
Abstract
Objective
To investigate the epidemiological profile and associated outcomes of electrical injuries at a major burn centre in southern China.
Methods
This retrospective study enrolled consecutive electrical burn patients admitted to the burn centre of the First Affiliated Hospital of Guangxi Medical University between 2008 and 2017. Demographic and clinical data and outcomes were recorded. Mann–Whitney U tests/Pearson’s chi-squared tests were used to examine the differences between low-voltage and high-voltage injuries.
Results
There were 217 high-voltage injuries and 159 low-voltage injuries. High-voltage burns were frequently observed between March and August, and low-voltage burns peaked between June and September. Burn patients were mainly men. Most burns occurred in participants aged 21 to 50 years and in industrial workers and electricians at work or householders at home. Only one person with high-voltage burns died (a mortality rate of 0.46%). Amputation rates were 37.33% for high-voltage burns and 22.01% for low-voltage burns. High-voltage injuries were associated with more extensive burns, longer hospital stays, and more complications and amputations.
Conclusions
More attention should be paid to prevention of electrical burns in male adults. Particular focus is needed on industrial workers, incidents in the spring and summer, and high-voltage injuries.
Keywords
Introduction
Electrical burns are one of the most important public health issues in industrial societies and can lead to serious outcomes and socioeconomic problems. Electrical burns are usually classed as high-voltage (≥1000 V) and low-voltage (<1000 V).1,2 Electrical arc flash burns, in which no current passes through the body, are usually considered a separate class and frequently cause superficial burns. By contrast, electrical burns (characterised by electrical current passing through the body) may result in deeper and more extensive burns than electrical arc flash burns, 3 and can result in higher morbidity and mortality.
Previous studies worldwide differ in reported prevalence and epidemiology for electrical burns. For instance, 94 patients with electrical burns were hospitalized in the Samsun Training and Research Hospital, Turkey, from 2008 to 2012; 4 47 patients sustained high-voltage injuries and 42 suffered low-voltage burns. In one burn care centre in Pakistan, 85 children presented with electrical burn injuries, 71.76% of these had high-voltage burns and there were 35 major limb amputations. 3 Of 202 patients with electrical injuries admitted to Motahari hospital in Tehran, Iran, between March 2011 and June 2012, 105 (52%) were construction workers. 5 Contact with overhead power lines was the main mechanism of injury and the findings showed that construction workers were exposed to more severe complications and invasive procedures. 5
Concomitant with advances in industrialization, there has been a high incidence of electrical burns in China in recent years. 6 A thorough understanding of the epidemiological profile of burns would contribute substantially to the prevention and treatment of electrical burn injuries. Although some studies have examined the epidemiology of electrical burns in different parts of China,6–9 there is no research on electrical injuries in southern China, which has undergone rapid industrial expansion. The Department of Burn and Plastic Surgery in the First Affiliated Hospital of Guangxi Medical University is one of the largest and most well-regarded burn centres, and treats burn cases from Guangxi and Guangdong in southern China. This study was conducted to examine the epidemiological characteristics of electrical burns over a 10-year period in the Department of Burn and Plastic Surgery, The First Affiliated Hospital of Guangxi Medical University. The associated outcomes were assessed with the intention of developing an evidence base for electrical burn injury interventions.
Patients and methods
Patient population and data collection
This retrospective study included 376 electrical burn patients admitted to the Department of Burn and Plastic Surgery, the First Affiliated Hospital of Guangxi Medical University, between January 2008 and December 2017. All participants had electrical burns caused by an electrical current. Patients with electrical arc flash burns and those admitted for later reconstructive surgery were excluded.
All patients received a standard treatment plan comprising fluid resuscitation, burn wound assessment and management, infection control, diagnosis and treatment of inhalation injury, nutritional support and rehabilitation.
The following data were recorded: current voltage, month, gender, age, population group, cause of burn, length of hospital stay, extent of burn, complications, mortalities and amputations. The study was approved by the ethics review committee of the First Affiliated Hospital of Guangxi Medical University (Nanning, China), and patient records/information were anonymized and de-identified prior to analysis. The informed consent requirement was waived owing to the retrospective nature of the study.
Statistical analysis
A standard descriptive analysis was performed and Mann–Whitney U tests or Pearson’s chi-squared tests were used to examine differences in length of hospital stay, total body surface area (TBSA) burned, complications, amputations and mortalities between groups exposed to different voltages. P < 0.05 was considered to indicate statistical significance. All tests were performed using IBM SPSS Version 22.0 (IBM Corp., Armonk, NY, USA).
