
Abstract
The current paper presents a case report of lower eyelid reconstruction after removal of a basal cell carcinoma. Our novel reconstruction method consists of translation and rotation of a paramedian forehead flap into the defect, conjunctivorhinostomy for reconstruction of the nasolacrimal duct, and placement of a sandwich ear cartilage graft that is primarily seated into the forehead flap to maintain the vertical dimension of the eyelid. This “all-in-one” technique has the advantage of one-step reconstruction, avoiding multiple surgical procedures.
Keywords
Introduction
Repair of lower eyelid full-thickness defects is one of the most challenging tasks in reconstructive surgery because of the particular structure of the eyelid and requirement for high operative accuracy. 1 The aesthetic and functional roles of the lower eyelid (e.g., maintaining the air–tear interface and facilitating tear drainage) as well as its mobile nature require the surgeon to perform a very delicate operation for reconstruction of this anatomically complex region. 2
Over the years, different types of local flaps have been used to reconstruct the lower eyelid after oncologic surgery or trauma. 3 Poorly treated defects can result in secondary complications such as keratitis, corneal ulceration, ectropion, entropion, ptosis, or epiphora. 1
Our novel reconstruction method consists of translation and rotation of a paramedian forehead flap into the defect, conjunctivorhinostomy for reconstruction of the nasolacrimal duct, and placement of a sandwich ear cartilage graft that is primarily seated into the forehead flap to maintain the vertical dimension of the eyelid.
Case report
A 60-year-old Caucasian woman (Figure 1) with a history of prolonged sun exposure (farmer) presented with a basal cell carcinoma of the right lower mid-half eyelid and infraorbital region. She had no other comorbidities and stated that the tumor had appeared 1 year previously and was treated with topical antibiotic ointments. Ophthalmological examination showed epiphora; conjunctival inflammation, which was treated with tobramycin eye drops for 7 days preoperatively; and no eye movement restrictions. A computed tomography scan showed no bone resorption in the vicinity of the tumor.

Basal cell carcinoma of the right inferior lower eyelid
During surgical reconstruction, a wide full-thickness resection was performed, consisting of about 80% of the lower eyelid, infraorbital and lateronasal skin, subcutaneous tissue, and periosteum of the infraorbital rim; the lateral aspect of the nasal bones were resected as well (Figure 2). Frozen sections during surgery were performed to ensure that the resection edges were free of tumor tissue. An ipsilateral paramedian forehead flap was raised for translation into the defect, and conjunctivorhinostomy was performed to reconstruct the nasolacrimal duct and prevent epiphora (Figure 3). A sandwich cartilage graft was prepared to maintain the vertical height and tarsal-like support of the new eyelid. A 2 × 1 cm cartilage graft was harvested from the same side as the defect and placed inside the flap between the subcutaneous and musculoaponeurotic layers of the forehead flap (Figure 4). The auricular cartilage was sutured at the site of the flap, and the flap was anchored laterally at the periosteum and medially to the canthal ligament. Suture closure was performed in layers, and the permeability of the reconstructed nasolacrimal duct was maintained with a silicone stent that was removed after 3 months. Thinning of the flap base was performed simultaneously (Figure 5).
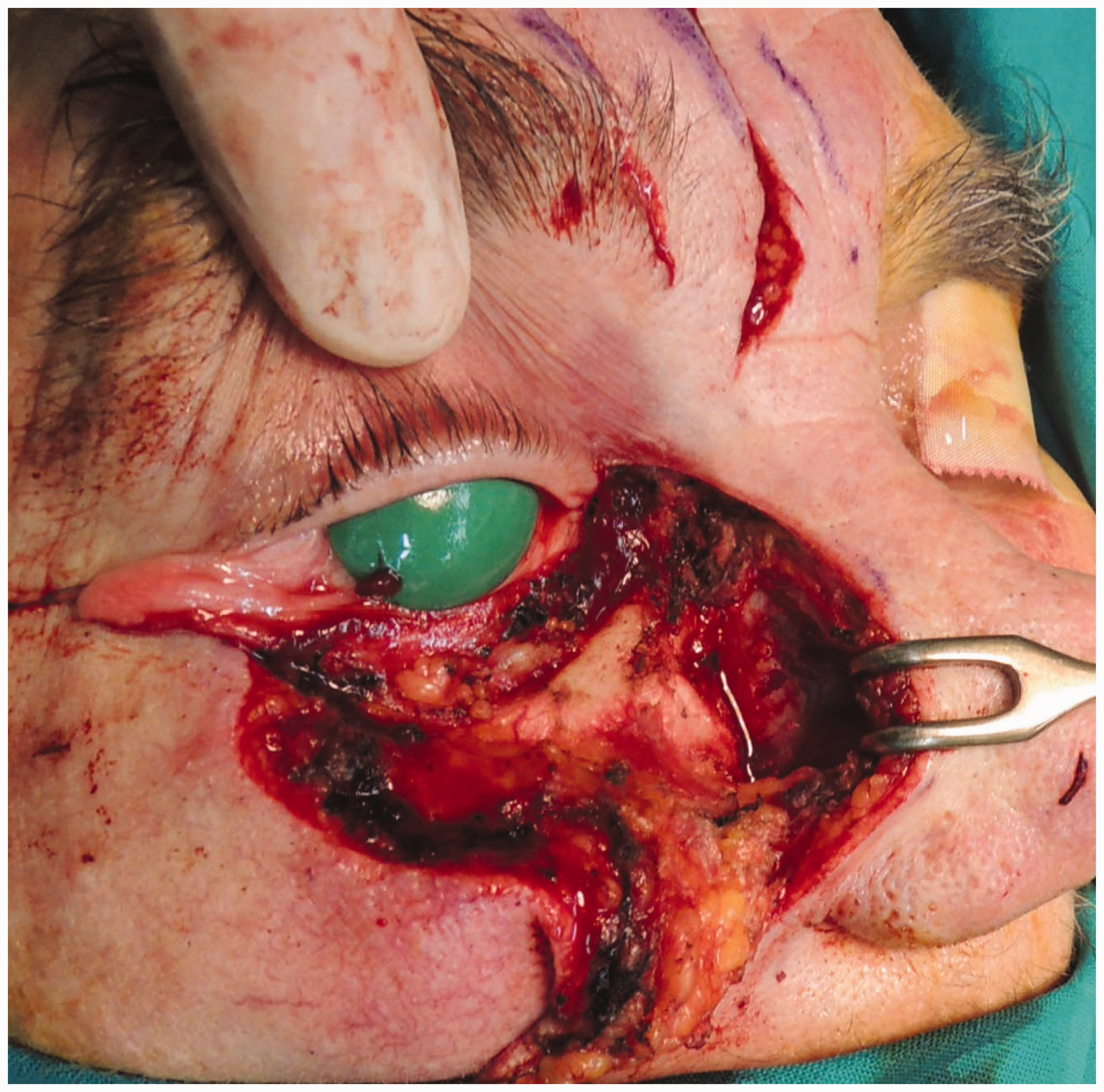
Tumor resection

