
Abstract
We report development of an aneurysmal bone cyst (ABC) that was located in the proximal region of the femur in an 11-year-old girl. Over a period of 30 weeks, the ABC showed fulminant local progression, with destruction of the bone, which led to an abrupt loss of function of the left hip. The standard tumour treatment protocol was followed. We performed embolisation of the tumour followed by a biopsy, which confirmed the diagnosis of ABC. The outcome was negative with total destruction of the proximal third of the femur, despite repeating the embolisation. Because of the unfavourable local progression, a second biopsy was performed and we reconfirmed the initial diagnosis. The final decision regarding the therapeutic approach was total hip arthroplasty with femoral reconstruction with a prosthesis. Following this treatment, the patient’s outcome was favourable, with complete recovery of function and no local relapse.
Keywords
Introduction
Aneurysmal bone cyst (ABC) is an osteolytic benign tumour, which is usually situated in the metaphysis of long bones and mostly encountered in patients younger than 20 years old. 1 The structure of this tumour is poorly organised, with vascular gaps separated by fibrous membranes composed of fibroblasts, giant multinucleate cells, and osteoclasts, which represent a multi-chamber aspect.1,2 The cells in ABC have an osteoclast-like phenotype (CD51+, CD14−, cathepsin K+, TRAP+) and are responsible for lacunar resorption 3
Most ABCs are diagnosed during childhood or adolescence. 4 Most causes of ABC are unknown and are usually discovered by accident, following some type of trauma. If ABC has a large dimension, it tends to deform the anatomy of the affected region. When the aneurysmal cyst is increased in volume, the main symptom may be nonspecific pain in the concerned area. All bones can be affected by this pathology, but the proximal femur is most frequently involved. 5 From a histopathological point of view, ABC can be classified into three types: conventional (vascular) type, which is a rapidly growing, extensive, damaging lesion, leading to cortical breach and soft tissue aggression; solid type, and a third mixed type of the other two types. 6
The most commonly used radiological investigation for ABC is plain radiography. Radiography often reveals an extensive tumour-like osteolytic lesion, located in the metaphyseal area of the long bones, with no invasion of the growth cartilage, and is well separated from the adjacent soft tissues. 7 Magnetic resonance imaging scans regularly show an extensive tumour with eccentric osteolysis and a polylobulated aspect with fluid-fluid levels. 6 The differential diagnosis for an aneurysmal cyst can be essential bone cyst, giant cell tumour, osteoblastoma, and telangiectatic osteosarcoma. 2 A biopsy is mandatory for an aneurysmal cyst because telangiectatic osteosarcoma needs to be considered as a differential diagnosis.
The classic procedure for ABC is a direct approach with opening of the cyst and its curettage. However, because of the high recurrence rate associated with this type of treatment (11–31%), 8 local adjuvant therapies are added to the procedure. These therapies include surgical cryotherapy, 9 alcohol sclerotherapy, 10 selective arterial embolisation, 11 and use of denosumab. 12 Denosumab is an innovative therapeutic approach, which inhibits osteoclast function, and can have positive effects on the development of ABCs. The purpose of treatment is to stop extension of the lesion, prevent pathological bone fractures, reduce relapse, and most importantly, stop pain. 1
This case report describes the aggressive development of an ABC in a paediatric patient. Regardless of the initial treatment, the outcome was unfavourable, which led to use of a mega-prosthesis for replacing the tumour.
Case presentation
We report a case of an 11-year-old girl who presented to the Emergency Department for diffuse pain of the left hip after a fall. Her medical and family history was unremarkable. A clinical examination showed mild, diffuse swelling of the left hip. The swelling was firm and non-tender, with moderate to severe painful manipulation. This was associated with pain-related decreased mobility of the hip. The patient was unable to walk. Plain radiography of the left hip in the frontal and lateral views showed an extensive osteolytic lesion in the proximal metaphyseal femur and femoral neck with thin sclerotic margins, with no invasion of the growth plate (Figure 1). Magnetic resonance imaging and a computed tomography (CT) scan of the hip showed the presence of an ABC in the proximal third of the left femur, with no extension in the adjacent soft tissue. Selective arterial embolisation was performed to devascularise the tumour, promote healing, and decrease the risk of high bleeding during the biopsy procedure. For this purpose, absorbable gelatine sponge particles were used. A biopsy was achieved through a lateral approach centred on the greater trochanter. A hole was drilled at the inferior pole of the cyst, thus reaching the haemorrhagic lesion where blood and cystic soft tissue were obtained for a histopathological exam. After the diagnosis was confirmed, we performed a second selective arterial embolisation to limit development of the ABC. The patient’s progress was favourable, with decreased local pain, and she gradually regained mobility.

