
Abstract
Exanthematous diseases are common in childhood, and varicella is one of the most frequent. We present the case of a 10-year-old girl with partial avulsion of the nasal tip reconstructed with an ipsilateral forehead flap. During her hospital stay, she developed a primary varicella-zoster virus infection, in which the skin lesions also appeared on the forehead flap. Due to its unusual nature, it is important to understand the evolution of a flap affected by systemic dermatosis.
Introduction
Exanthematous diseases are common pathologies during childhood, and most adults have been infected by their etiological agents. Varicella is probably the best known of these dermatoses. Its etiological agent is the varicella-zoster virus (VZV), which corresponds to Herpesvirus 3, an alphaherpesvirus. This virus establishes a latent infection in the dorsal root ganglia. When it reactivates, it causes an infection known as herpes zoster (HZ). This entity is well known and usually occurs as a complication of various pathologies that alter the immune response, such as after postoperative stress. However, primary infection does not usually occur after surgical procedures within a hospital setting, where there are no potential disease transmitters.1,2
Throughout history, infectious diseases of the integumentary system, which is considered the largest organ in the body, have been described. Based on this, it would be logical to think that in cases where skin flaps involve donor tissue, whether local, regional, or remote, the clinical manifestations of these dermatoses would continue to be expressed, but in the new recipient site. 3
The forehead flap was first used by Susruta Samhita in 700 BC. Important figures have made contributions and technical modifications to this procedure. Thus, the frontal flap has been perfected to reconstruct nasal units and subunits with a high degree of aesthetic finesse. The forehead flap is a great tool for repairing missing skin units.
We know that flaps can be affected by endogenous and exogenous factors due to a physicochemical process during the adaptation and healing stage. A hyperadrenergic state caused by nerve fiber section has also been reported. The release of oxygen radicals by damaged cells produces the release of prostaglandins, nitric oxide, and HIF1A, which promote vasodilation and antiplatelet aggregation. In addition to this, an increase in blood perfusion maintains the flap vitality, subsequently promoting neovascularization; thanks to endothelial cells and vascular endothelial growth factors. 4
In general, once a pedicled flap has integrated into the recipient bed, the cutaneous layer regains some of its original architecture and inherent properties, for example, hair growth, pigmentation, sensitivity, and sweating. Alterations in sensitivity and the involution or growth of skin appendages can occur up to a year after surgery. Based on the above, it is clear that a skin flap can be a target of multiple skin diseases. 5
Case report
A 10-year-old female patient with no relevant medical history was taken to the emergency department after suffering a dog bite with partial avulsion of the nasal tip. During the physical examination, a complete amputation of the alar subunit and a partial amputation of the dorsum and nasal tip on the right side were found (Figure 1). Complete reconstruction was performed using an ipsilateral paramedian frontal flap and auricular concha cartilaginous graft to restore the medial and external crura and mucosal flaps for internal coverage. The modeling and plication of the distal portion of the frontal flap allowed the restoration of the alar contour and provided a minimum contribution to the internal coverage.

A 10-year-old female with a nasal defect due to a dog bite. (a) The frontal view shows complete avulsion of the nasal ala and partial avulsion of the nasal dorsum and tip. (b) The oblique view shows the extent of the defect. (c) Appearance on the seventh day after the onset of the dermatosis. Some vesicles and scabs are still seen.
On the seventh day of hospitalization, she developed a mid-face, scalp, and trunk dermatosis characterized by an erythematous rash that evolved into pruritic vesicles, pustules, and scabs. Doppler ultrasound was utilized to assess the viability of the flap. The lesions evolved through the different phases in 12–48 h and were simultaneously present in all stages of development. The relevance of this case was the appearance of lesions in the frontal flap, in greater quantity and with the different stages of development coexisting throughout the territory of the flap, including the scalp (Figure 2). The patient also had a fever of 38.7°C, general malaise, and myalgia of moderate intensity for 2 days.