Forehead flap and reconstruction of the nasolacrimal duct. A silicone stent is used to create the new duct

Placement of a “sandwich” cartilage graft inside the flap

Translation of the forehead flap to the reconstructed site
Postoperatively, the patient presented good esthetics and functional rehabilitation, and no signs of epiphora, keratitis, ectropion, or wound healing impairment were seen (Figure 6). Frontal flap debulking was performed in a second-stage surgery. Lower eyelid retraction with inferior scleral show (2 to 3 mm) was present postoperatively.

Postoperative image at 3 months after pedicle detachment
The Ethics Committee of the Iuliu-Hatieganu University of Medicine and Pharmacy, Cluj-Napoca, Romania approved the study protocol. The patient provided written informed consent.
Discussion
A few basic principles should be kept in mind when considering full-thickness lower eyelid reconstruction; the main consideration is assurance of functional rehabilitation followed by tissue coverage and good esthetics. Normal tear film maintenance is necessary for corneal clarity and patient comfort. 4
Most lower eyelid defects are caused by surgical excision of a neoplasm, as in our case, but they can also be caused by burns, trauma, infections, or congenital colobomata. 4 Basal cell carcinomas are locally invasive periocular skin cancers that affect the lower eyelids more than the upper eyelids, 5 and various reconstruction methods have been proposed for full-thickness defects caused by such lesions: a nasojugal flap with dermal pennant, 5 an angular artery island flap, 2 a semicircular flap with a periosteal flap, a tarsoconjunctival flap, 4 a pericranium graft and Mustarde flap, 6 and a modified cheek advancement flap. 7 All of these reconstruction techniques can give good function and esthetic results, but they are not perfect. Full-thickness lower lid reconstruction is traditionally performed in a few stages: inner and outer layer soft tissue reconstruction, support tissue reconstruction, and further flap molding. Orgun et al. 1 performed a 10-year retrospective study of oncoplastic lower eyelid reconstruction analysis and found that reconstructions based on a horizontal trajectory resulted in lower rates of ectropion and ptosis than those based on a vertical trajectory. Therefore, our flap design was based on a horizontal trajectory to prevent these complications. Furthermore, the sandwich technique using interpositioned ear cartilage provides better support for the translated flap, and the donor site has a good esthetic appearance after surgery (Figure 6).
The created pocket fits the size of the cartilage graft perfectly, minimizing dead space and increase the rate of graft intake. The presented technique has the advantage of using solid cartilage placed between the subcutaneous and musculoaponeurotic layers of the flap, which results in a high survival rate because the graft obtains its blood supply from all four directions. Although the flap viability can theoretically be affected by partial splitting, this did not occur in our patient. The remaining width of the flap was adequate for blood perfusion. The standard forehead flap is commonly used in nasal reconstruction.11–15
Coverage of the osseous nasal defect by a flap is mandatory, and other methods such as skin grafts are inappropriate for these type of defects. Defects larger than 2 cm typically require the use of an interpolated flap. 16
Obstructed or surgically affected nasolacrimal ducts are managed by stent implantation or dacryocystorhinostomy,8,9 in which a stent remains in place and is subject to further obliteration. Our method of nasolacrimal drainage involves reconstruction of the duct with nasal mucosa and removal of the stent 3 months postoperatively to decrease the risk of future obstructions. New research in stem cell reconstruction should provide even better methods of duct repair. 10
In conclusion, this novel technique can allow for “all-in-one” management of full-thickness lower eyelid defects. It has the advantage of avoiding an extra step of reconstruction, and only one extra surgery is required for debulking of the frontalis flap. Further studies should help to elucidate the outcomes of this technique.