X-ray of the pelvis in the anteroposterior view showing an extensive lytic lesion that is located in the left femoral neck with thin sclerotic margins, with no invasion of the growth plate
One month later, local progression of the ABC was favourable. Radiographic findings showed osteosclerotic margins at the tumour site. Pain in the left hip was further diminished and the full range of motion was regained. At the 8th and 12th weeks of check-up, plain radiography was performed and showed no progression of the bone cyst. After approximately 16 weeks, the patient experienced moderate local pain. An X-ray showed that the osteolytic process was expanded (Figure 2). A second biopsy was performed to exclude a potential malignant diagnosis, which could have been missed. A biopsy specimen was also sent to another histopathological diagnosis centre and the initial diagnosis was reconfirmed (ABC vascular type). Furthermore, progression of ABC was unfavourable. Massive growth of the lesion had resulted in total destruction of the proximal third of the femur. The lesion expanded from the growth plate to 1 cm distally of the lesser trochanter, with severe local pain and functional impairment. Three-dimensional CT reconstruction showed massive destruction of the proximal left femur (Figure 3).
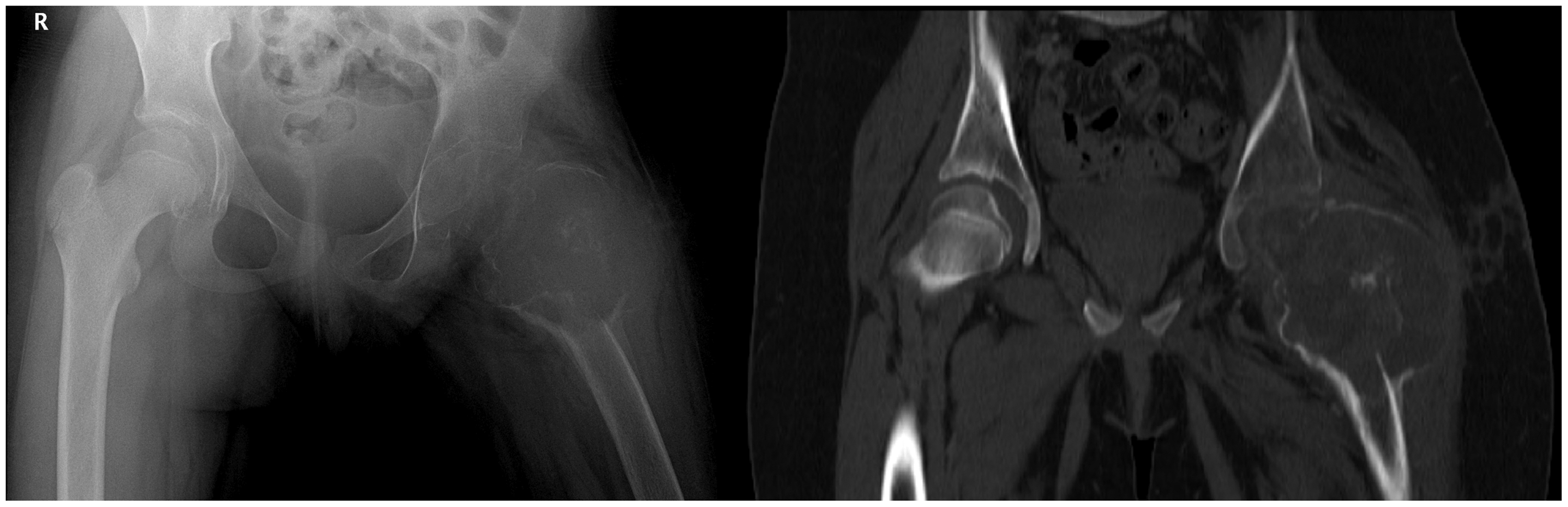
Progression of the lesion after 16 weeks. (a) Anteroposterior view of the pelvis shows massive extension of the osteolytic process with total destruction of the left femoral neck. (b) Non-contrast computed tomography of the proximal femur shows lytic lesions involving the epiphysis and metaphysis with no invasion of the adjacent soft tissue.