Evolution of the forehead flap and varicella-zoster virus involvement. (a) Appearance on the third day after the start of infection. The different phases of the infection are seen mainly in the middle area of the forehead and throughout the entire extension of the flap. (b) Sequence of the follow-up after the release and modeling of the forehead flap. Postoperative view at 6 months. The nasal flap appears to have moderate hyperpigmentation. The donor area of the forehead flap shows small areas of hypertrophic scarring; stigmas from the skin lesions caused by varicella on the cheek can also be seen. (c) Postoperative view at 12 months. (d) Frontal view of the donor site scar at 18 months, presenting a well-healed and aligned appearance, with noticeable symmetry in the brows.
An assessment was requested from the Pediatric service, and primary VZV infection was diagnosed, confirmed with a viral polymerase chain reaction swab of the lesions made on the ninth day of hospitalization. There is no documented prior contact with an infected individual within the family, nor any reported history of VZV infection or varicella vaccination. Nonetheless, the risk of a surgical site infection remains a concern, particularly due to exposure to surgical smoke, as the potential transmission of VZV during flap placement has been well-documented. Numerous in vitro and in vivo studies have highlighted these associated risks. According to Mahdood et al., these findings emphasize the critical need for effective measures to minimize exposure to surgical smoke and ensure strict adherence to infection control protocols to mitigate the risk of VZV transmission. 6 Based on this, we temporarily isolated the patient for 7 days and periodically reviewed the integrity of the flap. Treatment consisted of management with acyclovir and paracetamol. The patient was discharged on the ninth day after the onset of the rash for outpatient management. She had mostly crusted lesions. The viability and integration of the frontal flap in the recipient area were satisfactory by the third week, and there was also adequate time to prevent the infectious stage of VZV and carry out forehead flap separation. The release and shaping of the flap were carried out without complications; only small, pigmented areas left by the scabs were observed.
At the 6-month follow-up, good alar and nasal tip contour and adequate nostril symmetry were observed. No varicella stigmas were found, only mild hyperpigmentation and hair growth, solved by laser hair removal (Figure 2).
Discussion
The use of a frontal flap to cover a nasal defect has a high survival rate and provides excellent architectural adaptation to the recipient bed. Thanks to this, good aesthetic-functional results have been described.
We searched the literature on exanthematous diseases affecting different flaps and their possible complications; however, information was scarce. HZ in flaps has been reported in the literature, mainly in those that include a neurovascular pedicle, in which reactivation of a skin infection follows the dermatome of the recipient and the donor bed. 7
We believe that a flap already well integrated into the recipient bed may be prone to developing generalized and regional skin diseases. A larger neovascular network possibly contributes to this, and the subsequent release of cytokines, prostaglandins, and vascular endothelial growth factors make it an area with high metabolic activity. This factor can make flaps equally or more susceptible to exanthematous dermatosis; hence, it is important to start antiviral treatment early to limit disease expression and prevent a variable against adequate flap integration.
Tomita and Inoue document a case where HZ manifested in a transplanted rectus abdominis musculocutaneous flap 14 months following chest wall reconstruction for recurrent breast cancer. It was concluded that the VZV traveled along reinnervated sensory nerves, originating from the dorsal ganglia, passing through the intercostal nerves, and eventually reaching the skin of the flap (Table 1). 8
Literature review.
