
Abstract
Objective
With the recent exponential increase in express deliveries across China, the number of patients with flame burns caused by electric bicycle battery chargers (BEBBC) has markedly increased in burn units. In this study, we aimed to characterize BEBBC to systematically explore measures to prevent their occurrence.
Methods
We performed a retrospective chart review of patients with flame burns who visited the Burn Department of Rui Jin Hospital between January 2015 and December 2021.
Results
Sixty-three patients with BEBBC and 1412 with types of other flame burn were included in this study. Fifty-six of the 63 BEBBC cases occurred between 9 pm and 7 am. BEBBC incidents involved a higher incidence of group burn in which multiple individuals were affected. Non-local patients with BEBBC were significantly younger than their local counterparts. BEBBC had a higher mortality than types of other flame burn.
Conclusions
The rising incidence of BEBBC calls for greater attention because of the associated high mortality and heavy burden on society. Enacting related legislation, disseminating information to the public, and improving treatment to control infection can help prevent BEBBC, increase its cure rate, and reduce patient mortality.
Introduction
In most burn centers in China, scalds are the predominant cause of pediatric burns whereas flames are the primary cause of burns in adults. 1 Compared with scald burns, flame burns usually have higher mortality and result in a longer length of hospital stay and greater medical expenses, placing a huge burden on patients and society. 2 Prompted by the boom in China’s online retail business, the volume of express deliveries in China made up approximately 60% of the total volume in 2016. 3 According to a report from the China Express Association, the number of delivery service personnel employed in 2019 was more than 3.2 million. Increasingly more people are moving from small villages, towns, or cities to large cities like Beijing, Shanghai, and Guangzhou, and many work in the delivery services sector. Among these workers, the main mode of transportation is the electric bicycle, becoming an indispensable piece of equipment for earning a living. Consequently, the incidence of flame burns caused by electric bicycle battery chargers (BEBBC) has shown a remarkable increase over recent years. In this study, we retrospectively investigated this type of flame burn to analyze its clinical characteristics and features, with the aim to identify effective methods to prevent the occurrence of BEBBC and reduce patient mortality.
Methods
Study design and population
We reviewed and analyzed the clinical information of patients with BEBBC as well as other types of flame burn who were admitted to the Burn Department of Rui Jin Hospital between January 2015 and December 2021. We searched for specific key words such as “electric bicycle battery charger” in combination with “flame burn” included in the medical history, and selected patients were included in the BEBBC group. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 4
The study protocol was approved by the Institutional Research Ethics Board (IREB) of Rui Jin Hospital, Shanghai Jiao Tong University School of Medicine (no. KY2023-392, 6 December 2023). A waiver of the requirement for informed consent was approved by the IREB owing to the retrospective nature of this study.
Data collection
All patient details were de-identified for privacy protection. The following demographics and clinical variables were collected: 1) basic patient information, including age, sex, body mass index (BMI), occupation, household registration, and concomitant diseases before injury; 2) accident factors, such as group or single admission and time of fire occurrence; and 3) diagnosis, including burn lesion size and depth, whether the burn injury was combined with inhalation injury or other complicated injury, laboratory tests, treatment (e.g., blood transfusion or surgery), infection, and outcomes.
Statistical analyses
Continuous data are presented as mean ±standard error of the mean and were compared using Student’s t-test for normally distributed variables. Categorical data are presented as number (percentage) and were compared using the chi-square test. P < 0.05 was considered statistically significant. All statistical analyses were conducted using GraphPad Prism version 6.01 (GraphPad Software Inc., San Diego, CA, USA).
Results
We collected and analyzed the data of 1475 patients with flame burn who were admitted to the Burn Department of Rui Jin Hospital between January 2015 and December 2021. Among the 1475 patients, 63 had BEBBC and 1412 had other types of flame burn (Table 1). The incidence of BEBBC and their proportion of total flame burn cases showed an increase over the study period (Figure 1). In terms of the seasonal distribution, there was no evident disparity among spring, summer, autumn, and winter.
Clinical information on BEBBC and other flame burns.
