
Abstract
Primitive neuroectodermal tumours (PNETs) are rare malignant small round cell tumours. Notably, despite widespread reports of PNET in multiple parts of the body, it is extremely rare in the pelvis. Here, a rare case of giant PNET of the pelvis, that was treated with surgical intervention comprising hemipelvectomy and amputation, is reported. A 42-year-old female patient presented with an enlarged mass on the left hip and severe pain in the left lower extremity for the previous 6 months. Preoperative imaging examinations indicated an irregular soft tissue-like signal shadow sized 19 × 15 × 12 cm at the left ilium and sacrum. After surgical intervention involving left hemipelvectomy and amputation, the tumour was diagnosed by pathology as PNET. During the courses of postoperative radiotherapy and chemotherapy, local recurrence and distant metastasis occurred, and the patient died 9 months following surgical treatment. To the best of the authors’ knowledge, the current case is the largest pelvic PNET resection reported to date. Pelvic PNET is extremely malignant and has a high mortality rate regardless of surgical treatment, however, surgical resection of the lesion may relieve the symptoms, extend life, and improve quality of life to a certain extent.
Introduction
Primitive neuroectodermal tumours (PNETs) are a rare type of malignant small round cell tumour originating from the primitive neuroepithelium. 1 In the current reclassification of bone and soft tissue tumours by the World Health Organization (WHO), PNET and Ewing sarcoma were discussed in the same group. 2 PNETs tend to occur in neuroepithelial cells of the central nervous system and the peripheral mesenchymal tissues, and thus, are classified as central (cPNET) and peripheral (pPNET) types, respectively. The cPNETs occur mostly in the brain and spinal cord, and pPNETs are relatively common in the chest wall and limbs, but are extremely rare in the pelvis. 3 Herein is described an uncommon case of giant pelvic PNET that was treated with surgical intervention comprising hemipelvectomy and amputation.
Case report
A 42-year-old female patient was initially admitted to Jiangxi Provincial People’s Hospital Affiliated to Nanchang University in August 2015, with an enlarged mass on the left hip and severe pain in the left lower extremity for the previous 6 months, and with a prior diagnosis of lumbar disc herniation that she had received in a private clinic. Conservative treatment recommended by a previous hospital was ineffective, however, and the mass on the left hip had increased rapidly within the two weeks prior to being admitted to the Department of Orthopaedics, Jiangxi Provincial People’s Hospital Affiliated to Nanchang University. Physical examination showed a 25 × 15 × 10 cm mass on the left hip with poor mobility and local superficial venous engorgement. Imaging examination, using a 64-slice spiral computed tomography (CT) system (Siemens, Erlangen, Germany) and a 3.0T magnetic resonance imaging (MRI) system (Siemens), indicated apparent bone destruction of the left ilium and sacrum, as well as the invasion of left hip and iliopsoas muscle groups. Irregular soft tissue-like signal shadows with unclear boundaries were also visible, covering an area of approximately 19 × 15 × 12 cm (Figure 1a and b). Pulmonary CT images were also reviewed and suggested that two small nodules were visible in the dorsal segment of lower lobe of the right lung. In addition, tumour puncture biopsy results showed that the small round tumour cells were diffusely distributed, and were of consistent size. Immunohistochemical analyses of the biopsy indicated that the tumour was positive for CD99 antigen and neuron-specific enolase (NSE), and negative for cytokeratin (CK) and S-100 protein. Based on the above findings, the patient was diagnosed with PNET and was scheduled to undergo a left hemipelvectomy and amputation.

Preoperative computed tomography (CT) and magnetic resonance imaging (MRI) in a 42-year-old female patient during an initial hospital visit due to an enlarged mass on the left hip and severe pain in the left lower extremity, showing: (a) preoperative mass on the left hip of approximately 19 × 15 × 12 cm (CT image); and (b) preoperative irregular soft tissue-like signal shadows with unclear boundaries (MRI scan image).