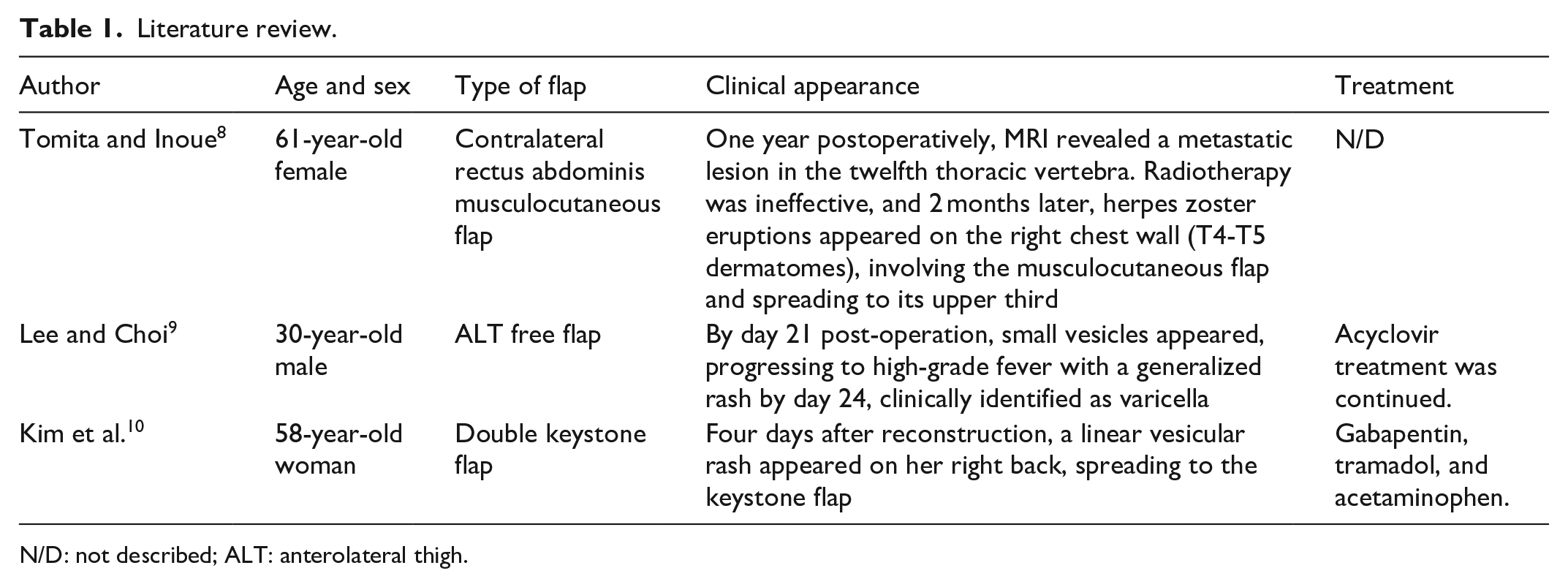
N/D: not described; ALT: anterolateral thigh.
Lee and Choi report a primary varicella infection in the forearm in a free ALT flap in an adult treated with acyclovir and symptomatic management. The flap did not suffer any damage from the disease. 9 Kim et al. report VZV reactivation in flaps in two breast reconstruction patients and one patient with an arm reconstruction due to trauma, although they do not report the type of flaps. HZ appeared from 21 days to 6 years. The authors consider that HZ is evidence of flap reinnervation (Table 1).10,11
We have not found reports in the literature of a similar VZV primary infection in a forehead flap in a pediatric patient; therefore, flaps may have the same possibility of suffering dermatosis as in the described case.
Conclusion
Primary varicella infection does not seem to represent a risk for the flap integration since, in general, traditional treatment with antivirals and symptomatic management was provided. We consider collecting more studies with similar characteristics pertinent to obtain sufficient information about the physicochemical changes when a flap is taken to its recipient site and its autonomization process. Due to its unusual nature, it is important to understand the evolution of a flap affected by a systemic dermatosis for decision-making and to prevent complications.
Finally, the information on this topic opens a perspective to new reports that increase our knowledge about how exanthematous diseases can appear on skin covered by flaps.
Learning points
This case report illustrates how a viral infection such as varicella-zoster can affect a local flap. However, this should not compromise the integrity or viability of the flap as long as the infection is promptly and appropriately addressed, as would be the case in any other scenario.
Flaps affected by varicella zoster should not be a cause for alarm; therefore, standard care and management procedures should be followed.
Footnotes
Acknowledgements
We thank Sergio Lozano-Rodriguez, MD, MWC, for his help in editing this manuscript.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for publication
Complete written informed consent was obtained from the Legally Authorized Representative of the minor patient and assent from the minor for anonymized patient information to be published in this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) of the minor patient and assent from the minor for anonymized patient information to be published in this article.
Author contributions
R.M.M.: Surgeon, data collection, translated paper. D.E.S.M.: Surgeon, data collection. E.A.P.: Surgeon, data collection. M.F.O.C.: drafted paper. C.M.G.C.: data collection, translated paper, paper revision. E.J.V.: drafted paper. Y.C.G.: Surgeon, data collection, informed consent statement.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge financial support by Plastic, Aesthetic, and Reconstructive Surgery from the Hospital Universitario “Dr. José Eleuterio González.”
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.