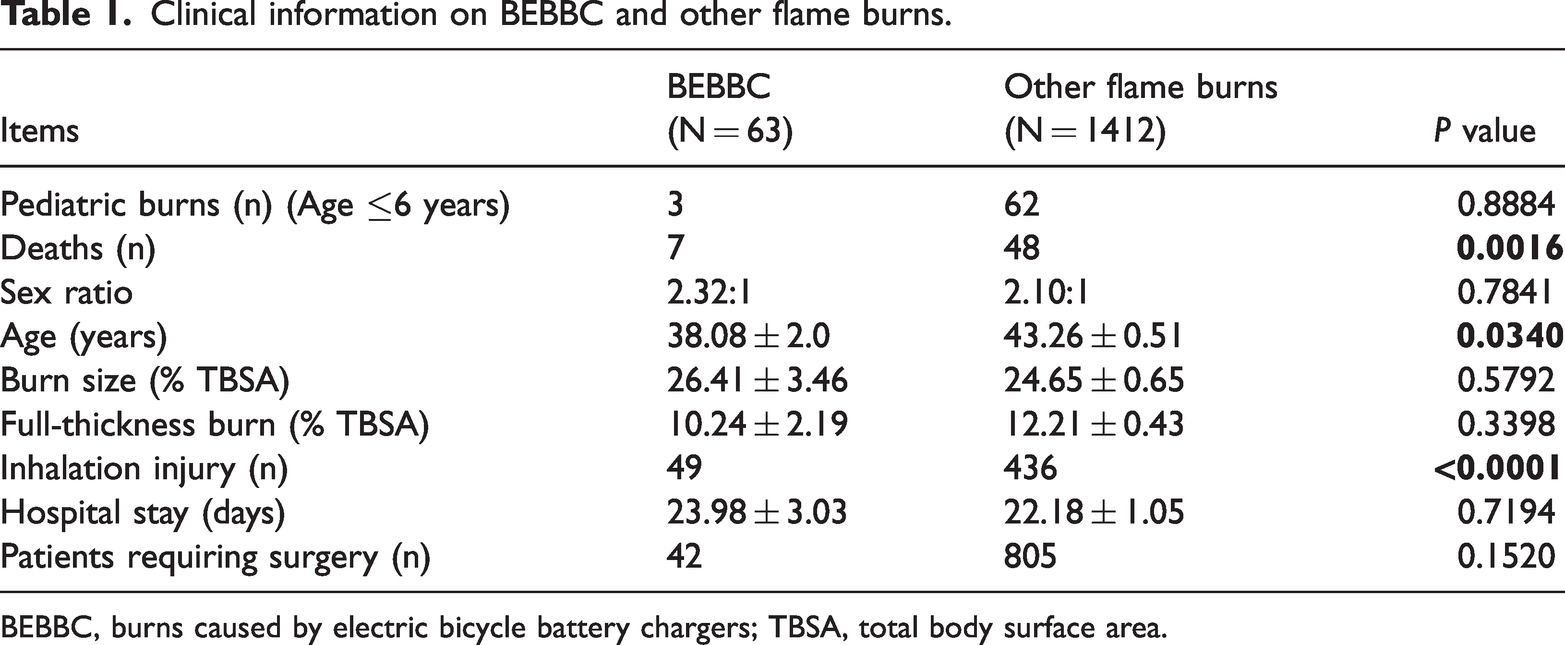
BEBBC, burns caused by electric bicycle battery chargers; TBSA, total body surface area.

Rate of burns caused by electric bicycle battery chargers (BEBBC), 2015–2021.
Most fire events resulting in BEBBC occurred during the night and early morning. Approximately 88.89% of BEBBC events occurred between 9 pm and 7 am. To escape the fire, seven people had to jump out of their building, and three of these patients experienced lumbar, humerus and ulnae, or metacarpal fractures. Other associated injuries included one case of brief coma. After inquiry, it was found that this patient was inebriated before the injury. Another two patients had corneal injury and four had soft tissue contusions.
Most BEBBC occurred in high-density living environments, which resulted in a significantly higher frequency of group burns (defined as at least two patients involved in the same fire event and simultaneously admitted to the emergency department), in comparison with patients who had other flame burns (58.73% vs. 8.29%, P < 0.0001) (Figure 2). The average number of patients in each incident was 1.95 ± 0.12 (median 2, and maximum 4).

Rate of patients with BEBBC and other types of flame burn. BEBBC, burns caused by electric bicycle battery chargers.