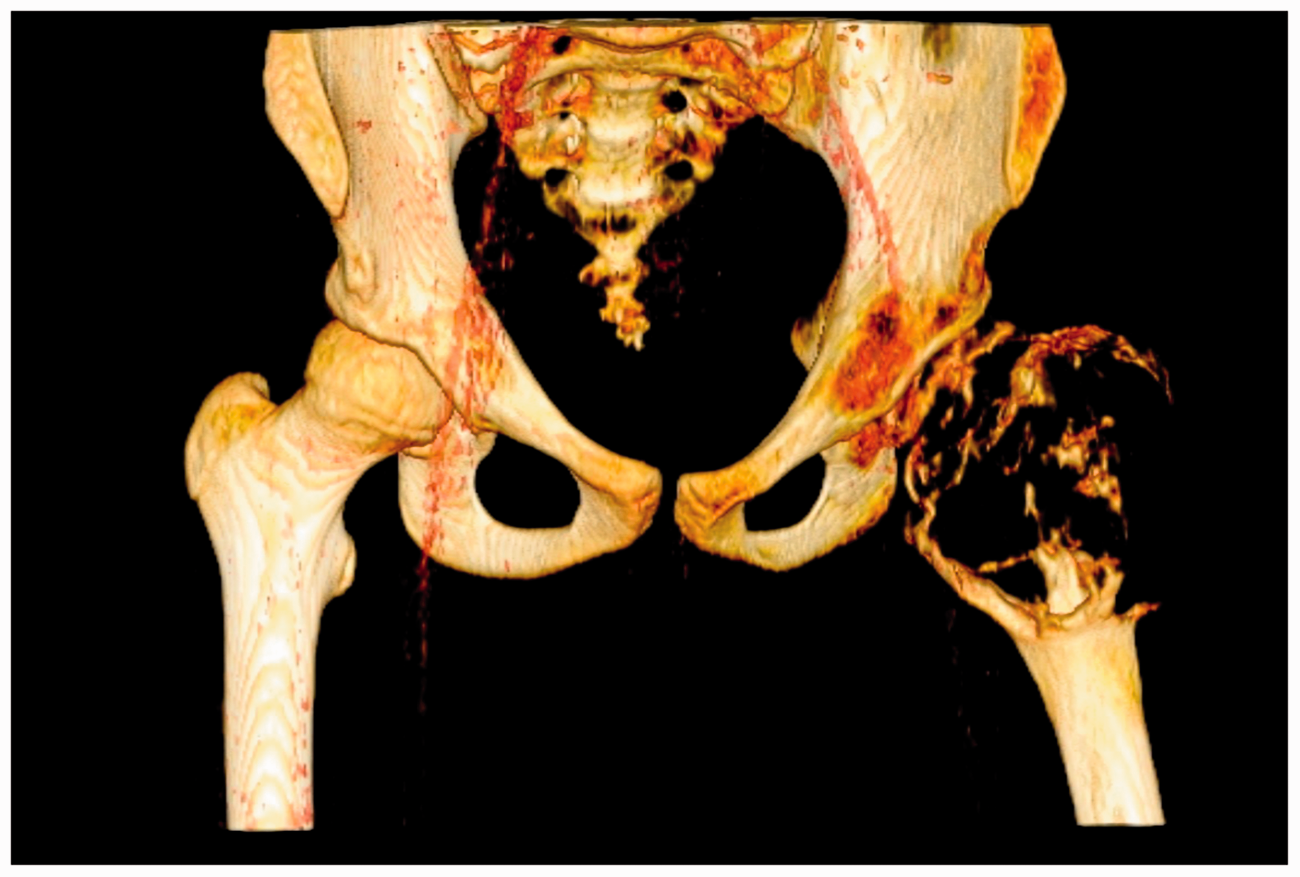
Three-dimensional computed tomography reconstruction of the hip affected by aneurysmal bone cyst
Before surgical treatment, a CT scan showed disappearance of the cortical wall and differentiation of the cyst from the adjacent soft tissue by a fibrous membrane. We injected contrast agent to confirm under fluoroscopy that the cystic walls were breached. Unfortunately, the cyst communicated with the surrounding soft tissues. Therefore, sclerotherapy was contraindicated.
Considering the fulminant evolution of the lesion throughout 8 months (Figure 4), we decided to perform radical treatment for the tumour. We chose to excise the tumour (Figure 5). We used a reconstructive prosthesis of the proximal femur and total hip arthroplasty. The resection was wide, reaching approximately 2 cm distally to the inferior pole of the cyst. The implant had to insure the possibility of needing to reinsert the local muscular structures. For hip arthroplasty, we used a total uncemented prosthesis. The acetabular cup was attached without a requirement for any particular preparation of the acetabulum.

X-ray anteroposterior view of the femoral neck showing development of aneurysmal bone cyst. (a) First admission to hospital and diagnosis. (b) Progression after 8 weeks. (c) Extension of the osteolytic lesion after 16 weeks. (d) Anteroposterior view after resection and reconstruction.

Intraoperative photographs showing the macroscopic appearance of the lesion. A resected specimen is shown in panels A, B, and C.
At the 3rd week of follow-up, the patient’s recovery was favourable and passive movement of the left hip was regained. Eight weeks later, the full range of motion and full weight-bearing were achieved (Figure 6). The 1-year follow-up showed good progress with total recovery of function, no local pain, and total weight-bearing.