Results
During the 10-year period, 566, 673, 656, 809, 666, 783, 737, 609, 670 and 749 burn patients were admitted in 2008, 2009, 2010, 2011, 2012, 2013, 2014, 2015, 2016 and 2017, respectively; of these, 32, 38, 35, 43, 37, 39, 41, 36, 36 and 39, respectively, sustained electrical burns. Thus, there was a relatively even distribution of cases throughout the study period, with an electrical burn incidence rate of 4% to 6% of all admitted burns each year. Of the 376 electrical burn patients, 217 (57.71%) had high-voltage burns (≥1000 V) and 159 (42.29%) had low-voltage burns (<1000 V).
Month
Most electrical burns occurred March to November, during which period 334 patients (88.83%) were injured; high-voltage burns were most frequently observed March to August (141/217, 64.98%) and most cases of low-voltage burns occurred June to September (103/159, 64.78%) (Figure 1a).

Distribution of electrical burns by month, gender, age, population group and cause.
Gender
Electrical burn injuries affected men more than women (336/376, 89.36% vs. 40/376, 10.64%, respectively); both high-voltage and low-voltage burn patients were mainly men (202/217, 93.09%; 134/159, 84.28%, respectively) (Figure 1b).
Age
The age of the 376 patients ranged from 1.3 years to 72 years (average: 34.61 years). A total of 74.47% (280/376) of patients were young (21–40 years) or middle-aged (41–60 years), 20.21% (76/376) were children (0–10 years) or adolescents (11–20 years), and only 5.32% (20/376) were older (61–80 years) (Figure 1c). Both high-voltage burns and low-voltage burns, respectively, were mainly observed in participants aged 21 to 30 years (43/217, 19.82%; 22/159, 13.84%), 31 to 40 years (61/217, 28.11%; 30/159, 18.87%) and 41 to 50 years (58/217, 26.73%; 33/159, 20.76%). Most children (0–10 years) (32/159, 20.13%) sustained low-voltage burn injuries (Figure 1c).
Population group
Most patients were industrial workers ([total] 118/376, 31.38%; [high voltage] 76/217, 35.02%; [low voltage] 42/159, 26.42%), followed by householders (84/376, 22.34%; 37/217, 17.05%; 47/159, 29.56%), electricians (78/376, 20.74%; 61/217, 28.11%; 17/159, 10.69%), preschool children (34/376; 9.04%; 10/217, 4.61%; 24/159, 15.09%), students (24/376, 6.38%; 11/217, 5.07%; 13/159, 8.18%) and farmers (24/376, 6.38%; 11/217, 5.07%; 13/159, 8.18%) (Figure 1d).
Cause
Work-related accidents (173/376, 46.01%) were the most common cause of electrical injuries, followed by electrical accidents indoors (73/376, 19.41%). A total of 16.76% (63/376) of electrical injuries were a result of electrical accidents outdoors and 11.44% (43/376) occurred as a result of electrical operations (Figure 1e). The pattern of injuries showed that 56.68% (123/217) of high-voltage burns were a result of accidents at work and 44.65% (71/159) of low-voltage injuries resulted from accidents indoors (Figure 1e).
Length of hospital stay and TBSA burned
Both length of hospital stay and TBSA burned were significantly correlated with voltage (Spearman’s rho, 0.328 and 0.497, respectively; P < 0.01). The length of hospital stay of the high-voltage burns group ranged from 2 to 814 days (median: 56 days), significantly longer than the hospital stay period of the low-voltage burns group (range: 2–154 days; median: 35 days) (U = 10641.000, P < 0.001). The TBSA observed for the high-voltage burns group ranged from 1% to 45% with a median of 5%, which was significantly more extensive than observed for the low-voltage burns group (range: 1% to 27%; median: 1%) (U = 7404.500, P < 0.001).
Complications and outcomes
There were more complications and major amputations in patients with high-voltage burns than in those with low-voltage burns (87.10% vs. 67.92%, P < 0.001; 25.81% vs. 5.03%, P < 0.001) (Table 1). Only one person with high-voltage injuries died from severe infection caused by multidrug resistant Pseudomonas aeruginosa, which resulted in a mortality rate of 0.46%; there were no significant differences in mortality rates between the two groups (0.46% vs. 0.00) (Table 1).