Patients with BEBBC were classified as local or non-local residents, according to their household registration. There were 44 male patients and 19 female patients, and there was no sex difference between local and non-local patients. The average age of patients with BEBBC was 38.08 ± 2.0 years, which was significantly younger than that of patients with other flame burns (43.26 ± 0.51 years, P = 0.0340) (Table 1). The average age of non-local patients with BEBBC was also significantly younger than that of local patients with BEBBC (33.69 ± 1.91 vs. 54.23 ± 4.15 years, P < 0.0001) (Figure 3).

Average age among local and non-local patients with BEBBC. BEBBC, burns caused by electric bicycle battery chargers.
Forty-three patients with BEBBC (accounting for 68.25% of BEBBC cases and 86% of the non-local group) earned money from doing odd jobs such as making deliveries or working as a shop assistant or street vendor. Patients with BEBBC included three children (who were family members of adult other patients), with an average age, burn size, and full-thickness burn area of 3.33 ± 0.58 years, 14.67% ± 6.11% total body surface area (TBSA), and 2.33% ± 2.31% TBSA, respectively. All three children underwent surgery, and the average hospital stay was 23.5 ± 6.61 days. Eight patients (61.54% in the local group) were retired or unemployed, and most had a low income.
Among patients with BEBBC, the mean BMI was 23.98 ± 4.42 kg/m2. Six patients were obese (BMI ≥30 kg/m2), or approximately 9.5% of the total, and these patients had a higher incidence of chronic diseases such as hypertension, cardiopathy, and fatty liver. However, there was no significant correlation between BMI and inhalation injury incidence or mortality. The past medical history of patients with BEBBC showed that approximately 73.02% were healthy, with no chronic diseases. Six people had hypertension, two of whom had coronary or valvular heart diseases and one of whom had a history of cerebral infarction.
The average burn size and full-thickness burn area in patients with BEBBC was 26.41% ± 3.46% TBSA and 10.24% ± 2.19% TBSA, respectively. These were not significantly different from the average burn size and full-thickness burn area of patients with other flame burns (24.65% ± 0.65% TBSA, and 12.21% ± 0.43% TBSA, respectively). Twenty patients with BEBBC had a burn area over 30% and an average burn size of 61.40% ± 4.64% TBSA. Of patients with other flame burns, 435 had a burn area over 30% and an average burn size of 55.45% ± 1.03% TBSA. Regarding the rate of severe burns in the two populations, there was no statistically significant difference. The largest burn size in the BEBBC group was 95% TBSA and the minimum burn size was 0% TBSA, indicating that these patients only had inhalation injury and no skin lesions (Table 1).
Forty-nine patients with BEBBC were diagnosed with inhalation injury. In comparison with the group with flame burn, the incidence of inhalation injury in the BEBBC group was significantly higher (77.78% vs. 30.88%, P < 0.0001). Fourteen of the 49 patients (28.57%) underwent tracheotomy. Two patients were treated with tracheal intubation on the first or second day after injury owing to acute respiratory tract swelling, and the tracheal cannula was removed within the following 3 to 5 days.
The BEBBC group also had significantly higher mortality in comparison with the group that had other flame burns (11.11% vs. 3.40%, P = 0.0016) (Figure 4). The main cause of death was multiple organ dysfunction syndrome (MODS) in four patients with BEBBC, acute respiratory failure after severe inhalation injury in one patient, and ventricular fibrillation in one patient. One family insisted the patient be transferred to a local hospital, and the patient died of acute renal failure on the second day (Table 2). The main causes of death in patients with other flame burns are also summarized in Table 2. There was no significant difference between the two patient groups. We analyzed the characteristics of death in both groups. A quick sequential organ failure assessment (qSOFA) value of ≥2 and a revised Baux (rBaux) score of >140 are considered high risk in predicting the prognosis of patients with burn. 5 However, both groups showed no differences in qSOFA values or rBaux scores. The same was true for the rate of bloodstream infection with carbapenem-resistant Klebsiella pneumoniae (CRKP), the duration of mechanical ventilation, incidence of pneumonia, and length of hospital stay for the two groups (Table 3).
