
Abstract
Objective
To evaluate a newly developed Hybiome ProGRP chemiluminescent assay.
Methods
Analytical sensitivity, precision, recovery, and equivalency of serum and plasma, serum stability, and complement interference of the Hybiome ProGRP assay were evaluated. Serum specimens from 318 individuals including 38 small cell lung cancer (SCLC), 65 non-small cell lung cancer (NSCLC), 53 benign lung diseases, and 162 healthy controls were assessed using the Hybiome ProGRP assay and Roche Elecsys ProGRP assay, and the results were compared.
Results
The Hybiome ProGRP assay showed good analytical sensitivity, precision, and accuracy, and it showed equivalence between serum and plasma and serum stability. The methodological comparison results showed good correlation between the Hybiome and Roche assays (slope, 0.9889; intercept, 1.28). Both the Hybiome and Roche assays showed good ability to distinguish between SCLC and NSCLC. Based on 95% specificity in the NSCLC cohort, a clinical differentiation cut-off for separating SCLC from NSCLC patients was 114 pg/mL for the Hybiome assay and 117 pg/mL for the Roche assay; the AUC was 0.9166 and the sensitivity was 71.05% for Hybiome and 0.9045 and 76.32% for Roche, respectively.
Conclusion
The Hybiome ProGRP chemiluminescent assay shows good analytical performance and good correlation with the Roche Elecsys ProGRP assay.
Keywords
Introduction
Tumor markers are extensively used to determine the diagnosis and prognosis of cancer patients. Lung cancer is the most common cancer worldwide, accounting for an estimated 2.09 million incident cases and 1.76 million deaths in 2018 (Data source: GLOBOCAN 2018). Lung cancer is classified into two major entities depending on the cell type: small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC). SCLC accounts for up to 15% of all new lung cancer cases and differs biologically from NSCLC by the presence of neuroendocrine differentiation and a higher rate of tumor growth. 1 Carcinoembryonic antigen (CEA), cytokeratin 19 fragment (CYFRA21-1), and squamous cell carcinoma antigen (SCCA) are commonly used in NSCLC treatment monitoring.2–4 Neuron-specific enolase (NSE) and pro-gastrin-releasing peptide (ProGRP) have been shown to be good tumor markers in SCLC. ProGRP has better sensitivity and specificity compared with NSE and it is rarely elevated in other malignant diseases or in benign conditions.5–8 Therefore, ProGRP is considered to be an ideal tumor marker for SCLC.9,10
Gastrin-releasing peptide (GRP) is a gut hormone that is often produced by SCLC cells, so it can be helpful in diagnosing patients with SCLC. 11 However, GRP was not suitable for a clinical diagnosis because of its poor stability in specimens. ProGRP is a precursor of GRP that consists of GRP residues 1 to 27, residues 28 to 30 (a cleavage site), residues 31 to 98 (a constant region), and a variable carboxy-terminal region. Three types of human ProGRP were found in SCLC cells, with 115, 118, and 125 amino acids. 12
The ProGRP immunoassay was originally developed in Japan in 1995 as an enzyme-linked immunosorbent assay using monoclonal and polyclonal antibodies. A fully automated and highly sensitive assay was launched by Abbott in 2009, which used a double monoclonal antibody assay with acridinium chemiluminescent paramagnetic technology. 13 However, ProGRP levels fluctuated when serum specimens were tested using this method. Only plasma specimens were recommended in this assay, which limited the combined use of NSE and ProGRP because NSE should be tested only in serum. 14 PerkinElmer then developed a novel, highly sensitive time-resolved immunofluorometric assay (TR-IFMA), 15 and Roche Diagnostics GmbH launched a new quantitative ProGRP assay (the Elecsys® ProGRP assay). 16 Both the TR-IFMA and Elecsys assays are applicable for serum and plasma tests.
Here, we evaluated the technical and clinical performance of a new acridinium-labeled chemiluminescent ProGRP immunoassay that was developed by a Chinese IVD manufacturer (Suzhou Hybiome Biomedical Engineering Co., Ltd.), which is abbreviated “Hybiome”, and it includes precision, specimen stability, complement interference, method comparison, and differentiation potential for SCLC from NSCLC.
Materials and methods
Immunoassays
The Hybiome ProGRP assay
Hybiome ProGRP assay (Suzhou Hybiome Biomedical Engineering Co., Ltd., Suzhou, China) is a one-step immunoassay that uses streptavidin-coated magnetic beads and a chemiluminescent label for quantitative determination of ProGRP in both serum and plasma. ProGRP is recognized by a biotin-labeled monoclonal antibody E149 at amino acids of 48 to 52 and an acridinium-labeled monoclonal antibody E146 at amino acids of 57 to 61. The complex is then captured by streptavidin-coated magnetic beads (Figure 1).