Complications and outcomes of electrical burns.

aAmputations of limbs or plus minor amputations.
bAmputations of fingers/toes.
The primary complication with the highest incidence was coma, followed by cardiac injury liver injury, compartment syndrome, shock, acute renal failure and lung injury (Table 2; Figure 2).
Main complications and combined injuries of electrical burns.
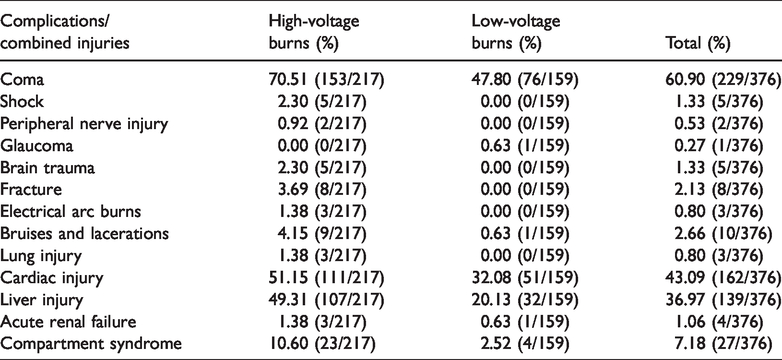

Main complications and combined injuries of electrical burns. ARF: acute renal failure.
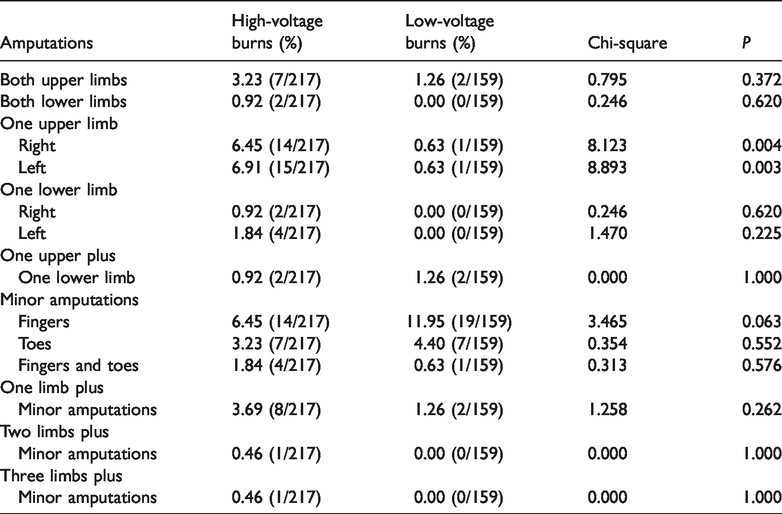
Eighty-one patients (37.33%) who had high-voltage burns had undergone amputations; of these, 56 had major amputations and 25 had minor amputations (Table 1). Amputations were performed on 35 patients (22.01%) with low-voltage burns, 8 of whom had major amputations and 27 minor amputations (Table 1). For major amputations, the amputation rates for one upper limb in the high-voltage burns group were significantly higher than those of the low-voltage burns group (right: P = 0.004; left: P = 0.003) (Table 3).
Amputation subtypes for electrical burns.
Discussion
Although not common, electrical burns deserve special attention. They comprise approximately 0.04% to 5% of all admissions to burn centres in developed countries, and up to 27% in developing countries. 2 During our study period, annual electrical burn injuries accounted for 4% to 6% of all annual admitted burns, suggesting a relatively low incidence of electrical burns in southern China. The percentage of high-voltage electrical burns (57.71%) was higher than that of low-voltage burns (42.29%), similar to previous study findings.1,4 In contrast, other studies10–13 have shown that low-voltage current is responsible for most electrical injuries. This discrepancy may stem from differences in the susceptibility of various populations.
