunction was categorized according to the most recent thyroid hormone levels. Hypothyroidism was defined as elevated TSH levels with low fT3 and/or fT4 levels. Subclinical hypothyroidism was also categorized as hypothyroidism. Subclinical hypothyroidism was defined as elevated TSH levels with normal thyroid hormone levels. Euthyroidism was defined as normal fT3, fT4, and TSH levels. Hyperthyroidism was defined as suppressed TSH levels with high fT3 and/or fT4 levels. Subclinical hyperthyroidism was also categorized as hyperthyroidism. Subclinical hyperthyroidism was defined as suppressed TSH levels with normal thyroid hormone levels. The reference ranges for thyroid function tests are as follows: TSH, 0.4–5.0 mIU/L; fT3, 2.0–4.25 pg/mL; f T4, 0.8–1.9 ng/dL.
AITD is defined as a group of immunological disorders of the thyroid gland that include Graves’ disease and chronic lymphocytic thyroiditis (CLT) (also known as Hashimoto’s thyroiditis (HT)). The diagnosis of Graves’ disease was based on thyrotoxicosis with clinical features of hyperthyroidism, demonstration of circulating thyroid antibodies against thyrotropin receptor, and radionuclide scanning. The diagnosis of CLT/HT was based on demonstration of circulating antibodies to thyroid antigens (thyroperoxidase and thyroglobulin), reduced echogenicity of thyroid ultrasound and proper clinical features.21–23
Radiographic and clinical assessment of knee pain
The status of radiographic knee OA was assessed using the Kellgren–Lawrence (K-L) scale. 24 We defined radiographic knee OA among patients who had knee x-rays with a K-L grade higher than 1. All patients were asked to rate the intensity of their knee pain on a 10-cm VAS (0 = no pain and 10 = maximum pain).
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD) or median (range). The prevalence data were compared using the chi-square test or Fisher’s exact test. Partial correlations between knee VAS score and overall MSUS severity score were assessed using Pearson’s correlation analysis. Simple and multiple linear regression were performed to identify factors affecting overall MSUS severity score. All statistical analyses were performed using SPSS version 21.0 (IBM Corp, Armonk, NY, USA). P values of <0.05 were considered statistically significant.
Results
In total, 109 patients were enrolled. The mean patient age was 58.2 ± 13 years, 96 (88.1%) were female, and the mean duration of thyroid disease was 4 years. In fourteen patients (12.8%), this was their first visit, and 100 patients (91.7%) were taking medication for thyroid disease. When patients were classified according to their most recent thyroid function test, 61 (56%) had euthyroid status, 11 (10.1%) had hypothyroidism, and 37 (33.9%) had hyperthyroidism. In addition, 68 (62.4%) patients tested positive for thyroid autoantibody were diagnosed with AITD (Table 1).
Baseline characteristics of the patients.

n, number; SD, standard deviation; VAS, visual analog scale; OA, osteoarthritis; K-L grade, Kellgren–Lawrence grade.
The mean MSUS abnormality scores of knee joints of all patients were as follows; synovial hypertrophy grade 1.5 ± 0.7, joint effusion grade 1.1 ± 0.3, and PD grade 0. The mean overall MSUS severity score of the joints in all patients was 1.2 ± 0.6 (Table 2). When thyroid function was classified into two groups as euthyroid or thyroid dysfunction, including hypothyroidism or hyperthyroidism, the frequency of abnormal findings on MSUS of knee joints was significantly higher in the thyroid dysfunction group (p < 0.001). Among the abnormal findings on MSUS of knee joints, there was a significant difference between the two groups in the rate of joint effusion (p < 0.001). The thyroid dysfunction group also had a significantly higher overall MSUS severity score (p < 0.001) (Table 3). Statistically significant differences in MSUS abnormalities were also noted for hypothyroid vs euthyroid state (p = 0.003), and hyperthyroid vs euthyroid state (p < 0.001), but not for hypothyroid vs hyperthyroid state (Figure 1). Simple and multiple linear regression were performed to identify factors affecting overall MSUS severity score. High knee VAS score was significantly associated with overall MSUS severity score regardless of knee OA status. However, age, sex, and body mass index (BMI) were not associated with overall MSUS severity score (Table 4). There was also no correlation between the presence of thyroid antibodies and MSUS abnormalities.
Summary of abnormal MSUS findings in patients with thyroid disease.

MSUS, musculoskeletal ultrasound; SD, standard deviation; Overall MSUS severity score was calculated as the sum of the severity rating, each ranging from 0 to 9 for synovial hypertrophy, joint effusion, and power Doppler signal (each ranging from 0 to 3).