Format of the Hybiome ProGRP assay.
Briefly, 50 µL of sample is incubated with 100 µL of biotinylated antibody and 100 µL of acridinium-labeled antibody for 10 minutes to form immune complexes in the presence of ProGRP. Then, 20 µL of streptavidin-coated magnetic beads are added, and the immune complexes bind to the magnetic beads via biotin–streptavidin interaction. Unbound substances are cleared away by washing in a magnetic field. Finally, H2O2-induced luminescence is measured by a photomultiplier and the ProGRP level in the samples is calculated based on a standard curve. The whole process takes 30 minutes. The assay is standardized against the Roche Elecsys ProGRP assay.
The control assay was the Elecsys ProGRP assay (Roche Diagnostics GmbH, Penzberg, Germany), which is a one-step electrochemiluminescence quantitative immunoassay with two monoclonal antibodies and it is suitable for both human serum and plasma tests. The binding epitopes of Elecsys ProGRP assay are the same as those in the Hybiome assay.
Specimens sources and handling
This study was approved by the Ethics Committee at the First Affiliated Hospital of USTC. Certain kinds of specimens were obtained with written informed consent.
Serum specimens (no hemolysis, fat blood, and jaundice) were collected from 318 individuals, including 162 healthy controls, 53 with benign lung diseases, 38 SCLC patients, and 65 NSCLC patients. The donors comprised 178 males and 140 females, between 23 and 92 years old. All cases of SCLC and NSCLC were diagnosed histologically, and no further histological type selection criteria were used.
Samples collected were frozen and stored below −20°C. The frozen samples were thawed in a water bath and centrifuged at 1000 rpm for 3 minutes before the tests. Repeated freeze-thaw cycles were avoided.
Statistical analyses
Correlation analysis was performed to compare the two assays. ROC was used to evaluate the ability of the two immunoassays to distinguish between SCLC and NSCLC, and optimal cut-off values were determined for each assay. The values of the spiked ProGRP specimens were measured on different days and were compared using a paired t-test. The differences were considered to be significant when p < 0.05. All statistical analyses were performed based on the software GraphPad Prism 7.0 (GraphPad Software Inc., La Jolla, CA, USA).
Results
Technical assessment
The average analytical sensitivity with three lots of reagents was 1.85 pg/mL and it ranged from 1.426 to 2.042 pg/mL.
Overall results for the Hybiome ProGRP assay coefficient of variation (CV) that was evaluated over 20 days are shown in Table 1. The total precision ranged from 4.3% to 5.2%, within-run precision ranging from 2.2% to 3.5%.
Within-run and total precision of the Hybiome ProGRP assay.

ProGRP, pro-gastrin-releasing peptide; SD, standard deviation; CV, coefficient of variation.
The calculated recovery of the Hybiome ProGRP assay when using a high-titer serum sample was spiked into five normal healthy serum samples is shown in Table 2. The average percent recovery was 96.16% and ranged from 90.6% to 105.2%.
Recovery of ProGRP in spiked serum.

ProGRP, pro-gastrin-releasing peptide.
The correlation between serum and EDTA plasma in the Hybiome ProGRP assay was shown in Figure 2. The correlation equation is y = 1.0239x + 0.5213, with a correlation coefficient of 0.9922. The results indicated that there was good equivalency between serum and plasma samples.