In the present study, high-voltage burn injuries were more frequent between March and August (spring and summer), whereas low-voltage burns peaked between June and September (summer). This may be associated with intense industrial output and domestic electricity usage in these seasons in southern China. Of the 376 patients studied, men were the most vulnerable, a finding that reflects previous studies.6,14–16 This may be because men often engage in high-risk jobs and are more interested in electrical appliances. Similar to previous findings, 6 the results indicated that almost 75% of the total injuries occurred in young and middle-aged people, an energetic and active group. In addition, there were a substantial number of low-voltage burns in young children. Young children obviously are less able to judge danger and protect themselves, and may not always be protected by their families. Comparable to several previous studies, we found that a high percentage of burns occurred in industrial workers and electricians at work or householders at home.4,5,17,18 These accidents mainly resulted from unsafe machine operation, electricity manipulation and protection equipment. Thus, preventive strategies are crucial to reduce the incidence of electrical burns. Information about the use of outlet covers for connection elements and arc-fault circuit interrupters, rules for the standardization of the manufacturing of electrical devices, use of warning signs and other measures could be standardized and implemented across the country. In addition, knowledge about electrical injuries and proper use of electricity, awareness of self-protection and electrical operation compliance could be enhanced via public education programs in schools, companies and communities.
We found that patients with high-voltage burns had experienced longer hospital stays and had more extensive TBSA burns than those with low-voltage burns, a finding consistent with other study findings.4,6,19 High-voltage burns are characterised by greater energy release and deeper, more extensive tissue damage, resulting in longer hospital stays. These two factors are directly related to mortality rates. 20
Electrical injuries can lead to many complications. Our results and those of others indicate that high-voltage burns tend to result in complications.2,21 In the present study, coma was the most frequent complication, but usually resulted in transient loss of consciousness and left few mental or physical sequelae. Cardiac and liver injuries were easily identified from elevated levels of creatine kinase isoenzyme MB and liver enzymes and abnormal electrocardiogram. After symptomatic treatment, these injuries substantially improved. Despite their rare occurrence, shock and acute renal failure are life-threatening conditions. It is very important to use resuscitation as early as possible to avoid various complications, indicating the importance of intensive care and comprehensive treatment.
Electrical burns are characterised by heterogeneous mortality ratios ranging from 2.35% to 26.7%.2,3,17,20 In-hospital mortality in the present study was 0.46% for high-voltage burns and 0% for low-voltage burns. In our burn centre, acute electrical burn patients at high risk of death usually receive multimodality therapy and close monitoring in the intensive care unit. Then, they are transferred to the ordinary ward for further treatment when their condition has greatly improved. This procedure differs somewhat compared with other centres. Furthermore, owing to the improved transport system in southern China, many patients can access our centre and receive rapid professional treatment. However, it is possible that some patients eligible for this study died in basic hospitals or on the way to our centre.
Electrical burns are still a major risk factor for amputations. Amputations are generally performed because of massive necrosis of deep tissues caused by the current. Amputation rates for electrical injuries range from 10% to 68%. 22 During this study, we performed 56 major amputations and 25 minor amputations in patients with high-voltage burns, and 8 major amputations and 27 minor amputations in patients with low-voltage burns. The amputation rates were 37.33% for high-voltage burns and 22.01% for low-voltage burns. Additionally, high-voltage burns involved more amputations of one upper limb, probably because that upper limb was the most common current entry point.6,23 Amputations not only cause physical disabilities, but also psychological problems. Thus, a major challenge is to how to reduce amputations and reconstruct the function of injured limbs.
There were some study limitations. First, the sample did not include individuals who may have died at the scene of electrical burns, on the way to our centre or in basic hospitals; or individuals who did not seek medical care for social, economic or other reasons. Therefore, we could not obtain an exact estimate of the incidence of injury. Second, as this was a retrospective study, we could not assess long-term morbidity, learning disabilities, rehabilitation patterns or social costs. Third, this study was conducted at a single burn centre. Further well-designed multicentre studies are needed that include long-term follow-up to avoid the limitations of the current study.
In conclusion, electrical burns are an important public health problem. Their prevention should be emphasized in male adults, especially with respect to industrial workers, incidents in the spring and summer, and high-voltage injuries. Future multicentre studies with long-term follow-up are needed to provide a thorough knowledge of electrical burns in southern China and to develop strategies to improve interventions for electrical burns.
Footnotes
Acknowledgements
We sincerely thank the National Natural Science Foundation of China for supporting this work (grant no. 81801915). We also thank Dr. Gaoming Li (a statistician from Army Medical University) for providing helpful suggestions, and the doctors and nurses in our department for their management of burn patients and maintenance of detailed medical records.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the National Natural Science Foundation of China (grant no. 81801915) and by the Talent Programme of the Third Military Medical University (Army Medical University) (grant no. XZ-2019-505-065).