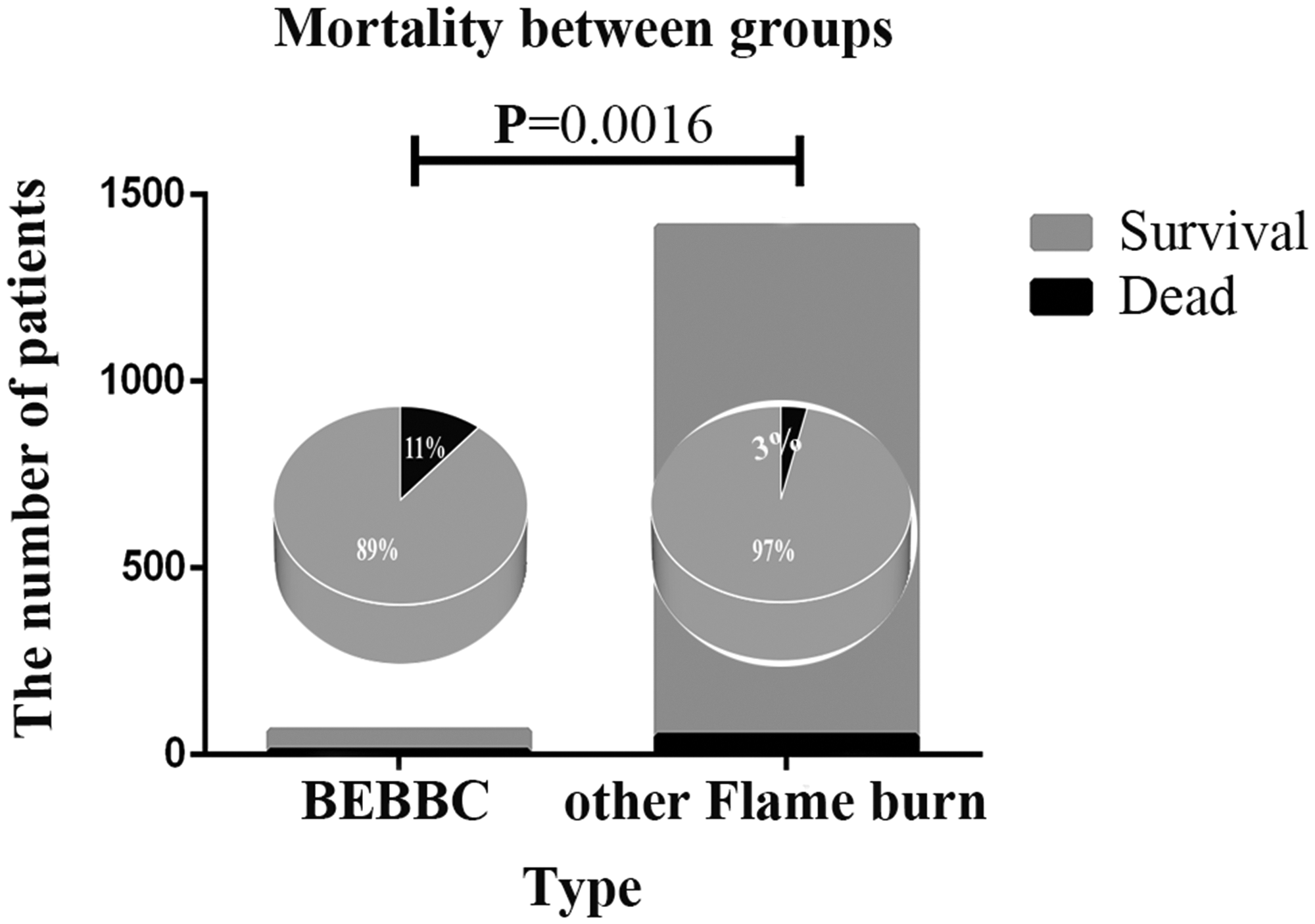
Mortality rates in the different patient groups. BEBBC, burns caused by electric bicycle battery chargers.
Causes of death in patients with BEBBC and other flame burns.

BEBBC, burns caused by electric bicycle battery chargers; MODS, multiple organ dysfunction syndrome.
All MODS cases in patients with BEBBC were caused by sepsis; 26 cases of MODS in patients with flame burn were caused by sepsis.
One patient with BEBBC died of acute renal failure. One patient with flame burn died of heart failure.
Characteristics of deaths among patients with BEBBC and those with other flame burns.

BEBBC, burns caused by electric bicycle battery chargers; qSOFA, quick sequential (sepsis-related) organ failure assessment; MODS, multiple organ dysfunction syndrome; BSI, bloodstream infection; CRKP, carbapenem-resistant Klebsiella pneumoniae; LOS, length of stay; SEM, standard error of the mean.