The patient underwent surgery following three courses of neoadjuvant chemotherapy. Each course comprised intravenous infusion of 250 mg/m2 cyclophosphamide (Cytoxan®) for 7 consecutive days, then i.v. infusion 40 mg/m2 doxorubicin (conventional) (Adriamycin) plus 2.0 mg/m2 vincristine on day 8, followed by a 2-week rest. Intraoperative exploration of the iliac fossa revealed a large retroperitoneal soft tissue tumour, the top of which reached the costal margin, and partial bone destruction of the left sacrum. Subsequently, the tumour, left hemipelvis and left lower extremity were successively resected, and the maximum diameter of the tumour was found to be 19 cm, accompanied with liquefaction, haemorrhage and necrosis. The patient’s preoperative pain symptoms were significantly relieved following surgery, indicated by a reduction in visual analogue scale (VAS) score from 8 points before surgery to 2 points at 1 week following surgery. Postoperative pathological examination of the excised tumour tissue revealed large and small round tumour cells with fine and granular nuclear chromatin, and mitotic figures were common. Immunohistochemical evaluation showed that the tumour cells were positive for CD99, NSE and synaptophysin (Figure 2), and were negative for CK and S-100. Based on these findings, the diagnosis of PNET was confirmed

Postoperative pathological examination of tumour tissue sections showing: (a) fine and granular nuclear chromatin, with large and small round tumour cells, and mitotic figures were common (haematoxylin & eosin staining, original magnification × 40); and immunohistochemical staining of tumour tissue sections, showing (b) strongly positive signal for CD99 antigen; (c) positive signal for neuron-specific enolase; and (d) positive signal for synaptophysin (En Vision; b, c and d original magnification × 400).
At 2 weeks following surgery, the patient was transferred to the oncology department of Jiangxi Provincial People’s Hospital Affiliated to Nanchang University for further treatment, comprising 54 Gy of radiotherapy delivered at a dose of 2.0 Gy once per day, and three courses of chemotherapy. Each chemotherapy course comprised 250 mg/m2 cyclophosphamide (Cytoxan®) by intravenous infusion for 7 consecutive days, then i.v. infusion 40 mg/m2 doxorubicin (conventional) (Adriamycin) plus 2.0 mg/m2 vincristine on day 8, followed by a 2-week rest. A 2 months following surgery, she experienced severe lumbar pain during chemotherapy. MRI of the lumbar spine showed obvious bone destruction of the lumbosacral vertebra, and local recurrence and metastasis of the tumour was considered (Figure 3). In addition, the pulmonary CT scan was reviewed and suggested that there were multiple metastases in both lungs. At the end of the whole chemotherapy cycle, the patient abandoned the treatment and self-discharged from hospital. The patient died 9 months after surgery.

Postoperative lumbar spine magnetic resonance imaging scan at 2 months post-surgery, showing obvious bone destruction of the lumbosacral vertebra, thus local recurrence and metastasis of the tumour was considered.
This study was conducted in accordance with the declaration of Helsinki and with approval from the Ethics Committee of Jiangxi Provincial People’s Hospital Affiliated to Nanchang University. Written informed consent to publish the case was obtained from an immediate family member (legal proxy) of the patient.
Discussion
Primitive neuroectodermal tumour was first reported by Stout et al. in 1918, 4 and first proposed by Hart and Earle in 1973, 5 while Ewing sarcoma was first reported by Ewing et al in 1921. 6 With subsequent in-depth research, Ewing sarcoma was found to lack the Homer-Wright (H-W) chrysanthemum-like cluster arrangement that is a structural characteristic of PNET under the light microscope. 7 In addition, immunohistochemical analyses show that Ewing sarcoma cells only express one or no neural differentiation markers, while PNET cells often express two or more markers. 8
Most cases of PNET involve individuals aged under 30 years, particularly children and adolescents, with a larger proportion of cases observed in males. 9 Imaging examinations of PNET are not specific and usually reveal invasive destruction and osteolytic changes, with extensive lesions that are poorly demarcated from normal bone. Thus, it is difficult or even impossible for surgeons to distinguish PNET from common malignant bone tumours through the clinical and imaging manifestations prior to surgery, and PNET diagnosis mainly relies on pathological examination. 10 In general, PNET specimens are fish-like, with a soft texture when necrosis occurs. Under the light microscope, the tumours are composed of uniform small round cells with unclear cell outlines and deep nuclear staining, as well as the characteristic H-W chrysanthemum-like cluster structural arrangement. Under electron microscopy, the cells are in their primitive form, with few organelles and a large amount of glycogen in the cytoplasm. In addition, immunohistochemistry shows that cells are often positive for CD99, which is a relatively specific marker for the diagnosis of PNET, particularly when combined with positive signals for at least two neural differentiation markers, such as NSE and synaptophysin. 11 In the present case, CD99 was diffusely expressed and strongly positive in the tumour tissue. Cells were also positive for synaptophysin and NSE, which concurred with the diagnostic characteristics of PNET.