Correlation of ProGRP levels between the paired serum and EDTA plasma samples.
The sample stability and complement interference were evaluated in the same experiment, and these results are shown in Figure 3. From day 0 to day 4, serum ProGRP levels showed good stability, with no obvious fluctuations. The ProGRP levels were not significantly different between different days using a paired t-test, which suggested that there was no complement inference in these 25 normal serum specimens and all of these serum specimens were stable for at least 96 hours.
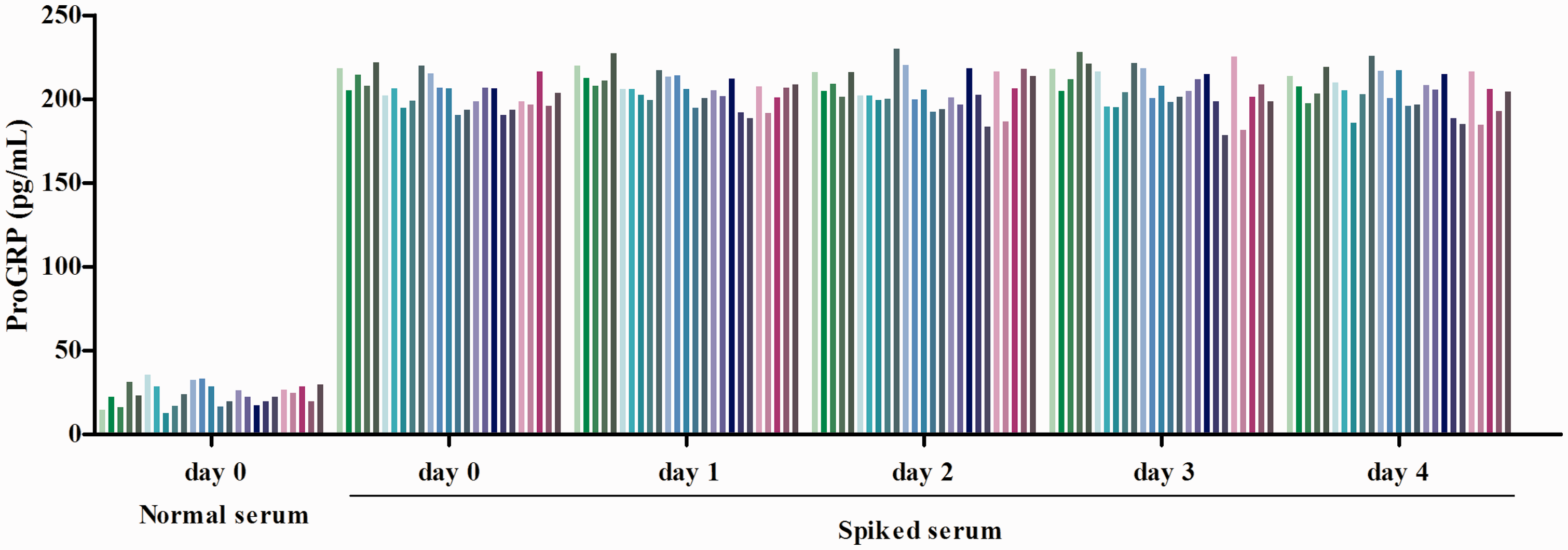
Serum stability at 2 to 8°C and complement interference. Each of the 25 fresh normal serum samples were spiked with a certain amount of high-level ProGRP serum, which was aliquoted and stored at 2 to 8 °C. One aliquot was analyzed from day 0 to day 4. Values of the spiked serum that was measured on different days were compared using a paired t-test, and all results were not statistically significant.
Methodological comparison
The methodological comparison results between the Hybiome and the Roche Elecsys ProGRP assays with 318 serum samples is shown in Figure 4. The slope and intercept were 0.9889 and 1.28, and the correlation coefficient was larger than 0.99.

Correlation between the Roche Elecsys and Hybiome ProGRP assays.
ProGRP levels were evidently higher in the SCLC group compared with the other three groups (Table 3). In the SCLC group, the ProGRP values were up to 11,134 pg/mL (Hybiome) and 11,205 pg/mL (Roche). In the healthy control group, the highest ProGRP value that was obtained was 168 pg/mL (Hybiome) and 157 pg/mL (Roche). In the benign lung disease group, the highest measured values for ProGRP were 167.5 pg/mL (Hybiome) and 102.4 pg/mL (Roche). In the NSCLC group, the highest ProGRP value was 231 pg/mL (Hybiome) and 244.6 pg/mL (Roche).
Distribution of ProGRP levels in healthy controls, NSCLC, SCLC, and patients with benign lung diseases using the Roche and Hybiome assays.

ProGRP, pro-gastrin-releasing peptide; NSCLC, non-small cell lung cancer; SCLC, small cell lung cancer (SCLC).
Both the Roche and Hybiome ProGRP immunoassays showed a clear differential diagnosis between SCLC and NSCLC, as shown in Figure 5. Based on the ROC curve, a clinical differentiation cut-off for separating SCLC from NSCLC was 114 pg/mL for Hybiome and 117 pg/mL for Roche. The AUC and sensitivity were 0.9166 and 71.05% for Hybiome and 0.9045 and 76.32% for Roche, respectively, based on the 95% specificity in the NSCLC cohort.