The average hospital stay was 23.98 ± 3.03 days in patients with BEBBC, which was not significantly different from that of patients with other flame burn. During this time, 42 patients underwent surgery, mainly including debridement and skin grafting procedures. The average number of operations was 2 ± 1. There was no difference in the number of patients who underwent surgery between the group with BEBBC and the group with other types of flame burn.
Discussion
BEBBC are a special type of flame burn. We found no difference between patients with BEBBC and those with other types of flame burn in terms of the pediatric burn proportion, sex ratio, total burn size or full-thickness burn size, length of hospital stay, or surgical intervention. However, the mortality incidence in BEBBC was 3.27 times that of other flame burns, indicating the risk of death in patients with BEBBC (11.11%) is a serious hazard. In high-income countries like Canada, mortality owing to thermal injury (including scald and flame burn) decreased from 11.3% to 2.8% between 1976 and 2015. 2 In China, mortality among people with burn aged over 60 years is 0.9%. 6 Another study based on 6325 patients with burn also showed a mortality rate of 0.9%, and risk factors included full-thickness burns, larger TBSA, and older age. 7 There was no difference between BEBBC and other flame burns in terms of the total burn size and full-thickness burn area. In comparison with patients who had other types of flame burn, patients with BEBBC were younger, on average. Additionally, most patients were healthy, with no underlying diseases. However, inhalation injury is an independent risk factor for mortality in burns. 8 The inhalation injury incidence among patients with BEBBC was 2.52 times that of patients with other flame burns. Sixteen patients with inhalation injury underwent tracheotomy or intubation owing to acute respiratory failure. If applied, an artificial airway and mechanical ventilation put patients at a high risk for ventilator-associated pneumonia, which worsens if combined with inhalation injury. 9
To reduce the incidence of BEBBC, crucial elements, including the susceptible population (“who”), frequently occurring times (“when”), and places of occurrence (“where”) must be clarified. The incidence of BEBBC and their proportion among all flame burns have gradually increased, a trend that has a close connection with social changes in recent years. The express delivery industry is booming as online shopping has become critical in the daily lives of Chinese people. China’s express delivery volume reached 63 billion pieces in 2019, and volumes in Germany and the United States are also predicted to double in the next decade. 10 Owing to the labor force demand in the express delivery industry, young workers from small cities, towns, and villages are moving to metropolises, such as Beijing and Shanghai. Considering the composition of patients with BEBBC, young non-locals engaging in delivery work and older local adults who are mainly retired constitute the principal victims, suggesting that these are the main populations requiring education on avoiding BEBBC hazards.
Regarding the occurrence time of BEBBC incidents, most took place during the night and early morning, times when most people are asleep. In this scenario, fire in combination with dense smoke require people to react quickly to escape. Awaking from sleep usually delays reaction time. Children often tend to bear the brunt of harm in a fire event. Although only three children were included in our study, all of them had moderate to severe burns according to the burn lesion size and depth. Moreover, all three children underwent multiple surgeries and had hypertrophic scarring, which place a heavy psychological burden on children and parents. 11
Obese patients (BMI ≥30 kg/m2) are likely to have impaired mobility. 12 In our study, the proportion of obese patients was approximately 9.5% of the total, and there was no evident correlation between obesity and worse outcomes, suggesting that obesity was a non-significant factor in BEBBC, based on the small sample size in the present study. However, obese patients have a higher rate of chronic diseases, 13 which might complicate medical treatment in a clinical scenario.
In terms of locations where BEBBC tended to occur, high-density residential sites were frequently involved. Young non-local individuals engaging in delivery service or temporary work usually live in lower-cost rental housing, where high-density living conditions are commonly seen. For convenient transportation for work or personal use, these individuals often use electric bicycles, which are commonly left charging in narrow common passageways on the first floor of residential This together with the presence of solid, flammable waste deposited in the same areas, increase the risk of fire. 14 The worst outcome is when a fire blocks the escape route on the first floor, hindering emergency rescue efforts.