In terms of treatment, previously published reports on PNET mainly focus on cases involving various parts of the body, and there is a general lack of large-sample cases analyses. Surgical resection of PNET of the pelvis is full of challenges, and to the best of the present authors’ knowledge, the current case is the largest pelvic PNET resection reported to date. The deep pelvic position provided sufficient space for PNET growth, and made it difficult to accurately assess the boundary distribution of the tumour in the present case. The main purpose of surgical treatment is to remove the tumours as far as possible within safe surgical boundaries. In this regard, hemipelvectomy and amputation are preferred for tumour resections that cannot retain sufficient marginal normal tissue and limb function.
As for malignant tumours of the pelvis, Cascella et al. 12 concluded that depending on the effect of neoadjuvant chemotherapy, satellite lesions may be eliminated as far as possible, oedema may also be alleviated, and the surgical boundaries may become clear, which could significantly improve the surgical outcome. Even if amputation is necessary due to the specific conditions, neoadjuvant chemotherapy plays a positive role in controlling the recurrence and metastasis of tumours, and improving prognosis.
Furthermore, PNET is highly invasive and prone to distant metastasis, and most patients die within 2–3 years after diagnosis. For example, in a report of 23 cases of PNET in multiple parts of the body, only two patients had a survival of 8 years, and the remaining 21 patients died within 3–9 months of diagnosis. 13 A retrospective analysis of 13 patients with spinal PNET, revealed that PNET was extremely malignant and had a high mortality rate regardless of whether the patients received surgical treatment or not, but surgical resection of the lesion could relieve symptoms, extend life, and improve quality of life to a certain extent. 14 Clinical data regarding previously reported cases of PNETs of the pelvic area are summarized in Table 1.14–21
Clinical data from cases of primitive neuroectodermal tumours of the pelvic area reported in the literature.
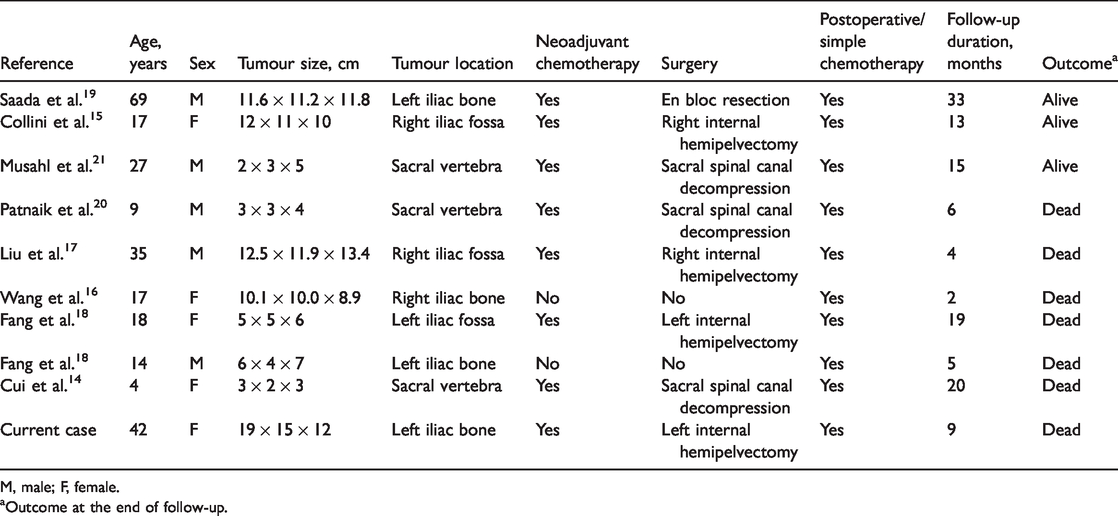
M, male; F, female.
aOutcome at the end of follow-up.
In conclusion, the case of a giant pelvic PNET is described, and to the best of the present authors’ knowledge, represents the largest pelvic PNET resection reported to date. PNETs of the pelvis are extremely malignant, and are associated with a high mortality rate regardless of whether surgical intervention is performed or not, however, surgical resection of the lesion may relieve symptoms, extend life, and improve quality of life to a certain extent. Furthermore, early diagnosis, well-designed systemic and local treatment plans, and as far as possible, the attainment of safe surgical boundaries during surgery, are the key points to improve the survival rate of patients with pelvic PNET.