Post-reconstruction X-ray of the pelvis shows total hip arthroplasty with a tumour prosthesis.
The patient provided verbal consent for inclusion in this report. Approval for this report from the ethics committee was not required.
Discussion
Although the initial treatment of our patient was in accordance with surgical protocols, development of the ABC was atypical. In our case, there was rapid progression of the lesion, leading to massive bone destruction. Acute pain experienced by the patient was resilient to medication and there was total loss of function.
Block resection has the best outcome and the lowest rates of relapse for ABC, providing the best control over the lesion. However, this method has the highest morbidity rate because of intra- and postoperative complications, such as massive haemorrhage, a high risk of infection, post-resection persistent pain, shortening of the limb, growth defects, and muscular hypotonia. 13 Considering the high risk of local complications associated with open surgery,14,15 many surgeons choose less invasive techniques, such as sclerotherapy and embolisation.16,17
Embolisation is a minimally invasive technique that devascularises the tumour. Embolisation can promote healing of the tumour and reduce intra- and postoperative complications of open surgery, offering the surgeon a better approach in cases of total resection. 18 Embolisation for ABC has a recurrence rate of 39% to 44% associated with cysts that are larger than 5 cm. Repeated embolisation can have favourable outcomes in recurrent lesions. In our case, the lesion persisted and became more aggressive, even though it had favourable progression for a while after repeated embolisation. This finding is in contrast to similar cases where repeated embolisation of ABC led to a successful outcome.19,20 Rossi et al. 8 showed that 102 patients with ABC treated by selective arterial embolisation with N-2-butyl-cyanoacrylate had a healing rate of 81.8% and a complication rate of 4.5%. They also concluded that, to be effective, this procedure must be performed by an experienced practitioner with good technical skills.
Sclerotherapy is a minimally invasive therapeutic procedure for ABC with good long-term results. This therapy slows development of the cyst and also lowers the risk of relapses. The most commonly used substances for sclerotherapy are Ethibloc, 9-Aetoxisclerol, doxycycline, pure alcohol in a liquid or gel state, and liquid nitrogen. 9 Considering the high risk of soft tissue necrosis due to pure alcohol, this procedure is not indicated in cases where imaging data reveals a cortical break. 21 In our case, three-dimensional CT reconstruction indicated cortical breakage, which was confirmed intraoperatively by fluoroscopic imaging after administrating a contrast-enhancing agent.
With regard to the standard treatment for ABC, reconstruction of the affected area with a tumour prosthesis of the femur and total arthroplasty of the hip is infrequent. This method is reserved for aggressive malignant tumours with a fulminant evolution. The reason for postponing resection of the tumour mass is its location. This situation is common and has specific challenges. 22
In paediatric patients, finding implants that have the right size for the age group is difficult. Additionally, development of a discrepancy in lower limb length during growth leads to a series of re-interventions on the implant to elongate it.23,24 Because of the small size of paediatric patients, they would benefit from a custom-made endoprosthesis. Additionally, in pathologies where removal of large portions of the skeletal structure is required, a customised implant would be a possible solution. Unfortunately, we do not have this therapeutic option in our clinic.
The system that we used in our patient was a modular system that enabled the femoral component to be extended. Therapeutic management started with a minimally invasive approach, attempting to conserve the bone capital and trying to avoid complications associated with open surgical techniques. Successive embolisation excluded the possibility of using a vascular bone graft because of insufficient arterial sources for grafting. In our patient, total arthroplasty of the hip was preferred over bipolar hemiarthroplasty. The reason for this is because, in paediatric patients, occurrence of laminar coxitis is frequent, and revision of the implant might be required in the near future with rehabilitation. 25 Dysplasia, which appears in the remodelling phase, can produce supero-external migration of the prosthesis and muscular imbalance between the hip’s adductors and abductors. 26 In a study on 111 patients who underwent total hip replacement before 20 years old, the 10-year survival rate (without revision) was 70%, and the complications of osteolysis and atrophy were observed. 27
Conclusions
The therapeutic plan that was applied to our patient was in accordance with the latest treatment protocols of minimally invasive techniques of embolisation. However, the unfavourable outcome of our patient led to block resection and prosthetic replacement as a final solution. Repeated embolisation can achieve local tumour control, even in ABCs that show progression after the first embolisation. However, in the present case, severe local symptomatology and massive destruction of the proximal third of the femur led to a radical therapeutic approach.
Even though there is a standard treatment protocol for ABC, which uses a minimally invasive procedure, treatment should be individualised for each patient. This is especially the case with aggressive local progression of the tumour that disturbs the patient’s function and quality of life for a long time. A radical therapeutic approach prevents the risks of local recurrence and pathological fractures.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.