News about BEBBC events is not uncommon throughout the year. Traditional media, such as television, radio, and newspaper, as well as social media platforms like WeChat and Weibo, are used to widely disseminate information, with a strong influence on society.15,16 Partly owing to the contribution of social media as a useful adjunct tool in developing public health policies, 17 the Safety Administrative Regulations of Non-Motorized Vehicles in Shanghai was issued and implemented on 1 May 2021. The law strictly forbids charging of non-motorized vehicles in passageways of buildings, especially on the first floor. Moreover, communities are now demanding that public charging stations be set up for non-motorized vehicles that are equipped with surveillance cameras, automatic fire alarms, and extinguishing systems.
To extend the driving distance of an electric bicycle, owners often adapt and reassemble the bicycle battery, altering the electrical circuit and sometimes the load to increase the voltage and output while riding. These batteries are usually designed to be flame retardant and the power supply is interrupted once fully charged. 18 However, with modification, the security settings are easily overridden and destroyed, which might be the primary cause of electric bicycle battery fires. Replacement batteries usually do not meet the factory-rated voltage and are therefore dangerous. Installation of such batteries is forbidden according to the Regulations of Shanghai Municipality on the Administration of Non-Motor Vehicle Safety, which strictly prohibits private modification of electric bicycle batteries.
The high rate of group burns in BEBBC incidents requires urgent attention. High-density living conditions facilitate group burns. Herein, we have not used the term “massive burn” because a mass casualty event is defined as a situation wherein the number of patients and the severity of their injuries exceed the capability of the existing facilities to deliver routine care. 19 In our experience, the maximum number of patients involved in a group BEBBC event was four, which was within the capacity of our burn unit to handle. Additional conditions to consider include patients who had already died before the arrival of emergency services and who were therefore not transferred to the hospital, or patients with slight injuries who were followed in the outpatient department instead of being admitted to the hospital. The above situations would increase the number of patients with group burn involved in this study.
We are also concerned with how best to increase the cure rate for BEBBC. The primary cause of death among patients with BEBBC was multiple organ dysfunction syndrome (MODS), and all cases of MODS in patients with BEBBC were caused by sepsis. There is evidence of pathological organism cross-colonization between burn wounds and the tracheobronchial tree. 20 The pathogenic organisms associated with mortality in our study were CRKP, carbapenem-resistant Acinetobacter baumannii, and carbapenem-resistant Pseudomonas aeruginosa. In particular, the incidence of CRKP has been increasing in recent years. CRKP infection is also an independent risk factor for patients with sepsis burn. 21
The main limitation of the present study is that this research was conducted among patients of a single burn center. However, this center is the largest burn unit in Shanghai and a Shanghai Burn Emergency Centre. Most patients with burn in Shanghai are treated at our burn unit. Further studies with a larger number of burn units and patients with BEBBC would improve the quality of this study and provide more general information to help in policymaking and medical treatment improvement to reduce the occurrence and mortality of BEBBC.
Conclusion
In this study, we identified the main characteristics of BEBBC in China, namely, high incidence at night and early morning, frequent occurrence in high-density living conditions, high frequency of group burn cases, high social impact, and high mortality (Figure 5). Greater attention is needed for the prevention and management of BEBBC. Appropriate measures include enacting legislation to prohibit battery modification and charging in fire passages of buildings; dissemination of science information to the public in high-density residential communities, especially those with a higher number of delivery service workers who use electric bicycles; and improved treatment of respiratory tract infections and gastrointestinal tract bacteria translocation. Such efforts will help to prevent BEBBC as well as increase the cure rate and reduce patient mortality owing to BEBBC.

Characteristics of burns caused by electric bicycle battery chargers (BEBBC).
Footnotes
Acknowledgements
The authors gratefully acknowledge Prof. Sun Mu and Mrs. Hu Jianlin of the Medical Record Statistical Information Department of Rui Jin Hospital for their support in data collection.
Author contributions
LQ, YL, and BY conceived the study and study design. XQW contributed to data acquisition. LQZ and BY conducted data analysis. All authors contributed to the interpretation of the data as well as manuscript writing, critical review, and final revisions. All authors had access to the data and read and approved the version to be published. All authors agreed to be accountable for all aspects of the work.
Data availability statement
Data are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was funded by the National Natural Science Foundation of China (No. 81671914, 81101433), Shanghai Municipal Key Clinical Specialty Project Fund (No. shslczdzk02302), and Shanghai General Hospital Integrated Traditional Chinese and Western Medicine Special Fund (No. ZHYY-ZXYJ-HZX-201911).