ProGRP ROC curves for SCLC (n = 38) compared with NSCLC (n = 65) for Roche and Hybiome assays.
Discussion
ProGRP is a promising tumor marker for SCLC, and it has been increasingly used in the clinic. Several new immunoassays have been developed and reported in studies over the last few years. Here, we performed an evaluation study of the newly developed Hybiome ProGRP immunoassay to assess its analytical performance and compared this method with a well-established Elecsys ProGRP immunoassay.
The results of evaluation studies for the Hybiome ProGRP assay showed good analytical sensitivity, precision, and accuracy. Within-run imprecision ranged from 2.2% to 3.5% and total imprecision values ranged from 4.3% to 5.2%, which was comparable with data reported on the ARCHITECT ProGRP assay and Elecsys ProGRP assay.13,16 Good precision (CV<8%) was mainly a result of using a streptavidin–biotin solid phase separation system, which has been historically applied in many immunoassays such as in the Elecsys series.
In a previous study, serum ProGRP levels decreased over time with the ARCHITECT assay, 14 and differing results were obtained using plasma or serum samples, while other kits, such as the Roche Elecsys and PerkinElmer TR-IFMA, showed consistent test results in serum and plasma. The Hybiome ProGRP assay performed equivalently in serum and EDTA plasma tests, and in a similar manner as the Roche Elecsys and PerkinElmer TR-IFMA assays. It is suspected that amino acid residues 75 to 83 of the ProGRP can be cleaved by thrombin that is generated during the clotting process in serum rather than in plasma.14,17 Because the Elecsys ProGRP assay and the PerkinElmer TR-IFMA use two monoclonal antibodies that bind to epitopes that are relatively resistant to endoproteolytic cleavage, ProGRP levels in serum can be stable for several days, as shown by these two assays. The Hybiome ProGRP assay used two of the same monoclonal antibodies as the Roche and PerkinElmer assays, as follows: E146 (aa 48–52) and M16 (aa 57–61).16,18 The identity of the main active materials lays a good foundation for the results to be consistent between the Hybiome and Roche Elecsys ProGRP and also for serum stability.
Complement interference is a general phenomenon in solid phase immunoassays, which mainly leads to falsely lower results. 19 Because solid-phase bounded antibodies can activate complement, binding of C1q to the activated antibodies further activates the complement pathway and leads to deposition of several complement factors onto the solid surface. These deposited complement factors sterically hinder the interaction between antigen and antibody on the solid surface and, thus, cause falsely lower results. In a rare situation, false-positive results happen because complement links solid phase and labeled antibodies together. 20 Elimination of assay interference should be a priority for manufacturers, and there are many cases reported, especially for solid phase immunoassay platforms such as TR-IFMA and VIDAS.20,21 Because complement C1 is calcium-dependent, adding a chelating agent (e.g. EDTA) can eliminate complement-related interference. However, EDTA is not suitable for use when it can affect the system. In such cases, other methods should be used, such as Fab that is added to eliminate the influence of complement in the TR-IFMA assay. In the experiment of complement interference and serum stability, we found that there was no complement interference in the Hybiome ProGRP assay and that serum is stable for 4 days at 2 to 8°C (Figure 3).
The Hybiome ProGRP assay shows good correlation with the Roche Elecsys ProGRP assay (shown in Figure 4; slope, 0.9889; correlation coefficient, 0.99), which is better than the correlation between the Fujirebio and ARCHITECT (slope, 0.93; correlation coefficient, 0.99), 13 and similar to the relationship between the ARCHITECT and Elecsys ProGRP assays (slope, 1.02; intercept, −2.72 pg/mL). 16
Distinguishing between SCLC and NSCLC is very important clinically because the differences in the prognosis and treatment for these two types of cancer. As shown in Figure 5, the Hybiome ProGRP assay has 71.05% sensitivity (AUC, 0.9166) and the Roche Elecsys ProGRP assay has 76.32% sensitivity (AUC, 0.9045) at a fixed specificity of 95% in NSCLC. These results are consistent with previous reports on the Roche Elecsys ProGRP assay (sensitivity, 78%; AUC, 0.94) and the PerkinElmer TR-IFMA assay (sensitivity, 78%; AUC, 0.89).15,16
In conclusion, the Hybiome ProGRP chemiluminescent assay shows good analytical performance and favorable correlation with the Roche Elecsys assay.
Abbreviations
ProGRP, pro-gastrin-releasing peptide; SCLC, small cell lung cancer; NSCLC, non-small cell lung cancer; CEA, carcinoembryonic antigen; NSE, neuron-specific enolase; SCCA, squamous cell carcinoma antigen; TR-IFMA, time-resolved immunofluorometric assay