Differences in MSUS findings between euthyroid and thyroid dysfunction groups.

**p < 0.005, Statistical analysis was performed using chi-square test, Fisher’s exact test, and Mann–Whitney test.
MSUS, musculoskeletal ultrasound; NA, not available; Overall MSUS severity score (ranging from 0 to 9) calculated as the sum of severity ratings for synovial hypertrophy, joint effusion, and power Doppler signal (each ranging from 0 to 3).
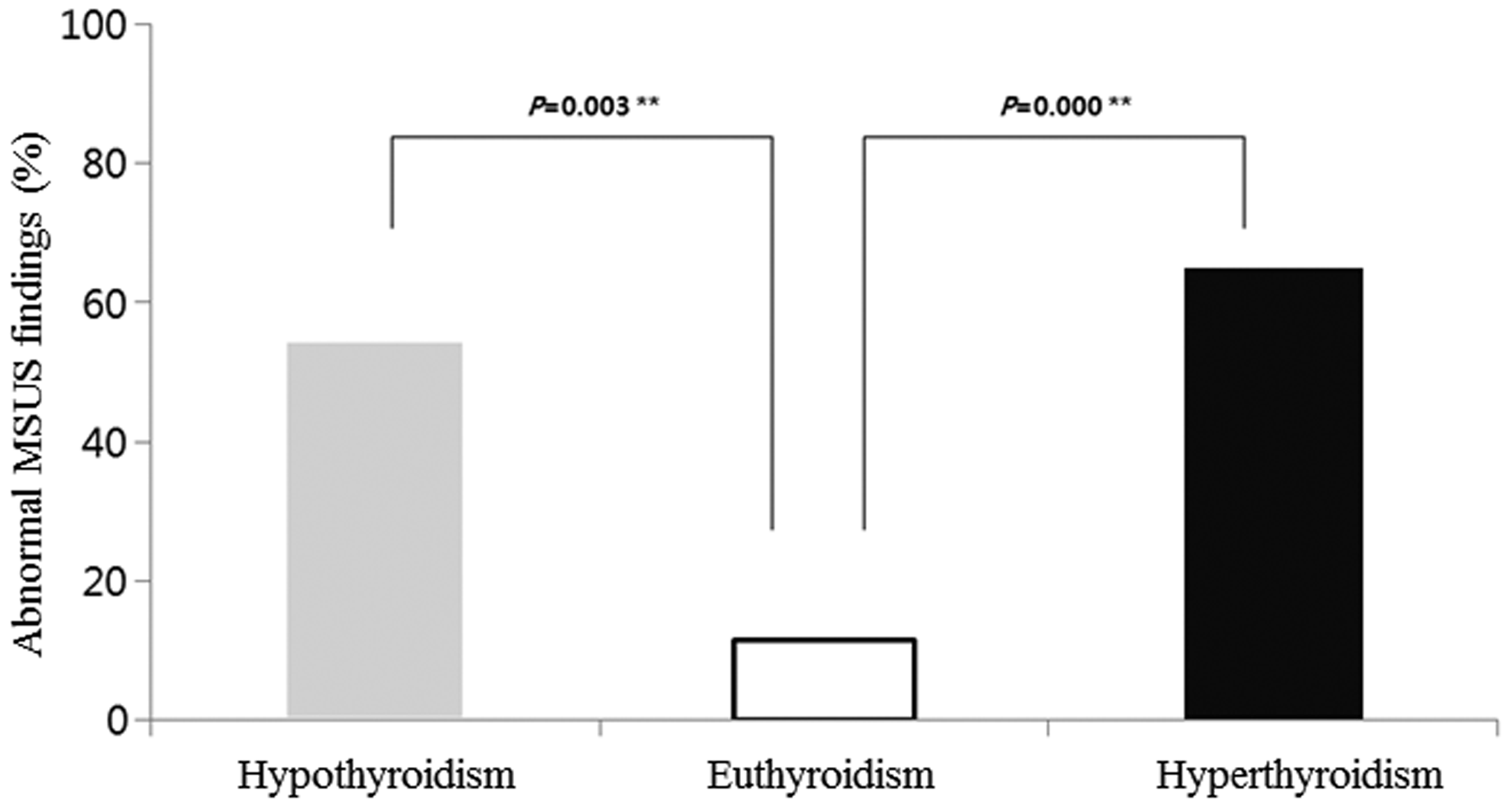
Frequency of abnormal MSUS findings according to thyroid status.
Univariable and multivariable analysis of factors associated with overall MSUS severity score for the patients with or without knee osteoarthritis.
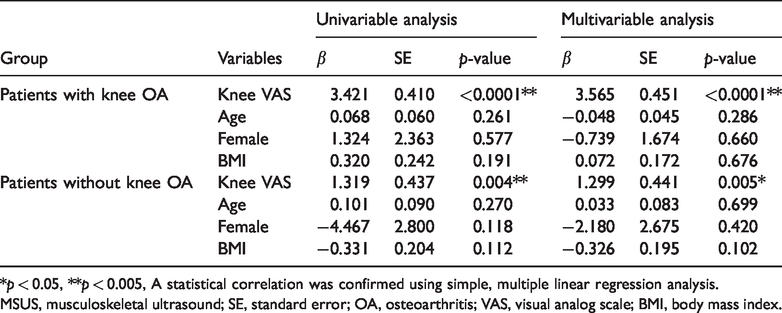
*p < 0.05, **p < 0.005, A statistical correlation was confirmed using simple, multiple linear regression analysis.
MSUS, musculoskeletal ultrasound; SE, standard error; OA, osteoarthritis; VAS, visual analog scale; BMI, body mass index.
Discussion
A previous study showed that pain sensitivity was related to thyroid function, which may be due to changes in hormone levels. 25 Another study involving 20 patients who had polyarthralgia with CLT without known rheumatic diseases showed that the number of painful joints was correlated with TSH levels. 26 Based on this relationship between thyroid disease and arthropathy, our study aimed to evaluate whether MSUS abnormalities were associated with thyroid dysfunction. MSUS can detect very small effusions or synovial hypertrophy in the knee joint that can otherwise be missed clinically. Even the scant synovial fluid in the knee joint can be detected in scans of the suprapatellar recess with MSUS. 27
Among thyroid dysfunction, hypothyroidism has been well recognized as typically affecting the knees, metacarpophalangeal joints, proximal interphalangeal joints, and metatarsophalangeal joints.14–16 Synovial fluid of the knee joints in these patients is noninflammatory and has increased viscosity.16,28 It has been suggested that TSH can increase the production of synovial fluid by hyaluronic acid and proteoglycan synthesis.15,29 In our study, compared with euthyroid patients, hyperthyroid and hypothyroid patients had increased joint effusion and overall MSUS severity score. Most of our patients were regarded as grade 0 or 1 according to the EULAR- OMERACT combined scoring system for grading synovitis. 19 Among the abnormal MSUS findings of knee joints, the only significant difference between the euthyroid group and thyroid dysfunction group was in the joint effusion grade. The frequency of abnormal MSUS findings of knee joints was significantly higher in the thyroid dysfunction group. These results demonstrate the correlation between abnormal MSUS findings of knee joints and thyroid dysfunction. In addition, high knee VAS score of the patients was associated with MSUS abnormalities. This reflected agreement between clinical symptoms and MSUS findings. In the clinical setting, patients with diagnosed thyroid dysfunction, in whom the thyroid dysfunction remains uncontrolled and who complain of joint pain, may be assessed using MSUS to find the cause. Moreover, a thyroid function test may be warranted in patients with an unexplained complaint of arthralgia.
Our study had some limitations. First, the number of patients was relatively small. Second, we did not compare knee MSUS abnormalities of patients with thyroid diseases to those of healthy controls matched for age, sex, and BMI. By analyzing factors affecting knee MSUS abnormalities, we tried to overcome this problem. Third, most of the patients had already been diagnosed with thyroid disease, medicated, and had followed up. Therefore, we suggest that further studies should follow up the serial changes in MSUS abnormalities of the knee joint before and after the treatment of patients with newly diagnosed thyroid disease. In a previous study, hypothyroidism was shown to be associated with inflammatory forms of arthritis as well as non-inflammatory arthritis, such as osteoarthritis. 30 Hypothyroidism is often associated with CPPD arthritis.10,11 The prevalence of gout is higher in both hypothyroid and hyperthyroid subjects than in euthyroid subjects. 31 In our study, there was no correlation between thyroid dysfunction, presence of thyroid antibodies, or MSUS PD signal indicating inflammation. Additional prospective studies involving large populations are required to elucidate the correlation between thyroid dysfunction status, thyroid autoantibodies, and inflammatory arthritis.
Key message
MSUS abnormalities correlated with knee arthralgia in patients with thyroid dysfunction. Thyroid function tests should be considered for unexplained arthralgia.
Footnotes
Acknowledgements
The authors thank Su Yeon Park (Department of Biostatistics, Soonchunhyang University Seoul Hospital) for her assistance with statistical analysis. The authors also thank Kyung Min Moon (Department of Pulmonary, Allergy and Critical Medicine, Gangneung Asan Hospital, University of Ulsan College of Medicine) for his assistance with creating figures.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study is supported by funding from Soonchunhyang University.